CHAPTER 3 Tuberculosis
Tuberculosis (TB) is an ancient disease that probably emerged in humans with the domestication of animals some ten thousand years ago at the start of the Neolithic period. Tuberculosis, like smallpox, is a crowd-dependent disease, needing a critical mass of victims in order to become endemic in a population; this would have been achieved in both animals and humans only when herds and cities would have created the prerequisite densities and contacts required.
It seems that the crossover from animals to humans in tuberculosis occurred with our domestication of goats rather than cows, since the goat strain of Mycobacterium bovis that causes the disease in animals is more closely related to the human bacterial agent Mycobacterium tuberculosis than is the strain in cows.1 However, it is entirely possible that tuberculosis occasionally afflicted Paleolithic man, since Mycobacterium tuberculosis has been discovered in the remains of a seventeen-thousand-year-old bison.2 As with smallpox, the physical evidence of tuberculosis has been found in ancient Egyptian mummies and other Neolithic burial remains, particularly in the bone decay produced in their spines, giving them a humpbacked appearance. The ancient Greeks called the disease phthisis, which Hippocrates in his Aphorisms described as a wasting illness characterized by such symptoms as the coughing up of bloody sputum, loss of hair, and diarrhea. In the Middle Ages, tuberculosis was commonly referred to as scrofula or the “king's evil,” in which the swelling of the neck caused by inflamed lymph nodes was believed to be curable with the miraculous touch of the royal hand, as was claimed by both the kings of France and England.But it was not until the modern era that tuberculosis apparently reached epidemic proportions in Europe. At the end of the Middle Ages, in the late fifteenth century, tuberculosis was already the leading cause of death among the monks of Christ Church Priory in Canterbury, England, accounting for almost a third of all cases of disease diagnosed in the community.3 By the seventeenth century, hospital and other records indicate that “consumption,” as the disease became known at this time, caused a fifth of all deaths in Britain, and perhaps as much as a quarter of Europe's population was infected by the disease.4 It should be no wonder, then, that the English author John Bunyan should famously call consumption the “captain of all these men of death” in his fictional biography The Life and Death of Mr.
Badman published in 1680. By the next century, consumption was thought to be causing fully a third of all deaths in Europe, and mortality and morbidity from the disease probably peaked at the end of the eighteenth and during the first half of the nineteenth centuries, before beginning a long, slow decline from the 1860s on the Continent and from the 1870s in Britain.5The bacillus responsible for tuberculosis was not discovered until 1882 by the German physician Robert Koch (who in the next year also uncovered the Vibrio bacterium that causes cholera). Koch's claim to have found a cure for tuberculosis, a solution containing killed bacteria that he called “tuberculin” and which he unveiled in 1890, proved to be premature, but it did form the basis for a skin test of the disease that is used to this day for diagnostic purposes.6 (Only those who have been infected will develop an allergic reaction to tuberculin.) A true cure for TB had to wait until 1943, when the first of the antibiotic drugs effective against the disease, streptomycin, was discovered by a Rutgers University biochemistry professor, Selman Waksman, and his laboratory assistants, Albert Schatz and Elizabeth Bugie.7 This was later followed by other drugs that are now frequently used in conjunction with streptomycin to treat tuberculosis, including para-aminosalycilic acid (PAS), isoniazid, and rifampin. In the meantime, a vaccine for tuberculosis was developed by two Frenchmen who headed up the Pasteur Institute at Lille, Albert Calmette and Camille Guerin, who first tested their formula containing an attenuated form of the tuberculosis bacillus, known as bacille Calmette-Guerin (BCG), in 1921. Even now, however, after nearly a century of trials, there is considerable debate among medical experts as to whether BCG does, in fact, provide any effective immunity; some contend it actually does more harm than good by making it difficult to diagnose whether a patient has active or latent TB.8 It did not help that, early in BCG's history, a batch contaminated with live tuberculosis bacteria was mistakenly given to 249 babies in Lübeck, Germany, in 1930, with disastrous consequences.
Tragic accidents like this one continue to be the bane of modern vaccination programs down into quite recent times, such as the association of a 1976 swine flu vaccine in the United States with a rare paralytic disease, Guillain-Barre syndrome (see chapter 5).Yet, the steady decline of TB for almost a century prior to 1943 does pose something of a mystery. How could this happen in the absence of antibiotics? Before 1882, doctors did not even have a clear understanding of the real causes behind tuberculosis. Contagion was accepted by some, just as it had been with respect to plague since the Middle Ages, but this had to compete with other explanations, including heredity; social/moral behaviors that could predispose a person to the disease, such as alcoholism or promiscuous sexual intercourse (resulting in syphilis); and a host of environmental factors, including poor hygiene, stress, overcrowding, and poverty.9 Even after Koch's earth-shattering discovery of Mycobacterium tuberculosis, debate continued as to just how the microorganism was communicated person to person; we in fact know that environmental factors such as overcrowding do make one more susceptible to tuberculosis, as the disease is rampant today in prison populations, particularly in Russia, where prisoners must sleep in shifts since there are as many as three inmates for each bed in a cell.10 Belle Epoque Frenchmen were quite right to campaign against spitting as a hygienic measure against tuberculosis, as we now know that the bacterium, in its dried form, can more easily penetrate to alveolar sacs deep inside the lungs carried on dust particles stirred up in the air rather than in larger liquid droplets emitted by contacts, and poverty naturally makes such conditions more likely.11 We also know from recent experience that TB can behave like an opportunistic infection glomming on to other diseases, particularly AIDS, that are largely based in social and moral behaviors.12 Finally, since it is as yet imperfectly understood why only one in ten people who are infected with the bacterium actually develop full-blown TB, while in the rest of the population the invading organisms are “walled off” in the lung in caseous or fibrous nodes known as “tubercules,” there still seems to be a role to play by individual predispositions, such as heredity.13
Even by the standards of what was known at the time, preantibiotic treatment of TB was woefully ineffective.
Bleeding was a standard medical response right up until the mid-nineteenth century; it is sometimes claimed that a phlebotomy could alleviate the symptom of haemoptysis, or the coughing up of blood from the lungs, which was taken as a sure sign of tuberculosis (made famous by the self-diagnosis of the English poet John Keats, who called the blood on his pillow “my death warrant”). However, I know from my own personal experience with this symptom (the result of chronic bronchiectasis, not tuberculosis) that only antibiotics can truly alleviate it, as the seeping of blood into the lungs will persist so long as bacterial infection remains and inhibits the healing of any scarring into the blood vessels surrounding the alveolar sacs. But starting in the second half of the nineteenth century, the sanatorium movement began to take over as the preferred method of treating the tubercular, first in Germany and then in Switzerland, where the resort at Davos became the most famous, visited by international luminaries, and that served as the setting for the novel by Thomas Mann, The Magic Mountain. By the end of the century, these were joined by the “cottage system” of Saranac Lake in the Adirondacks in upstate New York, founded by a physician who was himself suffering from the disease, Edward Livingston Trudeau.The early sanitoria operated on the principle that a supervised regimen of rest and mild exercise in the bracing mountain air, supplemented by a nourishing, if not gluttonous, diet of at least three full meals a day would give the body an opportunity to exert its own natural healing powers and effect a cure of tuberculosis. The principle was not a new one, as it could be found going back to at least ancient times, and the idea of retreating to a special climate for tuberculosis was the fashion among consumptives in the earlier part of the century who favored the warmer climes of Italy, southern France, or Spain. Trudeau's famous experiment with rabbits notwithstanding, it is not clear that the sanitoria did much beyond confirm the natural progression of the disease in the patient; not even the much vaunted benefit of isolating patients from the general population is as clear cut as it might seem.
Patients were usually released after a six-month period, when they were still very much infectious, and only a small minority ever had the privilege of visiting the sanatoria in the first place, as these were usually limited to early, “curable” cases of the disease or to those who could afford to pay, although some charitable institutions were set up in Britain and the United States, which survived on donations or the free labor of their inmates.14The last phase of tuberculosis treatment before the advent of antibiotics was perhaps the most brutal and was not any more demonstratively effective: this was the “collapse therapy” of performing an artificial pneumothorax on the patient by inserting a hollow needle into the pleural cavity of the chest and introducing a measured amount of air in order to collapse the lung. (Sometimes injections of paraffin wax or oil were substituted for air to try to make the collapse more permanent.) Although the procedure was first introduced during the nineteenth century, it reached the height of its popularity during the 1920s and 1930s and was based on the same theoretical principles as the sanatoria (where most pneumothorax operations took place): that the lung would benefit from a resting period when it would allow itself to heal. Although a collapsed lung would, in theory, deprive the bacteria of oxygen needed for growth, this was a dangerous procedure prone to complications, such as a gas embolism in the circulatory system when the needle was not inserted correctly, which could result in death. It was also not painless, especially after the effects of local anesthetic wore off, when patients commonly described the feeling of having a “mule kick” or a “knifelike pain” delivered to their chest, and it was a procedure that had to be repeated with “refills” of air injection on a regular basis if the lung was to remain collapsed for long periods. In frequent cases where the lung adhered to the pleura due to the normal fibrous scarring of tuberculosis, open chest surgery had to be performed, with even greater risks of fatal side effects.
At its most extreme, this surgery entailed removing part of the rib cage entirely, a procedure known as thoracoplasty, and cutting or removing the phrenic nerve, which paralyzed the diaphragm, in order to achieve permanent collapse, but patients ran a high risk of severe blood loss and shock. Overall, what follow-up studies were done of pneumothorax and thoracoplasty surgery showed that 50 percent or less of patients were still alive a few years later to justify such radical intervention; in a large minority of cases, it was estimated that it was completely unnecessary to the patients' chances of recovery.15Given these dismal results, it still remains to be explained why incidences of tuberculosis continued to decline even before proven antibiotic treatments took effect. The most likely explanation is the general improvement in living standards of populations in the West during the second half of the nineteenth and first half of the twentieth centuries, including better housing, diet, work conditions, and so forth.16 This makes sense if one considers that the height of the tuberculosis epidemic during the hundred years or more just prior to its protracted decline coincided with the rise and advance of industrialization in Western countries, with its attendant environmental degradation, dramatic shifts of population from rural to urban settings, and untrammeled exploitation of workers, especially children.17 This is further indicated by setbacks to the disease that occurred when living standards temporarily fell in times of crisis or national emergency, such as during the First World War. The bare fact of this decline, more than almost any other aspect, demonstrates that tuberculosis was, and remains today, a “social disease” that depends on more than mere biology for its behavior in a given population.
Yet another efflorescence of tuberculosis's dependency on societal factors is the romantic reinvention of “consumption” during the early nineteenth century, when it was in very great danger of being nearly perceived as not a disease at all. One could in fact say that consumption at this time became almost fashionable, when it was imagined that one could simply waste painlessly away into a version of Keats's “easeful death” (the reality, as patients drowned in their own blood or gasped frantically from air hunger, was obviously quite different), and apparently some even wished to get sick in order to acquire the delicately pale looks so admired in consumptives and that even today seem to be strived for by bulimic fashion models.18 By the end of the nineteenth century, consumption had lost most of its romantic associations, signified by the mere fact that the more prosaic term of “tuberculosis” was coming into greater usage, which was probably a function of the increasingly scientific approach to the disease following Koch's explication of its bacterial cause and of the fact that poverty was being seen more and more as the natural environmental context of tuberculosis. But until then, consumption touched the lives of many of Europe's leading artists of the romantic period, including Keats, Percy Shelley, Frederic Chopin, Robert Schumann, the Bronte sisters, Robert Louis Stevenson (who was a patient at both Davos and Saranac Lake), and, in the United States, Edgar Allen Poe, Ralph Waldo Emerson, and Henry David Thoreau.19 Even though many an artist's life span was prematurely cut short by the disease, it was widely believed at the time that their genius actually benefited from feverish bouts of activity induced by consumption, and indeed it is entirely possible that the tragically doomed creators' awareness of their impending demise lent a sense of urgency to their work. Tuberculosis also has a starring role in much of nineteenth-century literature, afflicting the characters of Charles Dickens, Victor Hugo, Anton Chekov, and Fyodor Dostoyevsky. Aside from Mann's Magic Mountain, perhaps the most well-known example is Alexandre Dumas fils's The Lady of the Camillias, in which tuberculosis claims its selfsacrificing heroine, Marguerite Gautier (based on Dumas' acquaintance with an actual courtesan who died of consumption at age twenty-three, Marie Duplessis). Dumas' novel and subsequent play became the inspiration of Giuseppe Verdi's opera La Traviata and in more modern times of the films Camille (1936), starring Greta Garbo as Marguerite, and Moulin Rouge! (2001), starring Nicole Kidman as Satine, a character clearly based on Marguerite.
An interesting footnote to this cultural aspect of tuberculosis is the disease's contribution to the vampire legend, particularly in New England. Sometimes, the decomposition of the body after death, which in the case of a disease like tuberculosis is most pronounced in the lungs, can apparently result in blood seeping from the lips, giving the impression that the corpse is still alive and achieves this feat by feasting on victims.20 Added to this would be the suspicious circumstance, especially in an age that imperfectly understood disease contagion, of several members of a family succumbing to consumption within a relatively brief period of time. The allegedly voracious sexual appetite of tuberculosis victims may have also contributed something to the infamously sensual aspect to the legend. From the late eighteenth through to the end of the nineteenth centuries, in Rhode Island, eastern Connecticut, and my home state of Vermont, the graves of both men and women were disinterred in order that a ghastly ritual might be enacted upon the occupants, which was believed to have the power to end their supernatural scourge: this consisted of none other than cutting out the heart (often described as full of blood) of the exhumed victim and burning it to ashes nearby. It seems that nearly all of such “corpse killer” incidents were initi-
ated by consumption running rampant through a family, giving rise to the belief that one of the deceased was now preying on the remaining members who were sickly but still alive. Part of this ritual apparently included a healing rite in which the ashes of the suspected vampire were fed to the ailing family member in the hopes that this might yet save his or her life. In at least one instance, that of Mercy Brown of Exeter, Rhode Island, whose months-old body was violated in March 1892 in an attempt to save her brother, Edwin, who likewise was to succumb to tuberculosis, this ritual occurred almost exactly ten years to the day from when Koch had announced his discovery of the bacterium that was truly sucking the life force from consumption victims.21 On my own farm in Vermont, one can still see the traces of such desperate attempts to escape tuberculosis when walking in the woods, only to suddenly stumble upon abandoned stone walls and cellar holes that stand like ghostly sentinels to their former inhabitants’ retreat halfway up the mountain in search of healthier air.
The romantic disposition of tuberculosis stands in evident contrast to that of plague and smallpox, and also of cholera. The reason for this is not hard to find: I believe it can be traced back to the physical symptoms of each disease. We have already seen how bubonic plague and smallpox can cause horribly painful and disfiguring eruptions on the body; both diseases can also be terrifyingly swift and sudden in their assault on the body’s defenses. We will also see that cholera is devastatingly rapid in its progression and produced symptoms that were particularly repulsive to nineteenth-century Western sensibilities. By comparison, tuberculosis could lie hidden and dormant, scarcely noticed by the victim, for years, and, when and if it did finally emerge from its latent phase into a virulent one, it typically caused the “pale, wan, frail look” (hence the name by which tuberculosis was commonly known, the “white plague” or the “white death”) that actually was admired and aspired to by fashionable beauties for at least the first half of the nineteenth century. Even the most visible symptom, the coughing up of blood, could apparently be discreetly hidden, until perhaps the very end, by a strategically placed handkerchief. Thus, tuberculosis was, for much of its romantic history it seems, the perfectly acceptable disease from which to die. The interconnectedness of the clinical and societal aspects of tuberculosis illustrates the fine line to be drawn between positivist and relativist interpretations of disease.
The latest chapter in the history of tuberculosis, which is still being written, is the emergence within the last few decades of epidemics of a multi-drug-resistant strain of the disease (known by its acronym as MDR-TB), and now an even extensively drug-resistant variety (XDR-TB). This is when TB bacteria, which are hard to kill because of their waxy coating, develop resistance to one or more antibiotic drugs by means of genetic mutations. (Keep in mind that hundreds of millions of these bacteria are usually present in a victim.) Such a scenario arises only when treatment regimens for TB fail to eliminate all bacteria that have been exposed to the drugs being used (which is said to be usually the fault of the doctor rather than the patient). Any number of circumstances may be responsible: the patient does not complete the full course of treatment (the usual “short course” of a combination of TB drugs lasts six to nine months); the doctor prescribes the wrong or insufficient dosage of drugs to correctly treat the patient's TB; the drugs have been manufactured badly (such as in a form that cannot easily be absorbed by the patient or with not enough active ingredient); or treatment centers, particularly in Russia and the third world, do not have enough drugs to allow patients to complete their recommended course. In essence, the patients now become an incubator for a far more deadly form of the disease than before they started treatment, and they can now pass this form on to other victims. It is perhaps no coincidence that, at the very same time that MDR-TB was arriving on the scene during the 1980s, a frightening, new disease called AIDS started taking its toll, which, as we will explore in more detail in chapter 6, destroys the body's immune system; AIDS makes it easier for the patient to not only contract TB but also become an incubator of MDR-TB. (Currently, tuberculosis is the most common “opportunistic infection” that actually kills off patients with AIDS.) As the first decade of the twenty-first century comes to a close, the World Health Organization (WHO) reports that a third of the world's population is currently infected with TB, with one new person becoming infected every second, and that 5 to 10 percent of those infected will go on to develop an actively virulent form of the disease. As of 2005, southeast Asia had the highest number of cases, nearly three million, or 34 percent of the world's total, followed by Africa with two and a half million, or 29 percent of all cases globally; it is no accident that these places also have some of the highest incidences of AIDS. TB strains resistant to at least one antibiotic drug have been documented in every country surveyed by WHO, and strains that are resistant to all major antibiotic drugs have by now emerged. More usually, MDR-TB is defined by WHO as strains resistant to the antibiotics isoniazid and rifampin; it is most prevalent apparently in the former Soviet Union.22
The case that is usually cited in the literature to illustrate the current MDR-TB crisis is an epidemic of both regular and MDR tuberculosis that occurred in New York City from approximately the mid-1980s to the mid-1990s.23 At the height of the epidemic in 1992, New York had nearly four thousand TB cases, comprising 14 percent of all cases in the United States, a third of which were MDR-TB, comprising 61 percent of those in the country at large. Moreover, 23 percent of patients contracted MDR-TB without ever having been treated before, proving that the drug-resistant strain was spreading independently of its “home-grown” origins, and over 40 percent of New York's TB patients were also infected with AIDS. Whereas TB infection rates had previously been falling or holding steady, the number of cases tripled in that one year. Yet, most see the origins of the crisis as going back to the 1970s, when the U.S. Congress stopped setting aside money solely for fighting TB and allowed states to spend it at their discretion. In most places, including New York, other priorities took precedence out of a sense of complacency that epidemic TB was a thing of the past, a victory celebration that proved premature.
Eventually, New York City's TB epidemic was brought under control, largely through a policy known as directly observed therapy (DOT), in which patients complete their drug course under supervision, and which has now been adopted by WHO as its preferred method for treating TB. For MDR-TB, this strategy must be tailored to the patient by first testing to determine which drugs the bacteria are immune to and then prescribing specific second-line drugs against them, a regimen known as DOTS-plus (the acronym stands for directly observed therapy short course). Using the DOTS technique, New York City's health department was able to reverse the poor compliance rates for completing treatment, which had stood at less than half of all patients at the height of the epidemic and in some places, such as Harlem, was as low as 11 percent. By the mid-1990s, compliance rates were now at 90 percent and cases of MDR-TB saw a correspondingly dramatic decline, down 91 percent.24
But this remarkable achievement came at a price, and not just in monetary terms of the one billion dollar price tag for the program; although most patients completed treatment voluntarily, after signing a contract agreeing to do so that was sweetened with incentives such as free medications and food and transportation coupons, a tiny minority—forty-seven patients in all—had to be coerced into completing treatment by being detained in special wards at hospitals, such as the twenty-five-bed facility at Goldwater Memorial Hospital on Roosevelt Island. New York City's health code was amended in 1993 to allow for such detention in cases of active tuberculosis where it was deemed there was a “substantial likelihood” that the patient might transmit his or her TB to others and would not complete treatment, based on “past or present behavior.” Some argue this was nonetheless a “sensitive solution” since patients had the right of appeal and were even provided free legal counsel; moreover, the mere threat of detention was perhaps a persuasive tool for voluntary compliance, thus obviating the need for enforcement in many cases, although no hard evidence has been produced to this effect.25 However, others insist this was an unprecedented infringement of liberties, since it was based on the principle of noncompliance rather than an immediate and quantifiable threat to the public health, as was the previous standard with all mental illnesses and other contagious diseases, and since less restrictive alternatives were not tried beforehand.26
Historical parallels have been drawn with comparable dilemmas in the past, such as the infamous “Typhoid Mary” case, in which the New York City health department forcibly detained an Irishwoman, Mary Mallon, in quarantine at a hospital on North Brother Island for the last twenty-three years of her life between 1915 and 1938 because she was a healthy but highly infectious carrier of typhoid fever. Although some might consider Mary's fate to have been cruel, she did infect a total of fifty-three people (three of whom died) during her career as a cook. (Typhoid, like cholera, is spread through contaminated feces, which Mary would have had on her hands since hand washing was not widely practiced at the time.) After her first period of incarceration from 1907 to 1910, Mary was granted her freedom despite a court ruling that upheld her detention in the face of a habeas corpus legal challenge filed by a lawyer on her behalf; her release was on condition that she sign an affidavit promising to cease employment as a cook, a condition she subsequently violated under an assumed name (at a hospital, no less). Yet, there is more to Mary's case than simply the biological issue of protecting the public from deadly germs, for it does not explain why hundreds of other healthy carriers besides Mary were allowed to go free, including a “Typhoid John” in the Adirondacks who infected thirty-eight victims, two of whom also died. An indefinite, involuntary detention of a healthy person as a public health threat was in fact unprecedented. It seems that the New York board of health was determined to make Mary an example of how someone who was in perfect health could nonetheless be a walking carrier of disease; Mary's misfortune was simply to be the first such healthy carrier to be so identified. Moreover, as a single, female, sexually active, working-class Irish immigrant with a physically imposing presence who refused to cooperate with authorities or even admit she was a carrier, Mary also posed a social threat to contemporary preconceptions of acceptable feminine behavior; she certainly did not get along with George Soper, the sanitation engineer who first tracked down Mary and who came from a middle-class, Protestant, educated background, almost the exact opposite of hers.27
If we go just a little further back in history, we have already seen that Britain's attempts to take extraordinary measures to combat plague in its empire in India at the turn of the twentieth century encountered widespread opposition among the native population there, to the point that they were rendered almost counterproductive (chapter 1). This was partly the result of a lack of conviction that these efforts were truly effective and partly because they ran counter to traditional cultural values and domestic sensibilities. It could be argued that, in this day and age, transmission of a disease like tuberculosis is far better understood and that modern Western culture is far more accepting of the authority and encroachments of medical science into our daily lives. The courts, press, and the public at large all, with few exceptions, seemed to endorse NYC health department's drastic actions taken ex officio to combat MDR-TB, the threat of which seemed to far outweigh any constitutional objections that might appeal to tender consciences. But we must remember that only a few people on the margins of society were directly affected; what would happen if large numbers from mainstream society had to be coerced, and if close family members had to be separated in the process? Although such scenarios might be the fodder for simulation exercises and Hollywood films, they have yet to be tested in the real world.
Despite New York City's success story, the way forward in the campaign to eradicate TB is far from clear. Not everyone, for example, is enamored of the DOT approach; in Russia, which has the third largest number of MDR-TB cases in the world, largely owing to its severely crowded prison system that serves as an incubator for the disease, there was much cultural resistance to DOT until relatively recently. This was because many in the Russian Ministry of Health were convinced of the necessity to go back to the old, Soviet method of treating TB, which operated on a ponderous, case-by-case basis that relied primarily on X-ray diagnosis and surgery.28 Perhaps for reasons of sheer national pride, Russia's reluctance to adopt DOT was not overcome until 1995, and even then universal, countrywide application of DOT was not to be achieved until 2007. Not coincidentally, it was not until the last decade that the growth rate in number of new TB cases has finally slowed in Russia. Yet, problems remain, including ineffective detection and notification of new cases, poor compliance and success in DOT administration, spectacularly high TB rates in prisons (where overcrowding and poor air quality conditions remain despite attempts at reform), and considerable coinfection with HIV (human immunodeficiency virus).29
Others suggest that DOT demands an allegedly too “paternalistic” and “authoritarian” approach to compliance for some cultures and that alternative treatment methods should therefore be considered, such as voluntary administration of “fixed-dose drug combinations” (which presumably would encourage completion of treatment through the ease of taking just one pill).30 Developing and getting new drugs to market that may be effective against TB is often a challenge when drug companies see “a high investment with little commercial return,” since “the vast majority of people with TB are young and poor and live in developing countries.”31 (This is the subject of the 2005 film The Constant Gardener.) Recent sequencing of the TB genome holds some promise for targeting “hibernating” bacteria that can lie dormant in the body and thus resist antibiotics, only to be reactivated at a later time, but the full fruits of this research are probably years away. More promising in the near term is perhaps efforts under way to develop a more effective BCG vaccine, which would allow for targeted eradication on the model of the successful campaign against smallpox.32
Then there are underlying causes of TB, such as poverty, which are far more intractable problems to solve, especially since TB and poverty are closely linked in a mutually reinforcing cycle: TB is said to flourish in the overcrowded, malnourished, unhygienic environments that poor people are most susceptible to, while at the same time the disease hits poor families the hardest in terms of lost wage income and increased expenses for medical treatment, often as the result of delayed and incorrect diagnosis.33 Yet, with the many possibilities of global spread of TB (such as on airline flights), the current crises in poorer nations simply cannot be ignored by richer neighbors. Since TB can be spread so rapidly and easily, with one contact potentially infecting dozens of others in short order, time is of the essence in the fight against the disease. Much of this challenge is of humankind’s own making, particularly in the case of MDR-TB, where ironically the cure is also our curse. But the consensus seems to be that society can conquer TB, if only it can muster the will, money, and ingenuity to do so.
Burial of a plague victim from the Al Maqamat (The Meetings) by Al-Hariri, Persian school, fourteenth century. Getty Images
Smallpox epidemic in Mexico. Aztec natives with smallpox contracted from Spaniards are ministered to by a medicine man. Illustration from Father Bernardino de Sahagun's sixteenth-century treatise, A General History of the Things of New Spain. The Granger Collection, New York
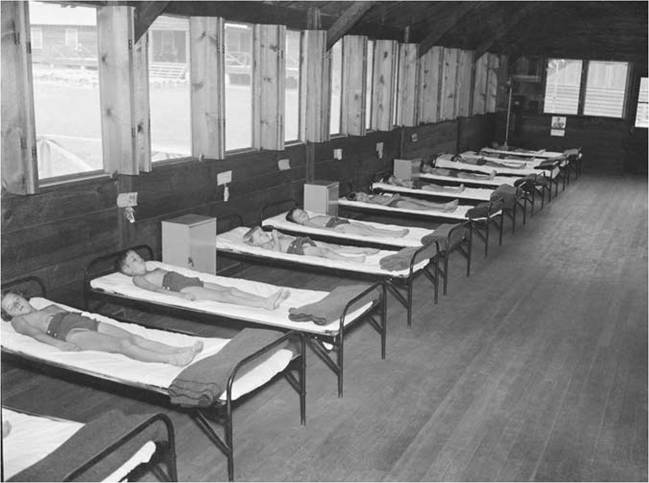
Tubercular children taking enforced rest for fifteen hours each day at a tuberculosis camp in Washington, DC, in 1938. Note the many wide-open windows designed to let in fresh air. © Bettmann/CORBIS
Bodies of Rwandan refugees, who died in a cholera epidemic that spread through refugee camps at Goma in July 1994, await burial in a mass grave near Kibumba camp, Zaire. © Howard Davies/CORBIS
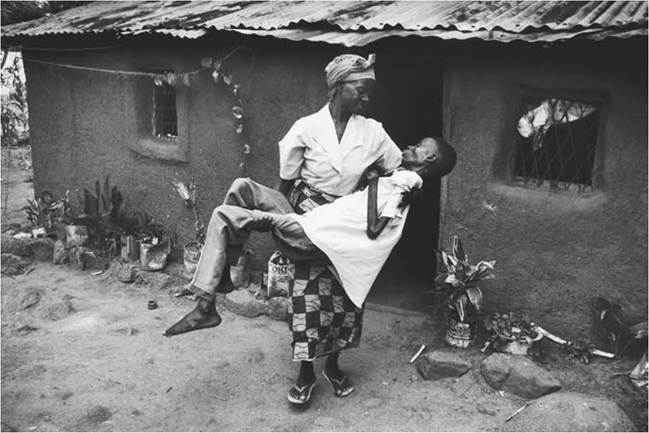
A Tanzanian mother carries her thirty-year-old son, Joseph, who is ill with AIDS, outside to sit in the shade, c. 2000. © Gideon Mendel/CORBIS
More on the topic CHAPTER 3 Tuberculosis:
- Chapter 23 Bovine Tuberculosis in Zambia
- Chapter 18 Bovine Tuberculosis in Rwanda
- Chapter 15 Bovine Tuberculosis in Ghana
- Chapter 13 Bovine Tuberculosis in Egypt
- Chapter 9 The Diagnosis of Bovine Tuberculosis
- Chapter 5 Tuberculosis in African Wildlife
- Chapter 16 The Status of Bovine Tuberculosis in Malawi
- Chapter 12 The Status of Bovine Tuberculosis in Cameroon
- Chapter 10 The Control of Bovine Tuberculosis in Africa
- Chapter 7 Epidemiology of Bovine Tuberculosis in Africa
- Chapter 6 The Mycobacterium tuberculosis Complex in Africa
- Chapter 21 The Changing Landscape of Bovine Tuberculosis in Tanzania