Resolution
The restoration of tissue homeostasis is the desired outcome of an inflammatory process. Lipid mediators, such as lipoxins and resolvins, limit the influx of neutrophils (Serhan et al., 2008b; Lee & Surh, 2012).
Lactoferrin from apoptotic neutrophils also reduces neutrophil infiltration, promotes the influx of M2 macrophages, and interacts with fibroblasts to promote wound healing (Takayama & Aoki, 2012).If inflammation persists, negative systemic effects of unchecked inflammatory mediators can be seen. Cachexia is a serious side-effect of chronic inflammation that leads to an overall loss of fat and muscle. Cachexia is due to prolonged release of TNFα, IL-1, IL-6, and IFNγ (Argiles et al., 2012). TNFα (cachectin) prevents adipocyte differentiation and synthesis of enzymes needed to make triglycerides by inhibiting lipoprotein lipase in nonadipose tissues and preventing fat absorption from the gut. Skeletal muscle atrophy, which is observed in cachexic animals, is likely due to the inhibition and proteolysis of protein synthesis mediated by NO and/or TNF. Osteoporosis also occurs in longstanding inflammation as a result of osteoclast stimulation by cytokines.
Systemic inflammatory response syndrome (SIRS) is an excessive inflammatory response that can lead to organ failure. It is a possible complication of bacterial sepsis and some viral infections. It can also be caused by massive tissue injury (e.g. trauma, tumor lysis syndrome). Clinical signs associated with SIRS include tachycardia, tachypnea, and generalized peripheral vasodilation, which may progress to septic shock and multiple organ dysfunction syndrome. The diagnostic criteria used to diagnose SIRS in dogs and cats are indicated in Table 2.3; two of the listed abnormalities must be present (Hauptman et al., 1997; Brady et al., 2000).
Table 2.3 Criteria for diagnosis of systemic inflammatory response syndrome (SIRS).
At least two of the indicated abnormalities must be observed to diagnose SIRS| Factor | Dogs | Cats | |
| Temperature (°F [°C]) | >102.6 [39.2] or 103.5 [39.7] or 120 | >225 or 20 | >40 |
| Leukocyte count (cells/μl) | >16,000 or 19,500 or 3 | >5 |
Classification of inflammation
Often, diagnosis of the cause of inflammation is sought several days after the initial injury has occurred. Cytologically, inflammatory processes are classified by the cell types present in the lesion. The differential diagnoses typically associated with each category of inflammation are summarized in Table 2.4.
Table 2.4 Category of inflammation and selected associated differential diagnoses
| Type of inflammation | Duration of injury | Differential diagnoses | |
| Infectious | Noninfectious | ||
| Suppurative | Acute | Bacterial | Traumatic; immune-mediated |
| Eosinophilic | Acute | Parasitic | Allergic; paraneoplastic |
| Granulomatous | Chronic | Fungal; bacterial (often atypical forms) | Foreign body |
| Pyogranulomatous | Chronic | Fungal; bacterial (chronic or atypical) | Foreign body; chronic suppurative processes |
| Lymphocytic/plasmacytic | Chronic | Viral | Vaccination; insect bite |
Suppurative inflammation
Suppurative (purulent, neutrophilic) inflammation is predominated by neutrophils. Degenerate neutrophils with karyolytic chromatin are associated with bacterial or fungal infection (Figures 2.32, 2.33). Nondegenerate neutrophils are suggestive of a sterile inflammatory process, but infection may still be occurring (Figures 2.34, 2.35). Causes of sterile inflammation include immune-mediated disease, caustic injury, and trauma.
Karyorrhectic and pyknotic neutrophils are observed in chronic inflammatory processes (Figures 2.36, 2.37). 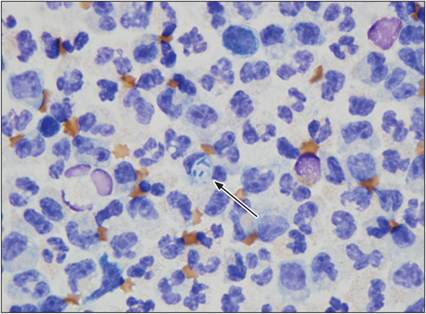
Figure 2.33 Suppurative inflammation with degenerate neutrophils and bacterial sepsis. Cytocentrifuged abdominal fluid from a 16-year-old, spayed female Bulldog. Neutrophils are the predominant cell type. Most neutrophils are degenerate; they have a pale, swollen nucleus with more open chromatin than neutrophils in a peripheral blood smear. Bacterial rods are contained within a cytoplasmic vacuole of a neutrophil (arrow) (Wright–Giemsa, 1,000? magnification).
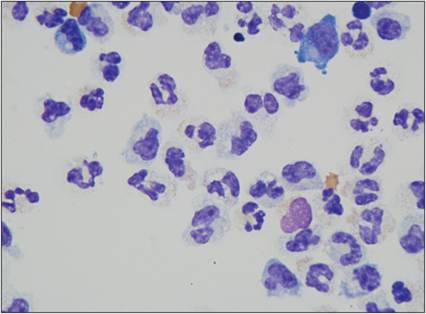
Figure 2.32 Suppurative inflammation with degenerate neutrophils. Direct smear of abdominal fluid from a 16-year-old, spayed female Bulldog. Neutrophils are the predominant cell type. Most neutrophils have a pale, swollen nucleus with more open chromatin than neutrophils in a peripheral blood smear, which indicates that they are degenerate (Wright–Giemsa stain, 1,000? magnification).
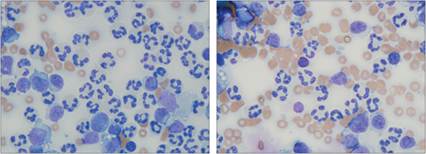
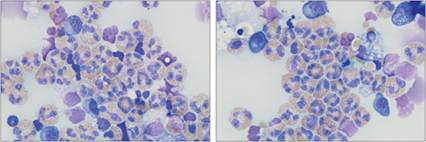
Figures 2.34, 2.35 Suppurative inflammation with nondegenerate neutrophils. Synovial fluid from an 8-year-old, neutered male Labrador Retriever. Several neutrophils and lower numbers of large mononuclear cells are present. Neutrophils are nondegenerate; they have segmented nuclei with crisp edges and dense chromatin, similar to neutrophils in a peripheral blood smear. Moderate numbers of erythrocytes are present in the background (Wright–Giemsa stain, 1,000? magnification).
Figures 2.36, 2.37 Pyknotic cells. Synovial fluid from a 3-year-old, spayed female mixed-breed dog.
The sample has a thin, stippled, eosinophilic background consistent with joint fluid of decreased viscosity. Each image has a cell with a small, round, very dense nucleus undergoing pyknosis (Wright–Giemsa, 1,000? magnification).
Eosinophilic inflammation
Lesions with eosinophilic inflammation contain >10% eosinophils (Figures 2.38, 2.39). Differential diagnoses for these lesions include parasitic, allergic, and immune-mediated diseases as well as paraneoplastic conditions and type I hypersensitivity reactions. Also, eosinophilic granuloma is a differential in cats that have a raised, erythematous mass with alopecia.
Figures 2.38, 2.39 Eosinophilic inflammation. Cytocentrifuged abdominal fluid from an 8-year-old, spayed female domestic shorthair cat with a history of vomiting and hypoalbuminemia. A thickened gastrointestinal wall and peritoneal effusion were detected ultrasonographically. Eosinophils are the predominant cell type. There are also low numbers of macrophages and plasma cells. Two small lymphocytes are present in 2.38 (Wright–Giemsa, 1,000? magnification).
Granulomatous inflammation
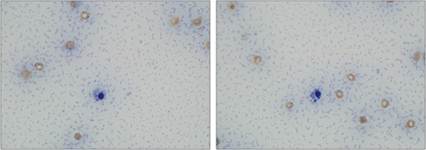
There are large numbers of macrophages in lesions with granulomatous inflammation. Multinucleated giant cells are often seen (Figures 2.40, 2.41). Foreign body reaction, fungal infection, atypical bacterial infection, and chronic irritation should be considered if granulomatous inflammation is diagnosed.
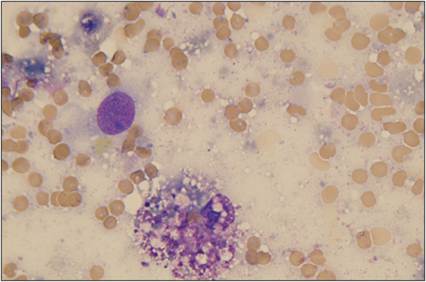
Figure 2.40 Granulomatous inflammation. FNA from a subcutaneous mass on the shoulder of a 3-year-old, spayed female domestic shorthair cat. A reactive macrophage (lower center) and a partially lysed cell (upper left) are shown. The macrophage has abundant, vacuolated cytoplasm and a round, eccentrically located nucleus with clumped chromatin (Wright–Giemsa, 1,000? magnification).
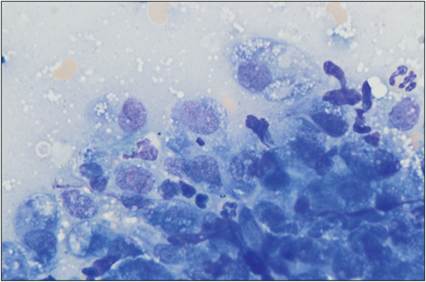
Figure 2.41 Granulomatous inflammation. FNA of a subcutaneous mass from a dog. There is an aggregate of macrophages with basophilic cytoplasm, small distinct cytoplasmic vacuoles, and a stippled nucleus. Often, macrophages that are arranged this closely together are termed ‘epithelioid macrophages’. Low numbers of neutrophils also are present (Wright–Giemsa stain, 1,000? magnification).
Pyogranulomatous inflammation
When a mixed population of macrophages and neutrophils is present, the lesion is described as pyogranulomatous (Figures 2.42, 2.43). As with granulomatous inflammation, the differential diagnoses include foreign body reaction, fungal infection, atypical bacterial infection, and chronic irritation. Close evaluation of the sample for fungal organisms and filamentous bacteria is highly recommended in these lesions. Special staining (e.g. silver stains and periodic acid–Schiff stain) can aid in the identification of infectious organisms.
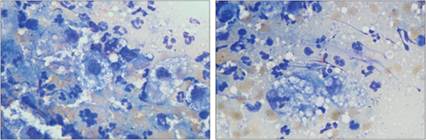
Figures 2.42, 2.43 Pyogranulomatous inflammation. FNA from a subcutaneous mandibular mass on a 14-year-old, neutered male mixed-breed dog. Degenerate neutrophils are present in large numbers. More than 20% of the cells are large macrophages. Many of the macrophages are vacuolated (Wright–Giemsa, 1,000? magnification).
Lymphocytic/plasmacytic inflammation
Lymphocytic inflammation is diagnosed when large numbers of small, well-differentiated lymphocytes predominate (Figure 2.44). If moderate numbers of plasma cells are also seen, the inflammation can be diagnosed as lymphoplasmacytic (Figure 2.45). Antigenic stimulation and type IV (delayed) hypersensitivity reactions are differentials for this type of inflammation. Sources of antigen are varied and include vaccines, insect bites, and viral infection.
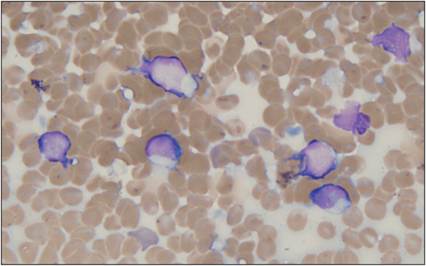
Figure 2.44 Lymphocytic inflammation. FNA of a dermal mass on the bridge of the nose of a 2-year-old, spayed female Border Collie. The sample contains moderate numbers of small to intermediate-sized lymphocytes with scant cytoplasm and a rounded nucleus with smooth chromatin. Large numbers of erythrocytes are present in the background (Wright–Giemsa, 1,000? magnification).
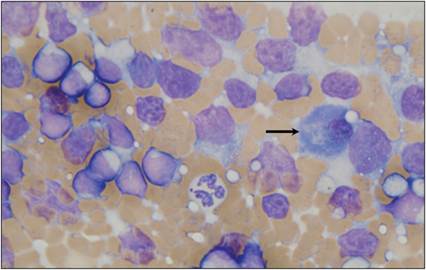
Figure 2.45 Lymphoplasmacytic inflammation. FNA from a firm, dermal lesion on the head of a cat. There are several erythrocytes and moderate numbers of lysed cells present. Intact small lymphocytes and fewer intermediate-sized lymphocytes and plasma cells (arrow) are observed. One neutrophil is present at the center of the image (Wright–Giemsa, 1,000? magnification).
Mixed inflammation
Chronic inflammatory lesions can involve all inflammatory cell types (Figures 2.46, 2.47). The predominant cell type should be identified, if possible, so that a more targeted list of differential diagnoses can be made.
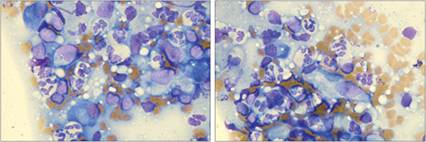
Figures 2.46, 2.47 Mixed inflammation. FNA of a raised dermal mass on the pinna of an 8-year-old, neutered male Boxer. A mixed population of neutrophils, macrophages, lymphocytes, and plasma cells is seen (Wright–Giemsa, 1,000? magnification).