Sampling
Indications and contraindications
Cytologic evaluation of the liver and gallbladder contents is generally pursued to confirm and define suspected hepatobiliary disease or screen for hepatic metastasis during staging of cancer.
Hepatic cytology should be considered a valued part of the diagnostic toolkit.The liver produces most of the plasma coagulation factors; this has led some to avoid aspiration when liver failure is suspected. Several studies suggest that altered coagulation times (prothrombin time [PT], activated partial thromboplastin time [aPTT], and buccal mucosal bleeding time) are not associated with significant post-collection complications (Moritz et al., 2018; Vasanjee et al., 2006). However, thrombocytopenia has been strongly correlated with post-procedural bleeding (Bigge et al., 2001). When hemorrhage was noted after hepatic aspiration, the clinical effects were minimal (Reece et al., 2020). As a general rule, therefore, evaluation of at least PT, aPTT, and platelet count is commonly advised for most patients prior to biopsy techniques. Mildly to moderately elongated coagulation results with normal platelet counts should not be viewed as a contraindication for hepatic sampling, but instead should indicate that there is an increased likelihood of post-sampling complications and additional monitoring may be advantageous. If clinically apparent bleeding diathesis, thrombocytopenia, or severely aberrant results are found, the potential risks of post-aspiration bleeding should be weighed against the potential information gained from the procedure.
Another potential contraindication is the possibility of iatrogenic metastasis. Very few studies have evaluated the potential to disseminate cancer during biopsy in veterinary medicine; those that have been published deal with urinary tract and pulmonary cancers (Nyland et al., 2002; Vignoli et al., 2007).
Extrapolating from human cases and animal models of human cancer, hepatocellular and biliary carcinomas are not likely to seed along the needle tract but subcutaneous implantation of hepatocellular carcinoma has been reported in dogs and humans (Peterson et al., 2022). The result of one meta-analysis on the tumor metastatic effect of biopsy retrieval concluded that more was gained from sampling and identifying a lesion than was risked in the collection of the sample (Klopfleisch et al., 2011). This does not mean that the risk should be ignored. Sample collection should be planned to avoid as many vital structures as possible and make resection as minimally destructive as possible.Technique
Fine needle aspiration (FNA) of the liver can usually be performed without sedation or local or general anesthesia. For larger, palpable masses or suspected diffuse disease (lymphoma), a blind technique can be used. Ultrasound guidance is usually advantageous for most cases, especially those with nonpalpable focal lesions. Ultrasound findings should guide the choice of approach. As a general rule, approaching along the costal arch or on the right thorax at the level of the 10th intercostal space will usually allow access to the liver. Fasting the patient is not required but may ensure that the stomach is not along the path of sampling. If a focal lesion is present, aspirates of the center of the mass as well as the margin of the lesion should be taken as both sites will provide different, yet complementary findings. Aspiration of the center of a large mass often shows necrosis and an inflammatory response, while aspiration of the margin contains an obviously neoplastic population. Studies have shown that sampling of multiple sites increases the probability of obtaining a representative sample (Kemp et al., 2015; Chaivoravitsakul et al., 2021).
Ultrasound gel must be meticulously removed prior to aspiration. Ultrasound gel preferentially attracts most stains and can prevent full cytologic evaluation of any obtained cells (Figure 9.1).
Intraoperative evaluation of lesions and rapid evaluation can aid the surgeon in making decisions on resection and closure techniques. 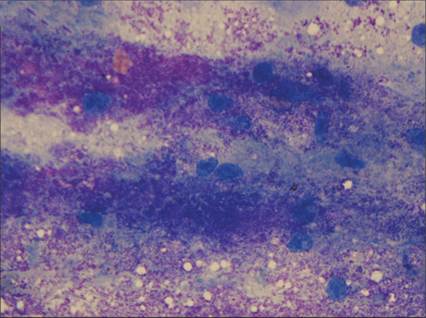
Figure 9.1 The copious amount of purple granular material that obscures cytologic features of the underlying hepatocytes is consistent with ultrasound gel. For cytologic evaluation, it is imperative that gel be removed from the site of needle insertion prior to collection of aspirates (Wright–Giemsa, 400? magnification).
A 20–22-gauge needle up to 3 inches (7.5 cm) long will allow penetration to the level of the liver in most patients. A 3 ml disposable syringe is ideal as it minimizes the amount of suction that can be applied while collecting the sample and can be either directly connected to the needle or to a segment of extension tubing. The needle should be placed at the site of the lesion and then advanced and retracted 5–10 mm multiple times along a single track (a sewing machine type action) to pack hepatocytes into the needle (Rothuizen & Twedt, 2009). Aspiration with application of negative pressure has also been described but is not recommended owing to the highly vascular nature of the liver (Rothuizen et al., 2006; Rothuizen & Twedt, 2009). The application of negative pressure will frequently cause excessive blood collection. If suction is applied, it should be completely released prior to withdrawal of the needle from the sample site; this is especially important in patients with ascites to prevent contamination of the sample with ascitic fluid. After withdrawal, disconnect the syringe, fill it with air, reattach it to the needle, and gently expel the contents of the needle onto a clean, labeled glass slide. An additional slide is then used to gently make squash preparations of the sample. Biopsy samples taken for histopathology can be rolled (tru-cut type biopsies) or imprinted (wedge biopsies) on a clean glass slide to provide a quick cytologic evaluation (Chapter 1).
After the sample is air-dried, a Romanowsky stain (e.g. Wright–Giemsa, Diff-Quik®) will provide excellent staining for routine cytologic evaluation. Alternatively, special stains can be applied to unstained samples to highlight or identify pigments and structures on the slide (Table 9.1).
Table 9.1 Selected special stains that can be applied to liver aspirates and their most common use
| Special stain | Use | Used on Romanowsky- stained slides |
| Rubeanic acid | Copper | Unknown |
| Rhodanine | Copper | Yes |
| Oil red O | Lipid | No |
| Sudan black | Lipid | No |
| Periodic acid–Schiff | Glycogen, fungal hyphae | Yes |
| Prussian blue | Iron, hemosiderin | Yes |
| Modified Ziehl–Neelsen | Lipofuscin, ceroid | Yes |
| Luxol fast blue | Lipofuscin, ceroid | Unknown |
| Hall’s | Bilirubin | Yes – frozen or nonstained tissue preferred |
| Schmorl reaction | Lipofuscin | Unknown |
Efficacy
Hepatic FNA, with or without ultrasound guidance, is most accurate at detecting hepatocellular and biliary neoplasia, less accurate at detecting vacuolar change, and has only poor sensitivity and accuracy for necrosis, hyperplasia, and cystic lesions (Roth, 2001; Bahr et al., 2013, Masserdotti, 2020). There are contradicting reports on the accuracy of hepatic FNA for inflammatory processes (Weiss et al., 2001; Bahr et al., 2013, Gardner et al., 2022). As with most cytologic samples, detection of an abnormal finding is more meaningful than a lack of abnormal findings. A recent retrospective study concluded that agreement with histopathology had low sensitivity and specificity (60% and 68.6% respectively) in the diagnosis of a single mass (Cray et al., 2023). If clinical suspicion is high for a disease process that is not detected on an initial sampling, repeat aspiration is recommended (Cohen et al., 2003).
Ultrasound is sometimes used to identify the affected area. However, it has been shown that ultrasonographic appearance was insufficient to detect various types of canine and feline diffuse infiltrative liver disease (Feeney et al., 2008). This study found that ultrasound diagnosis of liver imaged as normal had an accuracy of as low as 60%. In a similar study of canine patients known to have mast cell tumors elsewhere in the body, ultrasound failed to identify any cases of mast cell metastasis to the liver and had a reported sensitivity of 0% (Book et al., 2011). Irrespective of ultrasound findings, it is of diagnostic value to sample the ‘normal’ appearing tissue when hepatopathy is suspected.