Round cell origin tumors
Lymphoma/leukemia
Lymphoma is the most commonly observed neoplasm in the liver and can be found as a primary hepatic lymphoma or as part of a multicentric process (e.g. stage III–V lymphoma or leukemia [Figures 9.39–9.43a, b]; Trigo et al., 1982; Roth, 2001).
Although most hepatic lymphoma cases will contain approximately 50% large lymphocytes, the presence of >5% large lymphocytes found in multiple sites has been used as a criterion for diagnosing hepatic lymphoma (Stockhaus et al., 2004). These cells cytologically look similar to lymphoma in other tissues (see Chapter 8). History will commonly describe hepatomegaly with a diffuse lesion or multiple target lesions noted on echography. Addition of hepatic cytology to the lymphoma staging protocols affects the perceived stage; oddly, one study found that it migrated from stage III to stage IV, but this change did not predict a change in survival (Nerschbach et al., 2016).Lymphoma is not a single disease entity but a heterogeneous group of neoplasms, all of lymphocyte origin. Distinction of B- or T-cell origin can be determined with immunocytochemical, polymerase chain reaction (PCR), or flow-cytometric techniques (Figures 9.42a, b, 9.43a, b). Subclassification into one of the several lymphoid classification systems often requires either multiple aspirations to obtain sufficient numbers of cells for immunologic testing or biopsy to evaluate the architecture of the node. The diagnosis of large granular lymphocyte lymphoma can occasionally be made by cytology on liver samples (Figure 9.39). Diagnosis of small-cell lymphoma can be difficult, especially since a small lymphocyte inflammatory population can be present in lymphocytic cholangitis and hepatitis (Otte et al., 2017). The observation of a pure population of lymphocytes from several locations, potentially in conjunction with immunophenotyping or clonality testing, can help bolster a diagnosis of lymphoma or chronic lymphocytic leukemia (Figure 9.39; van den Ingh et al., 2006a, b).
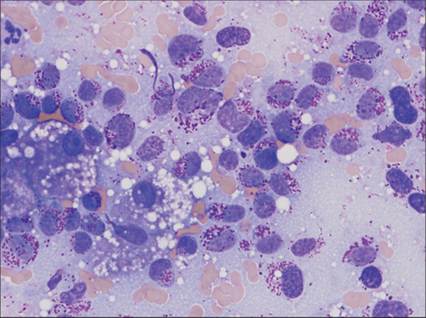
Figure 9.39 An infiltrative population of large round cells, which contain coarse fuchsia granules, are noted in this feline hepatic sample. The presumptive diagnosis is large granular lymphoma (Wright–Giemsa, 1,000? magnification). (Courtesy Dr. Amy Schnelle.)
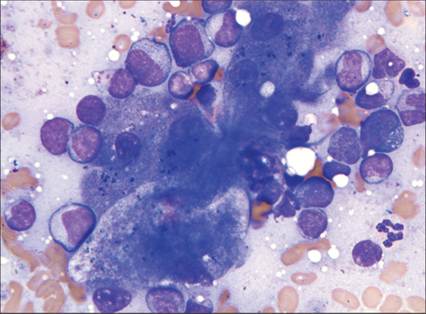
Figure 9.40 Neoplastic round cells are noted within the hepatic aspirate and were also found in samples from the spleen and peripheral blood of this Golden Retriever. Most of the round cells have scant amounts of basophilic cytoplasm and round nuclei, which are the same size or larger than the neutrophil present in the lower right corner of the image. Few neoplastic cells contain small pink cytoplasmic granules. The sample is most consistent with acute leukemia/lymphoma (Wright–Giemsa, 1,000? magnification).
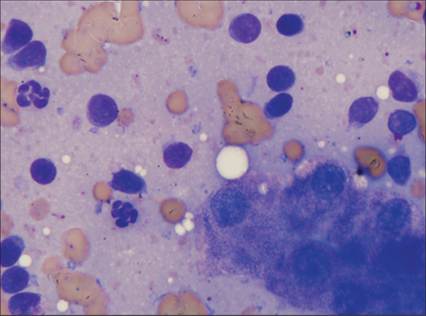
Figure 9.41 The liver aspirate from this domestic shorthair cat has very few clusters of hepatocytes and abundant lymphocytes, most of which are small cells (i.e. scant rim of cytoplasm around a nucleus smaller than a neutrophil and condensed chromatin). Very few blast cells are noted. Histologically, this was confirmed as a small-cell lymphoma (Wright–Giemsa, 1,000? magnification).
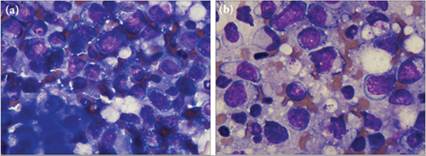
Figures 9.42a,b (a) A small cluster of hepatocytes is present in the lower left corner of the field; however, the predominant cell type in the image (and on the slide) is large lymphocytes, consistent with lymphoma. (b)A thinner area of the slide helps display the morphology of the large lymphoid cells. They are 2–3 times larger than a red blood cell, with increased amounts of basophilic cytoplasm, open chromatin, and one to several poorly distinct nucleoli.
These cells were CD3 positive by immunocytochemistry, suggesting a T-cell lymphoma (Wright–Giemsa, 1,000? magnification).
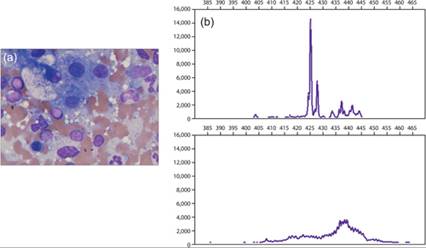
Figures 9.43a,b (a) An increased number of intermediate-sized lymphocytes with lower numbers of small and large lymphocytes is consistently found in multiple fields of this liver sample. This could suggest either lymphoid hyperplasia or lymphoma. Hepatocytes with foamy cytoplasmic rarefaction (suggesting glycogen or hydropic degeneration) and red and white blood cell precursors (suggesting extramedullary hematopoiesis) are also found (Wright–Giemsa, 1,000? magnification). (b) PARR analysis (PCR for antigen receptor rearrangement) on this sample confirmed a clonal expansion of lymphocytes and provided the diagnosis of T-cell lymphoma. The top graph depicts the patient’s T-cell receptor PARR results; note the narrow, tall peak, which indicates a clonal expansion of the T-cell receptor. Compare the patient’s results with the lower image from a reactive lymph node, which depicts a polyclonal T-cell receptor rearrangement. The x-axis indicates the size of the PCR product; y-axis indicates the level of fluorescence (an indication of the quantity of the PCR product). (PARR image courtesy Dr. Anne Avery.)