Clinical Manifestations and Diagnosis of HIV-Associated Pulmonary Hypertension
In the largest clinical series of HIV-associated pulmonary hypertension, 47-54% of all
Table 1 Pathogenetic hypotheses of HIV-associated pulmonary hypertension
Pathogenetic hypothesis
Clinical evidence
Cytokines hypothesis (Fig.
2)αι-Adrenergic hypothesis (Fig. 3)
Toxic substances
Liver disease and HIV-associated pulmonary hypertension
Several studies have found an increased production of cytokines-e.g., endothelin-1 (ET-1), interleukin-6 (IL-6), interleukin-1-beta (IL-1b), plateletderived growth factor (PDGF), and tumor necrosis-factor-alpha (TNF-α)-in patients affected by primary pulmonary hypertension, evoking a potential role of these substances in the pathogenesis of the disease [6-9].
In HIV-infected patients different factors can induce a chronic stimulation of α1-adrenoreceptors of the pulmonary vasculature, including: chronic hypoxia, high circulating levels of norepinephrine, appetite suppressant agents, or cocaine use. The chronic stimulation of pulmonary vascular α1-adrenore- ceptors can induce the local production of a large amount of cytokines, particularly ET-1, IL-1b, IL-6, and PDGF, which in turn stimulate the growth of new pulmonary capillaries, induce vasoconstriction of resistance-sized pulmonary arteries, and have an anti-apoptosis effect [10].
Patients with a history of chronic intravenous drug use may develop pulmonary hypertension. Pulmonary artery thrombosis is the main pathological finding in such conditions, and is believed to be due to foreign particle pulmonary emboli, following injections of solutions derived from heroin or from crushed oral medications in which talc was a frequent component [11, 12].
The use of appetite suppressant agents and/or cocaine has been associated with pulmonary hypertension, even in HIV-infected patients, possibly as a consequence of an increased α1-adrenoreceptor stimulation [12, 13].
Porto-pulmonary hypertension is now a well-described disease characterized by a clinical and hemodynamic picture substantially identical to primary pulmonary hypertension. In liver cirrhosis, an increased production and a decreased metabolism of some cytokines (e.g., ET-1) have been reported.
Kuddus et al. demonstrated that an enhanced synthesis and a reduced metabolism of ET-1 in hepatocytes can be an important mechanism of elevated endogenous and circulating ET-1 in patients affected by liver cirrhosis [14, 15].
Pellicelli et al. reported higher values of systolic pulmonary arterial pressure in HIV-infected patients with HCV/HBV-associated liver cirrhosis compared to other HIV-infected patients without cirrhosis [12].
Genetic factors (HLA antigens)
In a study conducted by Morse and co-workers, it was found that in ten racially mixed HIV-infected patients with HIV-associated pulmonary hypertension, there was a significant increase in the frequency of human leukocyte antigen (HLA) class II DR52 and DR6, and of the linked alleles HLA-DRB1-1301/2, -DRB3-0301, -DQB1 0603/4, compared to the frequencies of the same alleles in normal Caucasian control subjects [16]. HLA-DR6 and its DRB1-1301/2 subtypes were also significantly increased in HIV-associated pulmonary hypertension patients compared to the respective frequencies of racially diverse HIV-positive control subjects. Furthermore, HLA-DR6 and the DRB1-1301 subtype have also been reported to increase in HIV-positive patients who develop diffuse infiltrative lymphocytosis syndrome [17, 18]. It is possible that both entities represent different spectra of a common HLA-DR-determined host response to HIV-1.
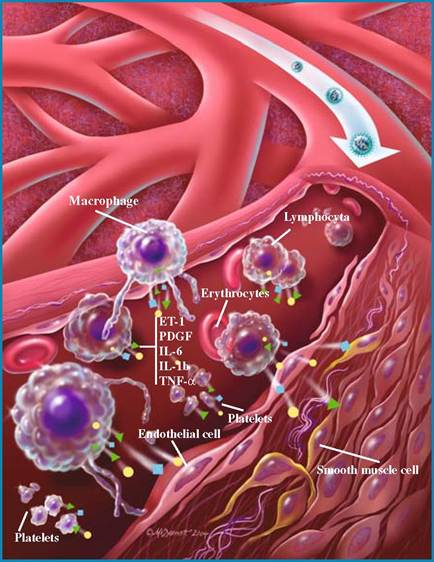
Fig. 2 The possible pathogenetic mechanisms involved in the development of HIV-associated pulmonary hypertension. HIV-infected macrophages, platelets, and lymphocytes may release multifunctional cytokines-endothelin-1 (ET-1), platelet-derived growth factor (PDGF), interleukin-6 (IL-6), interleukin-1 beta (IL-1b), tumor necrosis factor alfa (TNF-α)-which may affect the endothelial cells of the pulmonary vessels, inducing their proliferation and vasoconstriction by a reduction of nitric oxide (NO) production.
Moreover, ET-1 produced by endothelial cells may affect the smooth muscle cells of the pulmonary vessels inducing their migration and proliferation. (From [20], with permission from Teri McDermott. ©2004 Teri McDermott CMI)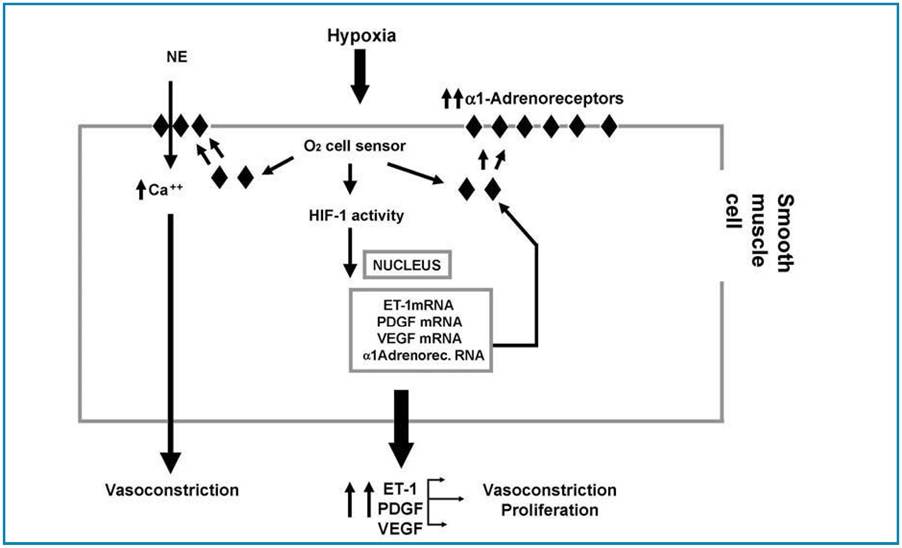
Fig. 3 Chronic stimulation of α1-adrenoreceptors of the pulmonary vasculature can induce the local production of a large amount of cytokines and particularly of ET-1, IL-1b, IL-6, and PDGF, which in turn stimulate the growth of new pulmonary capillaries, induce vasoconstriction of resistance-sized pulmonary arteries, and have an anti-apoptosis effect. (From [21], with permission from Wiley-Blackwell)
the patients were male, and the age at the time of diagnosis ranged from 2 to 56 years (mean 33 years). Intravenous drug use was the most common risk factor and ranged from 50 to 58%, while homosexual behavior was present in 20% of the patients, hemophilia in 9%, heterosexual contacts in 9%, and other risk factors in 6% of the patients [2, 11, 12], reflecting the epidemiology of HIV infection in the general population. The mean CD4+ count was 300 mm3 (range 0-937/mm3). Currently, no correlation has been found between the CD4+ count and the presence of opportunistic infections and the development of pulmonary hypertension.
The most common presenting symptom was dyspnea (from 49 to 85%), while pedal edema ranged from 11 to 30% of the patients, nonproductive cough from 7 to 19%, syncope from 8 to 12%, and chest pain was present in 7% of the patients. Raynaud’s syndrome, which is more frequently found in patients affected by pulmonary hypertension associated to connective tissue disease, was present in only one patient (1%) [2,12].
Signs of pulmonary hypertension on physical examination are subtle and often overlooked. An accentuated pulmonary component of the second heart sound, audible at the apex, may be noted in more than 90% of patients, reflecting an increased force of pulmonary valve closure due to elevated pulmonary artery pressure [19]. Other signs of increased pulmonary artery pressure may include the following [19]:
a.
An early systolic ejection click due to sudden interruption of pulmonary valve openingb. A midsystolic ejection murmur caused by turbulent transvalvular pulmonary flow
c. A palpable left parasternal lift produced by the impulse of the hypertrophied high-pressure right ventricle
d. A right ventricular S4 gallop
e. A prominent jugular “a” wave suggesting high right ventricular filling pressure Physical signs of more advanced disease
include the diastolic murmur of pulmonary regurgitation and the holosystolic murmur of tricuspid valve regurgitation, which is audible at the lower left sternal border and augmented with inspiration. A right ventricular S3 gallop, marked distension of the jugular veins, pulsatile hep atomegaly, peripheral edema, and ascites are indicative of right ventricular failure [19]. The principal diagnostic tests used for diagnosis of HIV-associated pulmonary hypertension with related clinical verification are reported in Table 2.
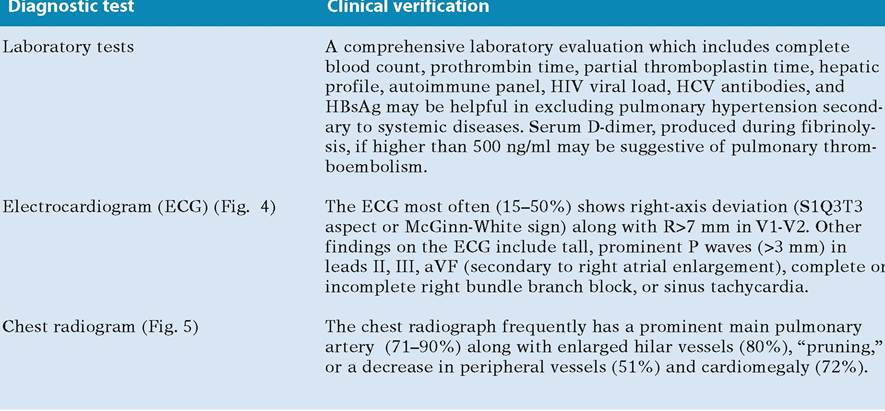
Table 2 Principal diagnostic tests for diagnosis of HIV-associated pulmonary hypertension
cont. →
Table 2 cont.
| Diagnostic test | Clinical verification |
| Transthoracic echocardiography (TTE) (Figs. 6-9) | The most frequent findings on TTE are: systolic flattening of the interventricular septum, right atrial and right ventricular enlargement, and tricuspid regurgitation. Additionally, TTE can estimate pulmonary arterial systolic pressure by measuring the Doppler flow through the tricuspid valve according to the modified Bernulli formula: P=4V2 (where P is pressure gradient and V is peak retrograde velocity). The right atrial pressure is nominally estimated at 10 mmHg. The grade of pulmonary hypertension is categorized as grade I (36-45 mmHg), grade II (46-55 mmHg), and grade III (> 56 mmHg). Finally, the TTE can evaluate secondary causes of pulmonary hypertension such as congenital heart disease or valvular disease. |
| Pulmonary function tests (PFTs) | The most frequent abnormality seen on PFTs in patients with pulmonary and arterial blood gases (ABG) hypertension is a decrease in the diffusing capacity for carbon monoxide (DLco; mean, 69% of predicted). A mild restrictive pattern (mild decrease in total lung capacity) may also be seen. ABG are frequently obtained along with the PFTs and most commonly demonstrate hypoxemia and a respiratory alkalosis (hypocapnea). |
| Ventilation-perfusion (V/Q) scan | An abnormal V/Q scan should not necessarily be interpreted as evidence of thromboembolic disease; patients with non-thromboembol- ic pulmonary hypertension often have abnormal V/Q scans, most commonly displaying a diffuse patchy pattern. In HIV-associated pulmonary hypertension the most common findings observed in V/Q scans is a patchy distribution of the tracer or normal lung scan. |
| Spiral computerized tomography (CT) | It is a fast, safe, minimally invasive procedure which shows the thrombus in segmental and subsegmental arteries and gives further information suggesting or confirming alternative clinical diagnoses frequently observed in HIV-infected patients (pneumonia, pulmonary fibrosis, cardiovascular diseases, pulmonary neoplasms, pleural diseases). |
| Pulmonary angiography and right heart cardiac catheterization (Fig. 10) | Pulmonary angiography is restricted to cases with unclear or negative spiral CT scans but with a strong clinical suspicion of pulmonary hypertension. Right heart cardiac catheterization is the standard for diagnosis and measurement of hemodynamic values. |
Table 3 Treatment of HIV-associated pulmonary hypertension
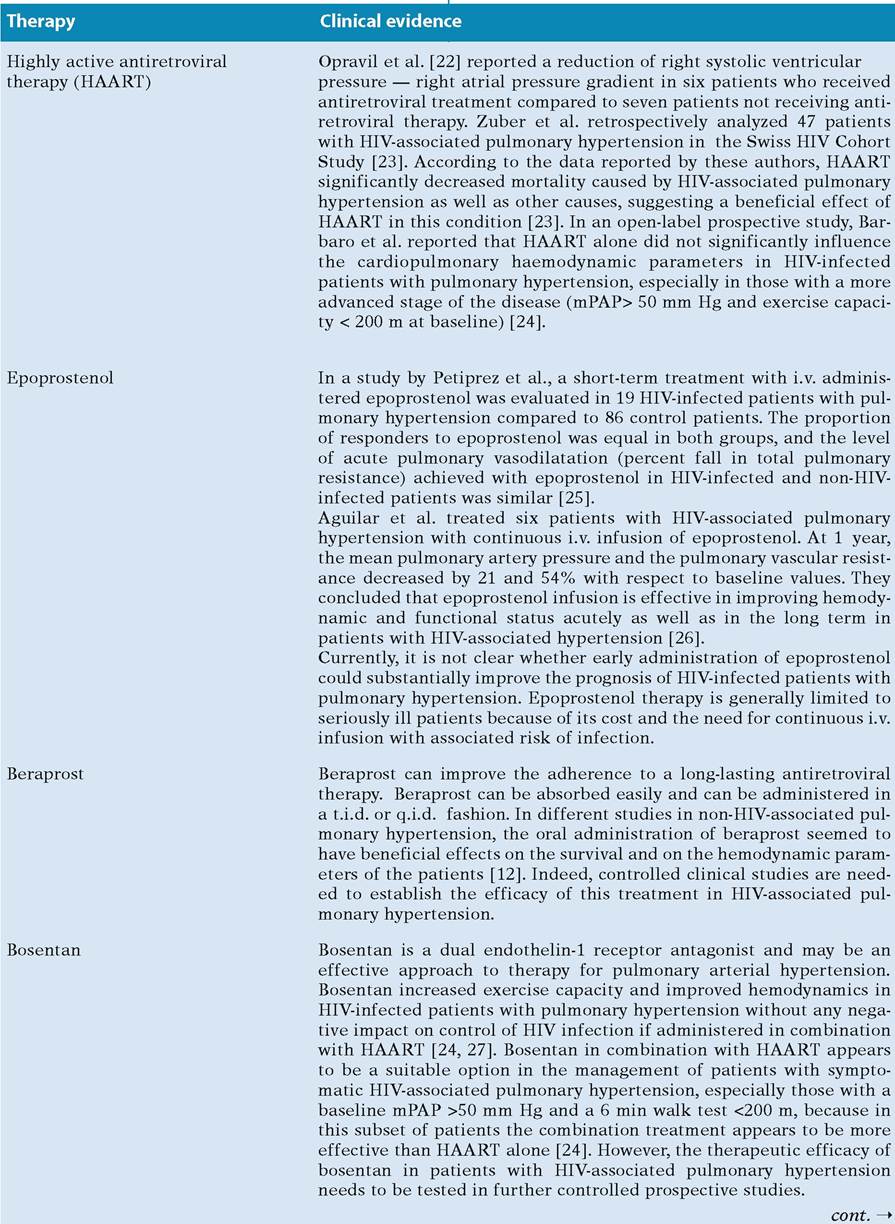
Table 3 cont.
| Therapy | Clinical evidence |
| Calcium channel blockers | Treatment with calcium channel blockers seems to be another alternative in the therapy of HIV-associated pulmonary hypertension. However, reports regarding a small sample of patients with HIV-associated pulmonary hypertension treated with this kind of therapy have shown contrasting response rates [12]. Moreover, calcium channel blockers should be used with caution in patients receiving HAART, since they interact with protease inhibitors. |
| Sildenafil | Oral sildenafil seems to be beneficial as a selective pulmonary vasodilator in patients with primary pulmonary hypertension. Sildenafil may preferentially inhibit cGMP-specific phosphodiesterase, which is abundant in lung tissue [12, 25]. Therefore, the possibility of treatment needs to be evaluated prospectively in patients with HIV- associated pulmonary hypertension. |
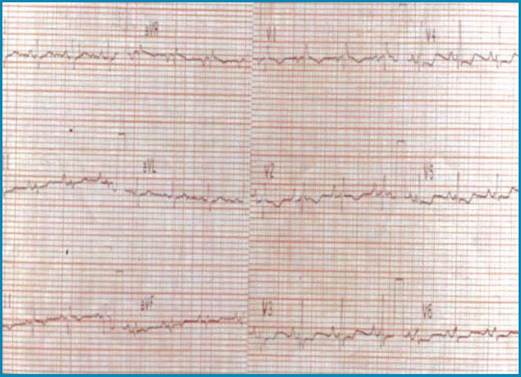
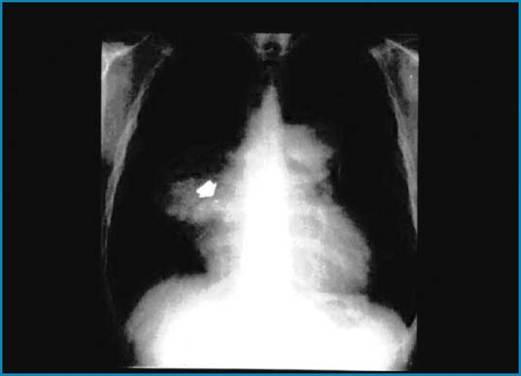
Fig. 4 ECG recording in a patient with HIV-associated pulmonary hypertension. A right-axis deviation (S1Q3T3 aspect or McGinn-White sign) along with tall, prominent P waves in leads II, III, aVF (secondary to right atrial enlargement) and complete right bundle branch block is evident
Fig. 5 Chest radiogram in a patient with HIV-associated pulmonary hypertension. A prominent main pulmonary artery along with enlarged hilar vessels (arrow) accompanied by a decrease in peripheral vessels and cardiomegaly is evident. (From [28], with permission from Wiley- Blackwell)
More on the topic Clinical Manifestations and Diagnosis of HIV-Associated Pulmonary Hypertension:
- The Purpose of a Diagnosis
- Barbaro Giuseppe, Boccara Franc (eds.). Cardiovascular Disease in AIDS. 2nd edition. — Springer,2009. — 169 p., 2009
- Chemically hazardous substances, ecotoxicology