Synovial fluid
Sampling
Aspiration of synovial fluid from the joints of dogs and cats is often performed on effusive joints, although fluid may occasionally be collected from joints without obvious effusion.
These joints may have accompanying masses, be associated with clinical lameness, or have previously displayed clinical or cytological abnormalities.Collection of joint fluid requires limited supplies. Materials for aseptic preparation of the site, an appropriately sized hypodermic needle, 3 ml or 6 ml syringe, an EDTA tube, and a sterile glass tube should be gathered in preparation. The patient should be appropriately restrained, with sedation or anesthesia, as indicated. Pain control should be instituted as needed. The site should be selected by reviewing anatomic landmarks and flexing and extending the joint of interest; this allows identification of a site in which the joint space may be accessed without a high likelihood of encountering significant vessels, nerves, cartilage, or bone. Review of individual joint anatomy may be helpful, and illustrated guides are available in clinical technique textbooks and elsewhere (Johnson & Mackin, 2012a). Once selected, the site should be clipped and prepared with a sterile scrub, and the synovial fluid should be carefully collected using sterile technique (Figures 12.1a–c). This ensures that an appropriate sample for culture is available, if needed, as well as avoiding introduction of microorganisms into the synovial space. Synovial fluid can be collected using a 22- or 25-gauge hypodermic needle of length sufficient to penetrate the joint of interest. Aspiration is applied to collect the fluid; however, aspiration should be discontinued before withdrawing the needle to help reduce blood contamination. A notation should be made if obvious blood contamination occurs during collection.
Synovial fluid should be collected into an EDTA tube for cytologic analysis, a sterile glass tube for any serologic testing or culture, and/or a culturette for bacterial culture, if needed.
Collection of fluid into an EDTA tube is helpful for prevention of cell clotting in samples with peripheral blood contamination. Clotting and cell aggregation can interfere with determination of accurate cell estimates. Preparation of one or more direct smears at the time of fluid collection is also beneficial. This provides a baseline for assessment of cell morphology and can help distinguish real findings from in-vitro artifacts. This is particularly helpful when trying to discern true hemorrhage from in-vitro peripheral blood contamination. 
Figures 12.1a–c The site should be prepared with a surgical clip (a) and then aseptically prepared (b). Sterile technique should be employed in sample collection (c). These steps ensure that microorganisms are not introduced into the synovial space during sampling and that the sample remains free of microorganism contamination. (Courtesy Brian Husbands.)
Analysis
Analysis of synovial fluid typically consists of measurement of the total protein concentration (generally estimated by a refractometer), a nucleated cell count, and cytologic assessment. It may also include assessment of mucin clot quality and viscosity if sufficient sample is available. Normal synovial fluid is typically thick in character, clear, and pale yellow or colorless.
A normal total nucleated cell count of viscosity was decreased in only 17 of 36 joints in which it was assessed (Jacques et al., 2002). In the author’s experience, fluid viscosity is often normal in joints with overt clinical and microscopic abnormalities, and assessment of this characteristic of synovial fluid should be omitted if only a limited sample volume is available for diagnostic testing.
Protein concentrations of 1.5–3 g/dl (15–30 g/l) are commonly observed in healthy synovial fluid (MacWilliams & Friedrichs, 2003). Protein concentrations may be elevated with the addition of inflammatory proteins or may decrease with fluid influx associated with effusion.
Protein concentrations may also be normal in samples with other evidence of joint disease.Assessment of direct smears of synovial fluid on low power (100? magnification) typically reveals an eosinophilic, stippled background, with windrowing (linear arrangement) of cells within this material, which reflects the high viscosity of the fluid (Figures 12.2a–d). This material is often thick and prevents adequate cell spreading. Since this material obscures much of the fine cytologic detail, the nucleated cells within the sample should be evaluated in the thinnest portions of the smear for more accurate determination of cell size, cytologic and nuclear features, and presence of inclusions or infectious organisms. The amount of blood that is present should be noted, as this may influence the cells observed. Cells within normal synovial fluid samples consist primarily of large mononuclear cells, which may include macrophages, monocytes, and synovial lining cells, as well as small mononuclear cells (consistent with small lymphocytes). Macrophages and monocytes within synovial fluid are similar in appearance to those observed elsewhere within the body; macrophages may or may not have vacuolated cytoplasm. Synovial lining cells may be rounded to spindloid in shape, with moderate to abundant basophilic cytoplasm, rounded or ovoid nuclei, and stippled chromatin. Neutrophils are infrequently identified and should be nondegenerate if observed in otherwise normal synovial fluid. Although variable percentages of neutrophils have been reported in synovial fluid, most samples contain less than 10% neutrophils (Pacchiana et al., 2004).
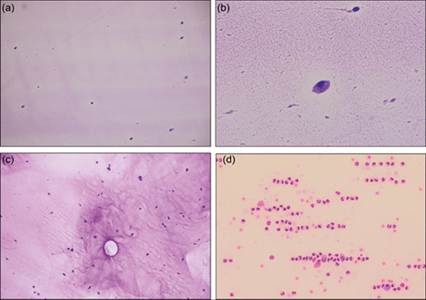
Figures 12.2a–d (a, b) Normal synovial fluid is of low nucleated cellularity with eosinophilic stippled background material (Wright–Giemsa: a, 100? magnification; b, 500? magnification). (c) The viscous nature of synovial fluid can result in uneven distribution of nucleated cells within a smear, posing a challenge in estimating cellularity (Wright–Giemsa, 100? magnification).
(d) The linear arrangement (windrowing) of cells is demonstrated in this synovial fluid sample with marked suppurative inflammation. Note the stippled, eosinophilic background; this highly viscous material results in the cellular arrangement observed in the image (Wright–Giemsa, 250? magnification).
Inflammatory arthritides
Inflammatory joint disease of infectious and noninfectious causes often is characterized by increased numbers of nucleated cells; generally, significantly increased fractions of neutrophils are part of the process. Since infectious and noninfectious diseases may have a similar cytologic appearance, clinical impression and suspicion are often very important in the selection of subsequent diagnostic testing for further differentiation.
Suppurative inflammation
Infectious disease
A variety of organisms can result in inflammatory joint disease, including bacterial, rickettsial, spirochetal, fungal, mycoplasmal, and viral pathogens. Observation of intracellular bacteria within synovial neutrophils indicates a need for culture of synovial fluid. Unfortunately, bacteria may not be visually identified in all cases of septic arthritis; therefore, bacterial culture may have value in cases with increased clinical suspicion, such as a juvenile animal with multiple effusive joints or a patient with a previous trauma to an affected joint. Culture may be generally valuable in cases with increased fractions of neutrophils without identified organisms, particularly those samples with moderately to markedly elevated nucleated cell counts (Figure 12.3). A retrospective study of 31 cases of septic arthritis reported a range in neutrophil fractions from 25% to 99%, with a median of 90% (Clements et al., 2005).
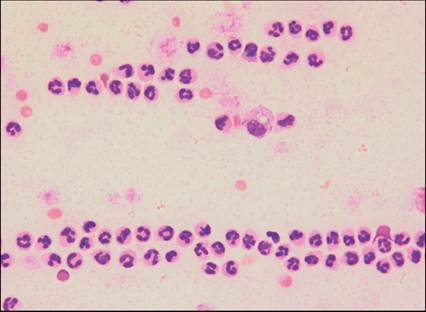
Figure 12.3 Suppurative arthritis in a dog. The sample is cellular and consists of nondegenerate neutrophils exhibiting marked windrowing (Wright–Giemsa, 500? magnification).
A variety of organisms can be identified. One study cultured Staphylococcus intermedius most frequently from ten cases of septic arthritis; S. haemolyticus, Streptococcus canis, and Enterococcus faecalis were among other cultured organisms (Riggio et al., 2014). Another study similarly cultured Staphylococcus spp. most commonly, followed by Streptococcus spp. and others (Clements et al., 2005). Using polymerase chain reaction (PCR), bacterial DNA was detected in joints with cranial cruciate rupture and medial patellar luxation, as well as normal synovial fluid, though the clinical significance is unclear (Bhandal et al., 2013). Mycoplasma gateae induced erosive joint disease in multiple joints in a young cat; the organism was isolated via anaerobic culture (Zeugswetter et al., 2007). Dogs experimentally infected with the spirochete Borrelia burgdorferi developed joint inflammation that was primarily suppurative during acute disease, transitioned to a mixed inflammatory population of neutrophils and mononuclear cells in intermediate stages, and was typically lymphoplasmacytic in chronic disease (Summers et al., 2005). Rickettsial morulae may be observed in cells within synovial fluid and are cytologically consistent with those observed in peripheral blood leukocytes (Figures 12.4a–d). The protozoan Leishmania donovani can result in joint inflammation, and amastigotes have been identified within macrophages alone or within both macrophages and neutrophils in synovial fluid (McConkey et al., 2002; Santos et al., 2006). A retrospective study of 13 cases of dogs with L. donovani found that synovial fluid nucleated cell counts ranged from 34,000 to 66,000 cells/μl; neutrophils ranged from 34% to 89%, and lymphocytes ranged from 18% to 62% (Sbrana et al., 2014). Blastomyces dermatitidis can be identified within the synovial fluid of infected dogs (Woods et al., 2013). Diagnostic testing for underlying infectious disease may be useful prior to starting immunosuppressive therapy for suspected immune-mediated joint disease.
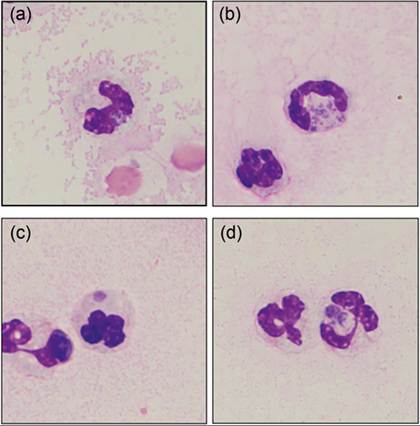
Figures 12.4a–d Rickettsial arthritis in a dog; molecular testing was not performed to determine species. Neutrophils contain basophilic, stippled morulae (Wright–Giemsa, 1000? magnification).
Noninfectious disease
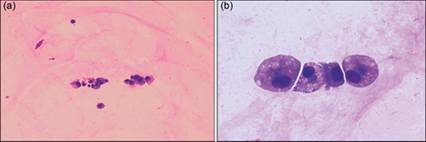
Immune-mediated arthritides include idiopathic polyarthritis, polyarthritis secondary to drug or vaccine administration, breed-specific conditions (e.g., Akitas and Shar Peis), steroid-responsive meningitis–arteritis, systemic lupus erythematosus, and polyarthritis/polymyositis syndrome; these conditions are not typically associated with erosive lesions of articular cartilage or underlying bone (Johnson & Mackin, 2012b). They typically affect young adult dogs, although the polyarthritis that affects Akitas occurs in dogs less than 1 year of age (Johnson & Mackin, 2012b). In cats, idiopathic polyarthritis, systemic lupus erythematosus, and chronic progressive polyarthritis have been reported (Oohashi et al., 2009). In animals in which other causes of cartilage and bone destruction have been ruled out, erosive polyarthritis should raise concern for rheumatoid arthritis in dogs and chronic progressive polyarthritis in cats, as these conditions are associated with radiographic changes in these species (Johnson & Mackin, 2012b). When synovial fluid is altered by suppurative inflammation and immune-mediated joint disease is a clinical concern, negative test results for likely infectious diseases (through culture, PCR, serology, etc.) and assessment of radiographic findings can help support clinical suspicion. Identification of multiple inflamed joints is an expected finding, although rare cases with single joint involvement are reported (Johnson & Mackin, 2012b). Neutrophils containing large, rounded, deeply eosinophilic inclusions (lupus erythematosus cells) and small, variably sized, rounded inclusions (ragocytes) have sometimes been associated with cases of suppurative arthritis due to an immune-mediated etiology. This material is thought to represent phagocytized nuclear material or complexes of immunoglobulin with cell or nuclear material (Figures 12.5a–c). However, these inclusions are infrequently identified, and care must be taken not to misinterpret intracellular bacteria or phagocytized cell debris. If used judiciously in patients with other strong clinical evidence, testing for rheumatoid factor and antinuclear antibodies, respectively, can help lend support for diagnosis of rheumatoid arthritis or systemic lupus erythematosus, respectively (Johnson & Mackin, 2012a, 2012b). Alone, positive results for either test are not pathognomonic for those conditions, and interpretation should be done with caution.
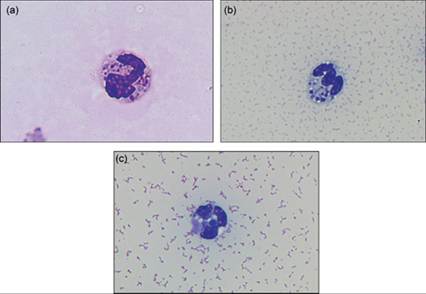
Figures 12.5a–c Synovial fluid from a dog with immune-mediated polyarthritis. (a) A neutrophil contains many basophilic structures; this cell is consistent with a ragocyte (Wright–Giemsa, 4,000? magnification). (Courtesy Anne Barger.) (b) Synovial fluid from a different dog; a ragocyte is also pictured (Wright–Giemsa, 3,000? magnification). (c) Same dog as 14.4b. A single lupus erythematosus cell is noted with a large basophilic inclusion (Wright–Giemsa, 3,000? magnification). (Courtesy Amy MacNeill.)
Mononuclear inflammation
Mononuclear inflammation of synovial fluid consists of increased numbers of large mononuclear cells, typically with a smaller fraction of small lymphocytes within the fluid (Figures 12.6a, b). This type of inflammation is typically mild to moderate in degree and is associated with degenerative joint disease or trauma. Radiographic evaluation can help identify evidence of osteoarthritis and may identify overt traumatic injuries.
Figures 12.6a,b Mononuclear inflammation due to osteoarthritis in a dog. This synovial fluid had a mildly increased nucleated cell count, due to increased numbers of large mononuclear cells (Wright–Giemsa: a, 250? magnification; b, 1,000? magnification).
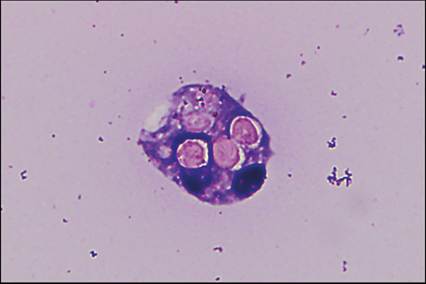
Figure 12.7 Phagocytized erythrocytes within a degenerating synovial macrophage (Wright–Giemsa, 3,000? magnification).