Thyroid gland
Normal thyroid gland
The thyroid gland is composed of primarily thyroid follicular cells, which line the thyroid follicles. Cytologically, these cells are seen in sheets that often have poorly distinct cell borders and appear as nuclei on a background of light blue to light purple cytoplasm.
If intact cell borders are present, the cells should have a high to rarely moderate nuclear to cytoplasmic (N:C) ratio and a round, central nucleus. The nuclei have finely stippled to reticular chromatin and inconspicuous nucleoli. A variable amount of colloid may be present. Colloid appears as amorphous, eosinophilic, extracellular material on cytology.Thyroid medullary cells (also called parafollicular cells or C cells) are the second main cellular component of the thyroid gland. A cytologic description of these cells has not been previously documented. These cells may have a similar cytologic appearance to thyroid follicular cells, as the histologic findings in these cell populations are similar and they often require additional special stains for differentiation (Feldman et al., 2005). Thyroid medullary cells make up approximately 9% of the cells within the canine thyroid gland (Sokolowska et al., 2022).
Thyroid gland inflammation
Although inflammation does occur in the thyroid gland and is thought to be one of the main causes of hypothyroidism in dogs, cytologic evidence of inflammation is not common because the inflammation does not often lead to gland enlargement to a significant degree. Inflammation that leads to hypothyroidism is composed of predominantly lymphocytes, with plasma cells and macrophages occasionally noted on histology (Miller, 2017).
Thyroid gland neoplasia
The thyroid gland is often sampled for cytology when a mass is palpated in the ventral neck during a physical examination. The specific causes for neoplastic thyroid lesions in the dog and cat are different, but cytologic findings are often similar.
Thyroid adenomatous hyperplasia and thyroid adenomas are much more common in the cat. In two studies, shows evidence of moderate anisokaryosis (Wright–Giemsa, 500? magnification).
Thyroid C cells (or thyroid medullary cells) are also found within the thyroid gland and can lead to neoplasia. The incidence of this tumor in dogs has previously been described as low, but thyroid medullary carcinoma was found to represent approximately one-third of canine thyroid neoplasms in a previous study (Campos et al., 2014). Adenomas and carcinomas of thyroid medullary origin can produce amyloid (Patnaik Lieberman, 1991), which would appear cytologically as amorphous, fluffy, dark pink material in close association with the medullary neoplastic cells. The amyloid is thought to be produced locally, unlike with systemic diseases that cause amyloidosis of multiple organs. Confirmation of amyloid can be achieved by staining with Congo red and then using a polarizing filter to detect birefringence. Adenomas may occur as single or multiple lesions (Miller, 2017). Carcinomas are more likely to be multinodular in origin and more likely to lead to irregular enlargement of one or both lobes of the thyroid gland (La Perle, 2011). Carcinomas also have the potential to metastasize, with the most common locations of metastasis being the cranial cervical lymph nodes and the lungs. A unique case of multiple bone metastasis of medullary thyroid carcinoma has been reported in the dog (Renzi et al., 2022) Cytochemical and immunocytochemical stains/labeling antibodies that may be most beneficial for establishing a diagnosis of thyroid medullary carcinoma include Grimelius stain, neuron-specific enolase, synaptophysin, and calcitonin (Patnaik Lieberman, 1991) with cytokeratin-19 and thyroglobulin being beneficial to determine follicular origin (Ciaputa et al., 2014). Special staining may be the only way to distinguish a medullary neoplasm, as microscopic findings are similar to those of follicular neoplasms (Feldman et al., 2005).
Prognostic factors have recently been described for thyroid carcinoma of either follicular or medullary origin regarding increased likelihood of local invasiveness (tumor diameter, tumor volume, tumor fixation, ectopic location, follicular cell origin) and presence of distant metastasis (tumor diameter, tumor volume, bilateral location) (Campos et al., 2014).Ectopic thyroid tissue is common due to the complex embryogenesis of this organ. This tissue is usually found in the mediastinum but can be found anywhere from the base of the tongue to the diaphragm (Miller, 2017). Thyroid neoplasms due to accessory thyroid tissue have been reported in the dog (Almes et al., 2008; Boes et al., 2009a; Lyssens et al., 2020), but not the cat, and are an important differential to remember for lesions in the thoracic cavity with cytologic findings of endocrine origin. Sublingual ectopic thyroid neoplasia was found to make up 7.5% of thyroid neoplasia in a retrospective canine study (Broome et al., 2014).
Thyroid cysts
Thyroglossal duct cysts, thyroid cystic lesions, and parathyroid cystic lesions are also possible in the area of the thyroid (Swainson et al., 2000; Phillips et al., 2003). Thyroglossal duct cysts occur due to remnants of the thyroglossal duct (Miller, 2017). These types of lesions could lead to palpation and sampling of a mass. Cysts are epithelial-lined structures; however, the epithelial cells rarely exfoliate on cytology. This leads to aspiration of low cellularity fluid as the most common cytologic finding. For cysts/cystic lesions of the thyroid, cytologic findings are consistent with those of a seroma or hematoma including removal of brown to serosanguinous to orange, slightly cloudy fluid with an often low total nucleated cell count, variable but often elevated protein, and a mixed cellular makeup (Figure 16.6; Hofmeister et al., 2001; Phillips et al., 2003; Miller et al., 2017). Measurement of total T4 and parathyroid hormone (PTH) in the cyst fluid may be beneficial to help determine the origin of the lesion (Phillips et al., 2003).
Thyroid cystadenomas and cystic carcinomas have been described in the cat; therefore, additional testing may be needed when a cystic lesion is suspected to rule out thyroid neoplasia (Miller et al., 2017). 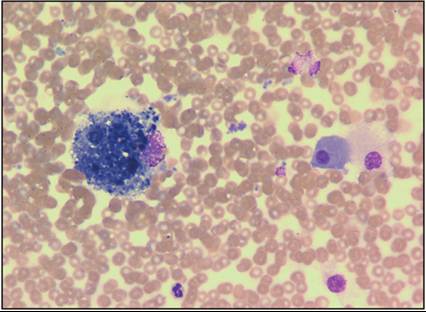
Figure 16.6 Thyroid cyst. Aspirate of fluid from a thyroid cyst showing moderate blood contamination and a macrophage that contains amorphous debris (Wright–Giemsa, 500? magnification).
Thyroid goiters
Goitrous hypothyroidism leading to a palpable ventral cervical mass has been reported in both dogs and cats and can occur secondary to congenital thyroid dyshormonogenesis in young animals (Peterson, 2015) or as spontaneous cases in adults (Galgano et al., 2014). These cases are often diagnosed by clinical signs (small stature, dull mentation, weakness/inactivity, weight gain, poor hair coat) and evaluation of thyroid hormones (Peterson, 2015; Galgano et al., 2014). Cytology is not often a component of the case workup.