Epidemics and Financial Practices from the Twentieth Century to Today
The twentieth century, when human beings stepped on the moon, transitioned into the information age with technological developments, and marked an era in science by developing robots, was also the scene of various and deadly outbreaks.
As a matter of fact, the two major world wars, the globalization trend and the mobility and migration movements, brought along outbreaks. The difference from previous epidemic adventures is that it shows a faster spread especially with the improvement in transportation opportunities. In addition, climate change (extreme heat and drought) caused by the increase in carbon emissions due to the increasing population and excessive consumption habits paved the way for the occurrence of various epidemics. It was perceived in another scenario as the most vital tool of war strategy. Although new measures were taken within the framework of developing economic and financial policies, collective deaths were inevitable.2.4.1 Spanish Flu (1918-1919) and Financial Practices
Considered to be the deadliest disease of the modern age, Spanish flu is estimated to have infected a 30-50% of the world’s population and killed 50 million people. The deadly virus H1N1, which emerged during World War I, was detected in the troops of both sides and the flow of information was restricted due to war reasons. Two possibilities were considered regarding the origin of the virus. In this context, the virus either started in China and came through the Chinese who migrated to North America or spread to the whole world in March 1918 from a military camp and prison in America where the first cases were seen. The epidemic was called the Spanish flu, as the world public learned about this through Spanish newspapers that did not participate in the war and were exempt from embargo (Lina 2008).
The second wave, which started in Europe and North America in August 1918 and when 90% of deaths were recorded, increased the number of cases that could not make it possible to fight in October 1918.
This created a strong belief that the outbreak was responsible for the end of the war. The third wave that took place in January 1919 showed a striking effect (Lina 2008). The number of people who lost their lives due to the epidemic is estimated to be 5 to 10 times more than those who died in World War I (Cotter 2020). In fact, according to some estimates, the deaths toll is thought to exceed 100 million. The Spanish flu, which spread from America to Asia, from Africa to the Pacific Islands, resulted in the grave picture in one year which the Black Death caused throughout a century. In addition, the epidemic was the first in terms of observability of long-term effects. Increased physical disability, low-income level, low socio-economic status, and higher transfer payments were identified in the postepidemic (especially births and born generation) studies (Almond 2006; Huremovic 2019).Information on the economic impact of Spanish flu is limited, both due to the fact that most governments have limited the flow of information because of the war, and that national income accounting was in its infancy at the time. The study of the Canadian Ministry of Finance suggested that the decreases in the industrial and commercial activity index resulted in only 0.4% loss in annual production (IMF 2006). The 1960s study investigating the effect of the outbreak in India suggested that agricultural production decreased by more than 3% (Schultz 1964 cited in IMF 2006). In addition, it was estimated that 8% of the agricultural workforce was infected and the heavy cost of the epidemic (through taxes and similar liabilities) was laid on the surviving section (IMF 2006).
2.4.2 HIV/AIDS Virus (1981-...) and Response Through Financial Policy Instruments
The HIV/AIDS epidemic, which started in the early 1980s in America and spread slowly throughout different continents and generations, has caused the death of more than 35 million people (Huremovic 2019). Evolving from wild African apes to humans, the virus produces new antigens while in the victim’s body and causes a person’s immune system to collapse (Diamond 2010).
As of the end of 2018, 37.9 million (36.2 million adult individuals, 1.7 million children under the age of 15) people live with HIV worldwide, while 1.7 million new people was infected with the epidemic. The epidemic has been infected by 74.9 million people since its inception in 1981 and killed more than 32 million people. The death toll, which peaked in 2004 with 1.7 million people, decreased to 770 thousand in 2018, especially with the policies pursued in underdeveloped countries where the virus was common. Since 2010, there has been a 33% reduction in the fatality rate arising from AIDS (UNAIDS 2019).
AIDS was declared by the World Bank as an economic development crisis in 2000. In some countries in sub-Saharan Africa, growth per capita was estimated to have decreased by 0.5% to 1.2% each year as a direct result of AIDS (Zakaria 2015). The vast majority of people with HIV worldwide live in East and South Africa (UNAIDS 2019). In the post-2010 period, Esvatini (Swaziland), Botswana, and Lesotho in South Africa were the countries with the highest adult HIV/AIDS prevalence in the world, with rates of respectively 25.9%, 24.8% 23.6%. While the epidemic, which is an important threat to development, decelerate the growth rate and increases medical care and health expenditures in the short term due to the sudden reaction in many countries’ economies, whereas in the long term, losses especially in human capital affect the transfer of information between generations and cause a risk (Anyanwu et al. 2013).
Untimely deaths due to AIDS reduce the qualified workforce and cause a long and costly replacement process. This was supported by findings in a study conducted in Tanzania that an estimated 40 billion dollars should be spent to train new teachers instead of teachers who died from AIDS by 2010 (Qilingiroglu 1998). Direct and indirect visible and invisible costs must be determined in order to determine the economic and financial dimension of the outbreak and to intervene in this direction (Qilingiroglu 1998).
These costs are:• “direct visible costs” such as diagnostic tests, health and personnel training, consultancy services, R&D activities,
• “direct invisible costs,” such as care services provided by patients’ relatives and charities, for free,
• “Indirect visible costs,” such as production losses due to illness and untimely death,
• “indirect invisible costs,” such as physical and psychological decline due to factors such pain, ache, anxiety, fear, blame, isolated life, depression as well as deterioration in quality of life.
Measures to combat AIDS are implemented according to the development level of the countries on a national scale, the priorities of health policies, and the effectiveness of donors and activists on an international scale. Within the scope of combating the AIDS epidemic, 90-90-90 global HIV targets set by UNAIDS are listed as follows (UNAIDS 2014):
• By 2020, 90% of individuals infected with HIV will know their HIV status.
• By 2020, 90% of all individuals diagnosed with HIV infection will receive continuous Antiretroviral Therapy (ART).
• By 2020, 90% of individuals in the ART process will have viral suppression (Fig. 2.2).
In the fight against AIDS, which is a global public good, diagnosis is very important for the detection and course of the disease. As seen in Fig. 2.3, rapid diagnostic tests are offered as public service. The most humane approach in the fight against AIDS is the production of vaccines and drugs that are still in the experimental stage in the public sphere (Saqaklioglu 2006).
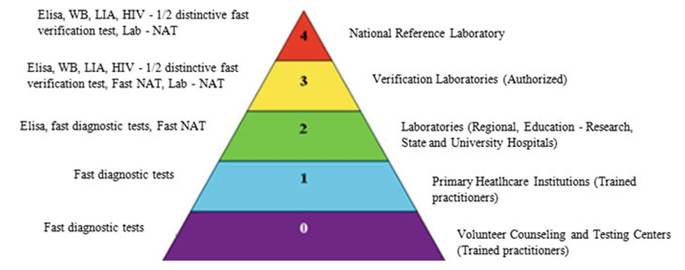
Fig. 2.2 Level based test centers and the responsibilities of laboratory. Source (By using WHO 2015, TR. Ministry of Health, 2019)
In Turkey, among the main duties of the Turkish Ministry of Health is “to perform preventive, curative medicine and rehabilitation services by fighting infectious, epidemic and social diseases”.[5] In addition to the health services provided to the patients by the Ministry of Health, in-service trainings (such as Epidemic Intelligence Service, Basic Training Courses, Extended Immunization Program Trainings) are provided under investment current expenditures for the purpose of infectious disease surveillance and control (Durusoy et al.
2011).Upon the publication of “HIV/AIDS Control Program (2019-2024)” and “HIV/AIDS Diagnosis and Treatment Guideline 2019” by the Turkish Ministry of Health, the effort to strengthen the fight against disease is revealed. In addition, patients diagnosed with HIV/AIDS in Turkey (regardless of whether they already have insurance) can benefit from examination and innovative treatment services free of charge within the scope of Global Health Insurance (T.C. Saglik Bakanligi 2019).
Public spending on health can be increased by increasing the financial capacity of governments, collecting more taxes, or prioritizing health spending from the government budget. The health ministries of the countries should work in an intervening and active manner in the framework of the budget, public financial management systems, and fiscal space/opportunities, together with the ministries of finance. Investments on HIV/AIDS should support the fair distribution of public resources devoted to combating HIV (WHO 2016).
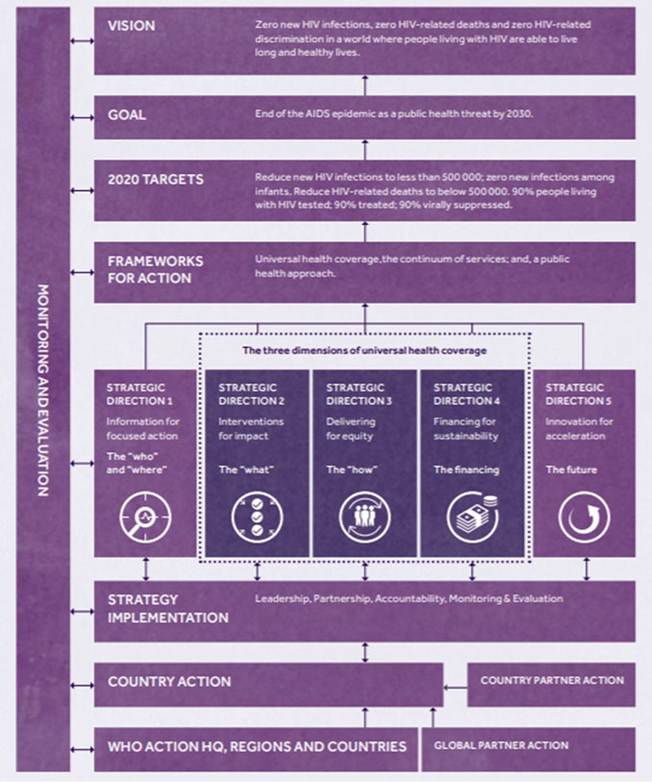
Fig. 2.3 Global health sector strategy (2016-2021). Source WHO (2016)
2.1