On plague in a time of Ebola
Cormac O Grada
University College Dublin
Before COVID-19, the last epidemic to command global attention was the 2014-15 Ebola epidemic. Ebola made the headlines for its highly infectious character, its high fatality rate, the lack of any known cure for it, and the grave risks that it posed for health workers and third parties.
The fears that it generated and the strict public health measures that it prompted echoed responses to the medieval Black Death and the third plague pandemic that originated in China in 1855.Ebola and plague (Yersinia pestis) have rather similar incubation periods and both cause painful and distressing deaths. Indeed, for a time in the 2000s, some experts believed that Ebola was a form of plague. Ebola is transmitted from person to person; whereas that is literally true of only one rare and highly lethal form of plague, pneumonic plague, the relatively recent finding that plague can be transmitted by body lice - and does not require the presence of rats and rat fleas - implies a route approximating transmission from person to person. Both diseases led to discoveries of a medical remedy - rapid in the case of the third plague once the bacillus responsible had been discovered, and similarly rapid in the wake of the 2014-15 crisis, with the preparation for use of the (previously discovered) VSV-EBOV vaccine. These common characteristics, coupled with the current spread of COVID-19, prompt the following reflections about plague and Ebola, even though the second and third plague epidemics dwarfed the 2014-15 Ebola outbreak in terms of mortality. I review the mortality due to the two diseases and their lethality, the role of public action in containing them;,and their economic impact.
Deaths from plague and Ebola
At the outset, alarming projections were made about the mortality implications of the likely spread of Ebola in western Africa and beyond, with econometric simulations forecasting that if the disease spread, one million or more would die ‘in the next six months’.
The World Health Organization’s mid-October 2014 forecast of 10,000 new cases weekly was more modest, though it still dwarfed the actual cumulative out-turn of about 30,000 cases and over 11,000 deaths (roughly 0.05% of the combined population of the three affected countries, Guinea, Liberia, and Sierra Leone). Summary data are presented in Table 1 and Figures 1a and 1b.Whereas demographic data on Ebola are plentiful, historians of the Black Death have very little solid data to work on. However, a compromise guesstimate suggests that the successive outbreaks of the Black Death c. 1348-1700 reduced Europe’s pre-plague population of about 80 million by around half. By and large, lower populations entailed higher wages and lower rents. Hard data on the lethality of the Black Death are also lacking, though it probably fell over time. Today, WHO reckons that half of those struck by plague recover without the aid of any medical treatment. During the 2014 outbreak of bubonic plague in Madagascar, 119 confirmed cases resulted in 40 deaths; an outbreak in August-September 2015, this time of the pneumonic form, killed 10 out of 14 victims. The fatality rate from Ebola in 2014-15 was much lower than from untreated plague.
Table 1 The Ebola epidemic: Cases and deaths
| All | Health workers | |||||
| Cases | Deaths | % | Cases | Deaths | % | |
| Guinea | 3,800 | 2,534 | 66.7 | 196 | 100 | 51.0 |
| Liberia | 10,672 | 4,808 | 45.0 | 378 | 192 | 50.8 |
| Sierra Leone | 13,982 | 3,955 | 28.3 | 307 | 221 | 72.0 |
| Total | 28,454 | 11,297 | 39.7 | 881 | 513 | 58.2 |
Source: http://apps.who.int/ebola/current-situation/ebola-situation-report-14-october-2015
A second striking and disturbing implication of Table 1 is the very high proportion - nearly 5% - of native-born health workers among those who died during the Ebola outbreak.
Perhaps the cumbersome procedures involved in ‘donning and doffing’ the highly uncomfortable Ebola protective suits worn by over-stretched health workers led some to take short cuts?Malcolm Casadaban, who died of plague in Chicago in 2009, was a most unlikely victim. A biology professor, Casadaban succumbed to accidental exposure to a strain of the virus in his lab. But although the plague bacillus was blind, the most likely victims of plague have always been disproportionately the poor; well-off people such as the parents and siblings of Florentine merchant Francesco Datini and the two archbishops of Canterbury, who died in rapid succession during the first outbreak of the Black Death, were exceptional among their peers.
Figure 1a Cumulative cases in Guinea, Liberia and Sierra Leone
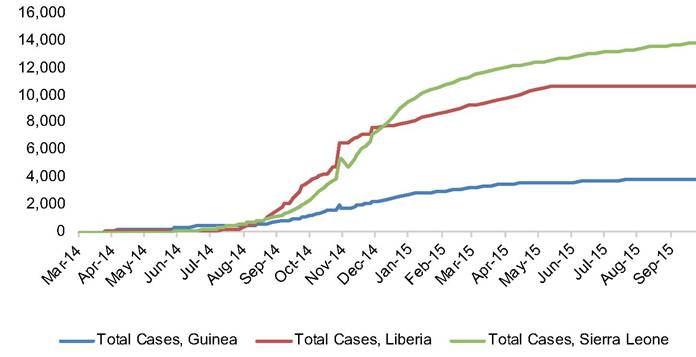
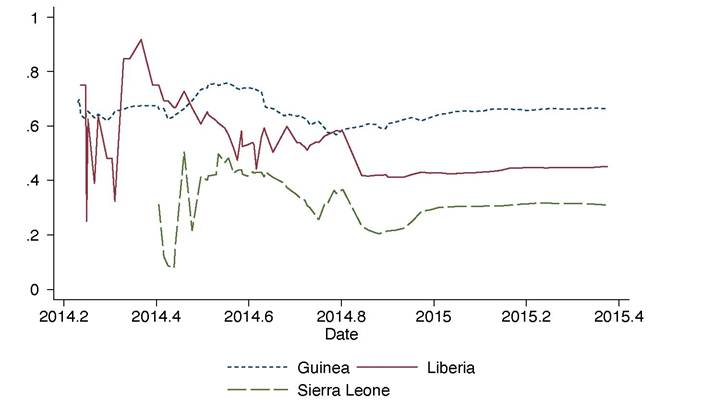
Figure 1b Cumulative death rates (dr) in in Guinea, Liberia and Sierra Leone
Public action
Why did plague recede in Western Europe during the 16th and 17th centuries? Why had it not done so earlier? The most likely reason is increasingly effective public action in the form of quarantining, removing foul-smelling refuse, and draconic measures against infringement. Such action, which is likely to have reduced the likelihood of transmission from fleas (and lice) to humans, required credible sanctions and a degree of public support. The effectiveness of public health measures depended on preparedness, and eliminating corruption in the forms of breaching quarantines, concealing deaths, deliberate misdiagnoses of plague cases, and anti-social behaviour in general.
Its ruthlessly effective Visconti rulers saved Milan from plague in 1348-50. In Milan, the conviction - not prevalent at the time - that plague was contagious led to efforts to control the movements of contacts. But public action can claim few other victories in 1348-50.
Quarantining and maritime cordons came later; the first Iazaretti (pesthouses) were those in Ragusa (1377) and Venice (1423). The policy of isolating suspected plague victims in such places, while based on the (false) presumption that the disease was spread only from person to person, may well have worked to the extent that Iazaretti were located in less flea- and rat-infested places; but the English policy of shutting healthy people in their homes when a death had occurred instead of allowing them to escape infection may well have been counterproductive. Municipal action such as the funding and enforcement of quarantines and the banning of processions reduced the threat of plague in parts of 17 th century Italy. Other institutional responses to plague included the London Bills of Mortality (published continuously from 1603) and bans on processions and other large congregations of people.On the eve of the Ebola crisis, Sierra Leone had 0.022 physicians per 1,000 inhabitants, Liberia 0.014, and Guinea 0.115. Although the medics behind these numbers did not know how to cure either plague or Ebola, the numbers also reflect broader medical infrastructures. All three affected countries were much poorer than, say, 17th century Italy or England, though they had also been growing much faster in recent years.
The goal of international relief in 2014-15 was to compensate for frail public health infrastructures and widespread destitution. However, given the huge transfers involved, corruption was inevitable. In November 2014 in Sierra Leone, when health workers protested violently at not being paid, all a spokesman for the National Ebola Response Centre could offer was that “somebody somewhere needs to be investigated (to find out) where these moneys have been going”.
The disease had already killed about 60 people in Guinea when it was identified as Ebola on 22 March 2014. At that time, WHO characterised it as “an outbreak of limited geographic area and only a few chains of transmission”, and this assessment tallied with evidence on earlier outbreaks of Ebola in central Africa.
However, by late May the disease had reached Sierra Leone and on 8 August 2014, by which time the death toll had reached nearly one thousand, WHO declared the outbreak an “international health emergency”. In the following weeks, alarming forecasts of the likely death toll from Ebola spurred the international community to action. By May 2015 such transfers exceeded $3 billion, more than 30% of the combined GDP of the three recipient economies.Still, there was plenty criticism of the response to the outbreak, at home and abroad. Medecins sans frontieres, who provided most of the frontline defence against Ebola at the outset, accused the authorities in Guinea and Sierra Leone of seeking to conceal the outbreak and WHO of prevarication.
Containment and cure
The Ebola outbreak inspired fear and panic because of its lethality, its long incubation period, and the lack of a medical cure. The virtual elimination of plague as a threat across most of the globe relied on preventive rather than curative measures, and it took centuries for those preventive measures to become fully effective. One of the main defences against its spread, quarantine, involved isolating victims for a biblical 40 days - a big multiple of plague’s incubation period of two to six days (which, of course, was not known at the time). In the absence of a cure, quarantine was also a key weapon against Ebola: a precautionary 21-day quarantine for those who have been in close contact with an Ebola victim.
There was no therapeutic cure for Ebola during the epidemic of 2014-15. One of the dramatic by-products of that epidemic was the final release of a highly effective vaccine, VSV-EBOV, the clinical discovery of which dated back to 2003. Had Ebola struck in the 1890s, it is possible that a similar drug would have been discovered, in which case the authorities would have gambled on its immediate use. Although the crisis was almost over by the time the vaccine was ready for use in July 2014, the speed with which it was developed is nonetheless impressive.
Economic consequences
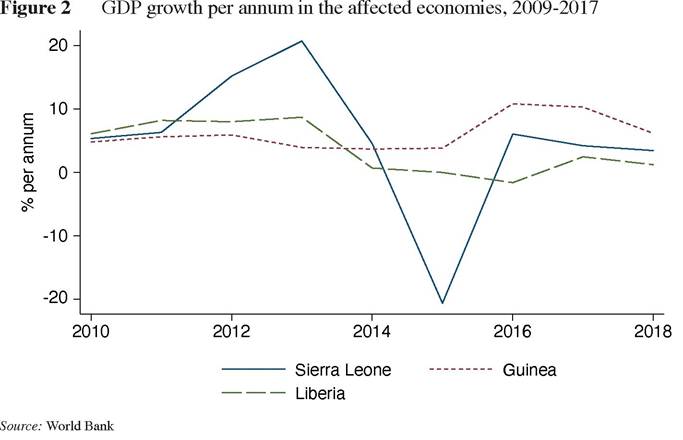
In October 2014, the World Bank predicted that Ebola would cost the affected countries US$25 billion in economic losses in 2015, equivalent to almost twice their combined GDPs and enough to cripple them economically for years to come. By January 2015 that prediction had been reduced to a still significant US$1.6 billion, equivalent to about 12% of combined GDPs. But in the event, the impact of Ebola on the level of economic activity was much smaller. The significant drop in GDP in Sierra Leone in 2014 was mainly due the global collapse in iron ore prices rather than to Ebola.
Analogous estimates of the economic impact of the Black Death are impossible, but elementary economics predicts that an exogenous shock such as the Black Death, which reduces population but leaves the capital stock and other resource endowments intact, should result in reduced output but an increase in wages relative to other factor payments. And undoubtedly, the first attack of the Black Death in western Europe resulted in significantly improved living standards for most survivors, while reducing urbanisation levels and making agriculture more pastoral. Some argue that high wages led to labour-saving technologies such as the Gutenberg printing press. The rather thin evidence available on income or wealth distribution implies a narrowing of the gap between rich and poor. There is also general agreement that it took populations a long time to recover their pre-plague levels, partly because plague kept returning but also because, in some countries at least, of incessant warfare in the following decades and centuries.
Final reflections
Despite the major differences between them, Yersinia pestis and Ebola share many resonances. The campaign to contain and eradicate Ebola - and the attendant red tape and corruption - recalls the varied attempts by the authorities at ridding western Europe of plague. Later efforts to control plague had an international dimension: the work of Odessa-born Waldemar Haffkine in Bombay was funded by the local authorities and by the Aga Khan, and plague’s virtual eradication in pre-independence India owed much to colonial policies. Today, the resources and knowledge available to campaigns against epidemics like plague, Ebola, and COVID-19 are global rather than local. In the case of Ebola, NGOs such as Medecins sans frontieres, institutions such as WHO, and the governments of the countries affected combined in bringing the 2014-15 epidemic under control.
According to WHO data, the epidemic had caused 11,313 deaths up to mid-October 2015, by which time the crisis had been stayed, with only 23 deaths after the end of August 2015. The number was very modest compared to, say, estimates of famine deaths in Somalia in 2011-12 or of deaths from malaria in sub-Saharan Africa in 2014 (0.4 million), yet the global impact of Ebola was far greater.
At the height of the crisis, the Harvard global health specialist Paul Farmer insisted that “if patients are promptly diagnosed and receive aggressive supportive care... the great majority, as many as 90 per cent, should survive”. Easier said than done, given the fears generated by Ebola and the primitive health infrastructures and rickety economies of the counties in question. Yet, how many lives might have been spared by a prompter response or by extra funding remains to be discovered.
About the author
Cormac O Grada is Professor Emeritus of Economics at University College Dublin. Several of his recent publications, on topics ranging from the origins of the Industrial Revolution to London’s last plague epidemics, have been collaborations with Morgan Kelly. His best-known books are Ireland: A New Economic History (Oxford, 1994) Jewish Ireland in the Age of Joyce: A New Economic History (Princeton, 2006), and Famine: A Short History (Princeton, 2009). His latest is Eating People is Wrong and Other Essays on the History and Future of Famine (Princeton, 2015). He is past Editor of the European Review of Economic History.
12
More on the topic On plague in a time of Ebola:
- On plague in a time of Ebola
- Trade and travel in the time of epidemics1
- Appendix B Infection Control and Isolation Recommendations