Hemarthrosis
Hemarthrosis is hemorrhage within a synovial space, which may be seen secondary to trauma, anticoagulant rodenticide intoxication, hereditary coagulation abnormalities, and other bleeding diatheses.
Observation of uniformly red synovial fluid during collection is supportive of hemarthrosis (as opposed to a wisp of red that may appear with peripheral blood contamination). Identification of macrophages containing phagocytized erythrocytes, as well as hemosiderin pigment (blue–black, granular material) and hematoidin crystals (orange, rhomboid, refractile, crystalline material), is indicative of joint hemorrhage in smears prepared immediately after synovial fluid collection (Figure 12.7). Care must be taken in interpreting erythrophagia in fluid samples that have been shipped or had other delays in sample processing, as in-vitro erythrophagia may have occurred.Tumors of the joint
A varied population of cells makes up the synovial lining, including vascular and adipose tissue and cells of fibroblast (synoviocytes) and macrophage origin. A review of 35 synovial tumors in dogs found 18 histiocytic sarcomas diagnosed in part by positive staining for CD18, and 5 synovial cell sarcomas were identified via positive staining for cytokeratin. The other tumors were synovial myxomas and several other sarcomas, including fibrosarcoma and chondrosarcoma (Craig et al., 2002).
Sarcomas of multiple types can have similar cytologic features (Figures 12.8a–c). These include spindloid or stellate borders, wispy cytoplasmic projections, variable amounts of moderately basophilic cytoplasm, nuclear pleomorphism, and prominent nucleoli. The cells can display mild to marked variations in cell, nuclear, and nucleolar size, as well as increases in the nuclear to cytoplasmic (N:C) ratio. Histiocytic sarcoma may share these features, but cells with rounded borders, cytoplasmic vacuolation, multinucleation, and lobulated nuclei may be observed as more prominent features (Figures 12.9a, b).
Similarly, synovial cell sarcoma has an appearance that can be difficult to differentiate from other sarcomas cytologically (Figure 12.10). Individualized and aggregated spindloid to rounded cells are observed, with moderate to marked criteria of malignancy. Special staining of histopathologic sections may be necessary for definitive diagnosis. A case report of a biphasic (spindloid and epithelioid components) synovial cell sarcoma was negative for the cytokeratin used in the immunohistochemical staining of the study, but foci of cells were positive for epithelial membrane antigen (Loukopoulos et al., 2004). Tumors of other cell types that involve the joint, such as lymphoma or metastatic carcinoma, are rare (Lahmers et al., 2002). 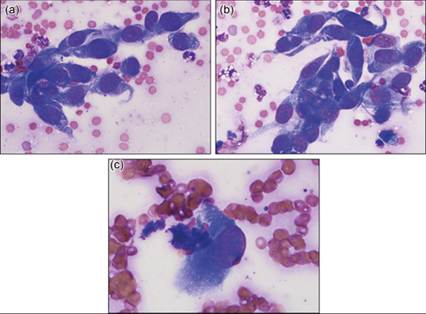
Figures 12.8a–c (a) Sarcoma cells demonstrating spindloid borders, moderately basophilic cytoplasm, rounded to ovoid nuclei, coarsely stippled chromatin, and prominent nucleoli (Wright–Giemsa, 500? magnification). (b) Criteria of malignancy observed in sarcoma: anisocytosis, anisokaryosis, anisonucleoliosis, binucleation, and anisokaryosis within a binucleated cell (Wright–Giemsa, 500? magnification). (c) Cell demonstrating nucleolar irregularity (Wright–Giemsa, 800? magnification).
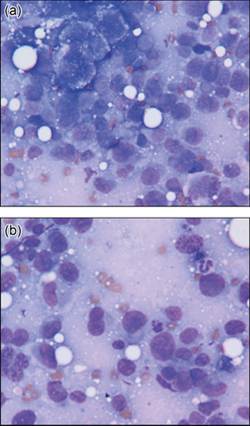
Figures 12.9a,b Histiocytic sarcoma in a dog. Rounded, irregular, and spindloid mesenchymal cells displaying marked pleomorphism (Wright–Giemsa, 700? magnification). (Courtesy Anne Barger.)
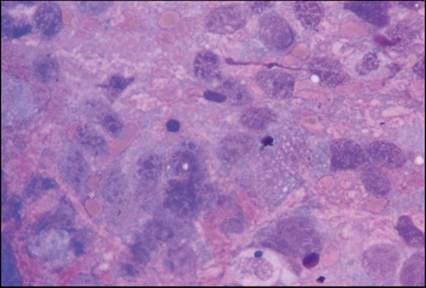
Figure 12.10 Synovial sarcoma in a dog. Spindloid to rounded cells demonstrate several criteria of malignancy within a background of eosinophilic, granular material (Wright–Giemsa, 800? magnification). (Courtesy Anne Barger.)
It should be noted that in human medicine, the term ‘synovial sarcoma’ has replaced ‘synovial cell sarcoma’, as research has determined that the cell of origin is a mesenchymal stem cell, rather than synoviocytes, with diagnosis made via genetic marker (Craig et al., 2015).
This nomenclature has been adopted by some in veterinary medicine, with one report suggesting the term ‘cytokeratin-positive joint associated sarcoma’ for use in tumors with appropriate IHC markers (Monti et al., 2018).Skeletal muscle
Sampling
Standard aspiration or fenestration techniques are employed in sampling skeletal muscle or tumors of skeletal muscle.
Normal cytology
In general, normal striated skeletal muscle is poorly exfoliative; however, fragments of skeletal muscle can be observed in a wide variety of samples, due to incidental aspiration (Figures 12.11a, b). The cytoplasm of the myocytes found in these fragments is deeply basophilic staining and, with adjustment of the fine focus of the microscope, the internal striation of the cells is often appreciable. Low numbers of nuclei are typically visible as small and oval-shaped with dark chromatin, although frequently a high level of detail is not appreciable. The nuclei are expected to be uniform in size and shape.
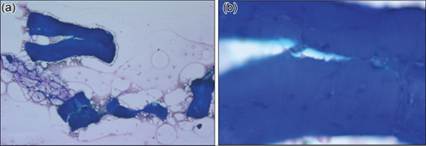
Figures 12.11a,b Striated skeletal muscle and mature adipose tissue. (a) Fragments of striated skeletal muscle may be seen on occasion. The linear arrangement of myocytes is typically preserved. (b) By adjusting the fine focus of the microscope, the cytologist can often appreciate the fine striations within the myocytes (Wright–Giemsa: a, 100? magnification; b, 500? magnification).
Inflammation (myositis)
Myositis is uncommonly observed on cytology. A presumptive or suspected cytologic diagnosis may be possible in samples containing significant numbers of inflammatory cells observed in close association with fragments of skeletal muscle; however, histopathology is recommended for definitive diagnosis.