Coagulative Disorders in HIV-Infected Patients Leading to Hemorrhagic Condition
Thrombocytopenia
The most frequent hemorrhagic condition associated with HIV infection is thrombocytopenia [57]. Although often asymptomatic, thrombocytopenia may be linked to a variety of bleeding abnormalities.
The underlying pathophysiology includes accelerated peripheral platelet destruction and decreased (“ineffective”) production of platelets from the infected megakaryocytes. In drug users, the disease appears to be of more rapid progression and more frequently complicated. HIV-associated thrombocytopenia responds to antiretroviral therapy, but this is less effective in drug users [58]. Some studies have evaluated the use of zidovudine (AZT) and have shown increased platelet production. HAART induces a sustained platelet response in HIV-associated thrombocytopenia, even in antiretroviral- experienced subjects and in those with AZT-resistant thrombocytopenia (Table 2) [59]. If antiretroviral agents fail to improve the platelet count or if antiretroviral agents cannot be used, other treatments, similar to those used in “classic” immune thrombocytopenia (ITP), can be employed, including steroids and intravenous immunoglobulins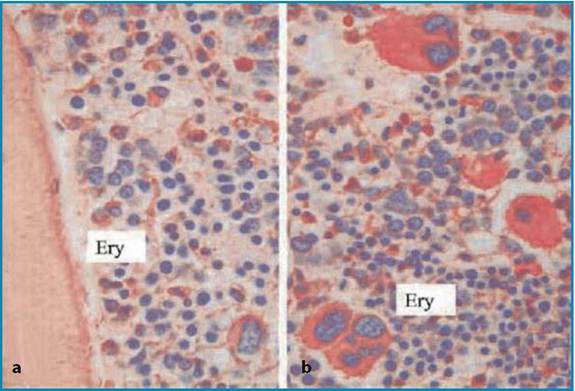
Fig.4a,b Photomicrographs of bone marrow core biopsy. a Paratrabec- ular aggregates of erythroid precursor cells as seen in myelodysplasia. H&E, ? 400. b Hypercellu- larity with erythroid and megakaryocytes hyperplasia. PAS, ? 400. (From [56], with permission of Wiley-Liss, Inc., a subsidiary of John Wiley & Sons, Inc.)
(intravenous anti-D). Splenectomy has been used to treat HIV-infected patients with refractory thrombocytopenia. Although it is an effective treatment, there are concerns about infections and selection of appropriate candidates. Other treatment modalities, such as interferon, vincristine, danazol, low- dose splenic irradiation, and staphylococcal protein A immunoadsorption have shown limited success in HIV-associated thrombocytopenia.
Alternatively, thrombocytopenia in HIV-infected patients may be treated with pharmacological hyperstimulation of megakaryocytopoiesis (administration of PEG-rHuMGDF or TPO). The latest evidence indicates that the chemokine receptor CXCR4 (co-receptor for the cellular entry of lymphotropic HIV strains) is expressed on megakaryocytes; as a result, the development of chemokine receptor antagonists may modify the course of the disease.Table 2 Platelet and CD4+ response to antiretroviral therapy in 34 HIV-infected patients with severe thrombocytopenia. (From [59], with permission from the British Infection Society)
| Variable | No. of patients | Baselinea | Treatr 3rd montl | ent h | a 6th ronth | Overallb c2 | p | 0 -3rd ronthc p | 3rd-6th ronthc p |
| HAART treatment | 15 | ||||||||
| PLT count (PLT x 10 9 /1) | 32 | 87 | 108 | 10.53 | 0.01 | 0.01 | NS | ||
| (6 -49) | (34 - | 259) | (20 -195) | ||||||
| CD4+(cells∕μl) | 58 | 127 | 142 | 8.1 | 0.02 | 0.05 | NS | ||
| (1 -392) | (10 - | 503) | (4 -387) | ||||||
| AZT treatment | 19 | ||||||||
| PLT count (PLT x 10 9 /1) | 29 | 49 | 79 | 20.63 | 0.001 | 0.01 | NS | ||
| (6 -47) | (12 - | 429) | (9 -253) | ||||||
| CD4+(cells∕μl) | 96 | 144 | 99 | 6.63 | 0.03 | 0.01 | NS | ||
| (9 -177) | (16 - | 528) | (15 -378) |
aValues of each variable are median (range); bFriedmann test; cWilcoxon-Wilcox test
Increased Hemorrhagic Tendency and Hemophiliac HIV Patients
One concerning side effect of HAART is the increased hemorrhagic tendency of hemophiliac patients contaminated and treated for HIV.
Shortly after the introduction of PIs for the treatment of HIV infection, an association between these drugs and an increased bleeding tendency in patients with hereditary bleeding disorders was observed. The patients experience not only an increased bleeding frequency in usual sites, but bleeding can also occur in unusual sites such as the finger joints. Mucus membrane bleeding and hematuria are also common. Ritonavir appears to be associated with the highest risk of bleeding followed by indinavir. PI-associated bleeds tend to be more resistant to factor VIII concentrate treatment, and periods of prophylaxis may be required in individuals with frequent persistent bleeding. Patients continuing PI therapy tend to develop a tolerance to this adverse effect over time. The mechanism of the bleeding tendency has not been elucidated. There is no consistent evidence of a disturbance of coagulation, fibrinolysis, or platelet function, which raises the possibility that PIs may exert a direct local effect on blood vessels. It is very important that this class-specific side effect is recognized and understood by both the physicians and the patients [52].References
1. Koppel K, Bratt G, Schulman S, Bylund H, Sandstrom E (2002) Hypofibrinolytic state in HIV-1- infected patients treated with protease inhibitor-containing highly active antiretroviral therapy. J Acquir Immune Defic Syndr 29:441-449
2. Hadigan C, Meigs JB, Rabe J et al (2001) Increased PAI-1 and tPA antigen levels are reduced with metformin therapy in HIV-infected patients with fat redistribution and insulin
resistance. J Clin Endocrinol Metab 86:939-943
3. Yki-Jarvinen H, Sutinen J, Silveira A et al (2003) Regulation of plasma PAI-1 concentrations in HAART-associated lipodystrophy during rosiglitazone therapy. Arterioscler Thromb Vasc Biol 23:688-694
4. Drouet L, Scrobohaci ML, Janier M, Baudin B (1990) Endothelial cells: target for the HIV1 virus? Nouv Rev Fr Hematol 32:103-106
5. Aukrust P, Bjornsen S, Lunden B et al (2000) Persistently elevated levels of von Willebrand factor antigen in HIV infection.
Downregulation during highly active antiretroviral therapy. Thromb Haemost 84:183-1876. Wolf K, Tsakiris DA, Weber R, Erb P, Battegay M (2002) Antiretroviral therapy reduces markers of endothelial and coagulation activation in patients infected with human immunodeficiency virus type 1. J Infect Dis 185:456-462
7. Miguez-Burbano MJ, Burbano X, Rodriguez A, Lecusay R, Rodriguez N, Shor-Posner G (2002) Development of thrombocytosis in HIV+ drug users: impact of antiretroviral therapy. Platelets 13:183-185
8. Saif MW, Greenberg B (2001) HIV and thrombosis: a review. AIDS Patient Care STDS 15:15-24
9. Sullivan PS, Dworkin MS, Jones JL, Hooper WC (2000) Epidemiology of thrombosis in HIV- infected individuals: The Adult/Adolescent Spectrum of HIV Disease Project. AIDS 14:321-324
10. Majluf-Cruz A, Silva-Estrada M, Sanchez-Barboza R et al (2004) Venous thrombosis among patients with AIDS. Clin Appl Thromb Hemost 10:19-25
11. Callens S, Florence E, Philippe M, Van Der PM, Colebunders R (2003) Mixed arterial and venous thromboembolism in a person with HIV infection. Scand J Infect Dis 35:907-908
12. Becker DM, Saunders TJ, Wispelwey B, Schain DC (1992) Case report: venous thromboembolism in AIDS. Am J Med Sci 303:395-397
13. Tanimowo M (1996) Deep vein thrombosis as a manifestation of the acquired immunodeficiency syndrome? A case report. Cent Afr J Med 42:327-328
14. Vielhauer V, Schewe CK, Schlondorff D (1998) Bilateral thrombosis of the internal jugular veins with spasmodic torticollis in a patient with acquired immunodeficiency syndrome and disseminated cytomegalovirus infection. J Infect 37:90-91
15. Bayer DD, Sorbello AF, Condoluci DV (1995) Bilateral subclavian vein thrombosis in a patient with acquired immunodeficiency syndrome. J Am Osteopath Assoc 95:276-277
16. Laing RB, Brettle RP, Leen CL (1996) Venous thrombosis in HIV infection. Int J STD AIDS 7:82-85
17. Meyohas MC, Roullet E, Rouzioux C et al (1989) Cerebral venous thrombosis and dual primary infection with human immunodeficiency virus and cytomegalovirus.
J Neurol Neurosurg Psychiatry 52:1010-101118. Carr A, Brown D, Cooper DA (1997) Portal vein thrombosis in patients receiving indinavir, an HIV protease inhibitor. AIDS 11:1657-1658
19. Narayanan TS, Narawane NM, Phadke AY, Abraham P (1998) Multiple abdominal venous thrombosis in HIV-seropositive patients. Indian J Gastroenterol 17:105-106
20. Roberts SP, Haefs TM (1992) Central retinal vein occlusion in a middle-aged adult with HIV infection. Optom Vis Sci 69:567-569
21. Mansour AM, Li H, Segal EI (1996) Picture resembling hemicentral retinal vein occlusion in the acquired immunodeficiency syndrome: is it related to cytomegalovirus? Ophthalmologica 210:108-111
22. Park KL, Marx JL, Lopez PF, Rao NA (1997) Noninfectious branch retinal vein occlusion in HIV-positive patients. Retina 17:162-164
23. Stahl CP, Wideman CS, Spira TJ, Haff EC, Hixon GJ, Evatt BL (1993) Protein S deficiency in men with long-term human immunodeficiency virus infection. Blood 81:1801-1807
24. Bissuel F, Berruyer M, Causse X, Dechavanne M, Trepo C (1992) Acquired protein S deficiency: correlation with advanced disease in HIV-1- infected patients. J Acquir Immune Defic Syndr 5:484-489
25. Toulon P, Lamine M, Ledjev I et al (1993) Heparin cofactor II deficiency in patients infected with the human immunodeficiency virus. Thromb Haemost 70:730-735
26. Muller MM, Griesmacher A (2000) Markers of endothelial dysfunction. Clin Chem Lab Med 38:77-85
27. Gujuluva C, Burns AR, Pushkarsky T et al (2001) HIV-1 penetrates coronary artery endothelial cells by transcytosis. Mol Med 7:169-176
28. Madalosso C, de SN Jr, Ilstrup DM et al (1998) Cytomegalovirus and its association with hepatic artery thrombosis after liver transplantation. Transplantation 66:294-297
29. Kaukoranta-Tolvanen SS, Ronni T, Leinonen M et al (1996) Expression of adhesion molecules on endothelial cells stimulated by Chlamydia pneumoniae. Microb Pathog 21:407-411
30. Zhong DS, Lu XH, Conklin BS et al (2002) HIV protease inhibitor ritonavir induces cytotoxicity of human endothelial cells.
Arterioscler Thromb Vasc Biol 22:1560-156631. Stimmler MM, Quismorio FP Jr, McGehee WG et al (1989) Anticardiolipin antibodies in acquired immunodeficiency syndrome. Arch Intern Med 149:1833-1835
32. Karmochkine M, Raguin G (1998) Severe coronary artery disease in a young HIV-infected man with no cardiovascular risk factor who was treated with indinavir. AIDS 12:2499
33. Ankri A, Bonmarchand M, Coutellier A, Herson S, Karmochkine M (1999) Antiphospholipid antibodies are an epiphenomenon in HIV-infected patients. AIDS 13:1282-1283
34. Feffer SE, Fox RL, Orsen MM et al (1995) Thrombotic tendencies and correlation with clinical status in patients infected with HIV. South Med J 88:1126-1130
35. Force L, Barrufet P, Herreras Z, Bolibar I (1999) Deep venous thrombosis and megestrol in patients with HIV infection. AIDS 13:1425-1426
36. Hirsh J, Hull RD, Raskob GE (1986) Epidemiology and pathogenesis of venous thrombosis. J Am Coll Cardiol 8(6 Suppl B):104B-113B
37. Kaufmann T, Nisce LZ, Metroka C (1991) Thromboembolism in AIDS-related Kaposi’s sarcoma. JAMA 266:2834
38. Heit JA (2002) Venous thromboembolism epidemiology: implications for prevention and management. Semin Thromb Hemost 28(Suppl 2):3-13
39. Biswas J, Roy CB, Krishna KS et al (2001) Detection of Mycobacterium tuberculosis by polymerase chain reaction in a case of orbital tuberculosis. Orbit 20:69-74
40. Friedman SM, Margo CE (1995) Bilateral central retinal vein occlusions in a patient with acquired immunodeficiency syndrome. Clinico- pathologic correlation. Arch Ophthalmol 113:1184-1188
41. Iranzo A, Domingo P, Cadafalch J, Sambeat MA (1998) Intracranial venous and dural sinus thrombosis due to protein S deficiency in a patient with AIDS. J Neurol Neurosurg Psychiatry 64:688
42. Biswas J, Kumar AA, George AE et al (2000) Ocular and systemic lesions in children with HIV. Indian J Pediatr 67:721-724
43. Kleinschmidt-DeMasters BK, Mazowiecki M, Bonds LA et al (2000) Coccidioidomycosis meningitis with massive dural and cerebral venous thrombosis and tissue arthroconidia. Arch Pathol Lab Med 124:310-314
44. Doberson MJ, Kleinschmidt-DeMasters BK (1994) Superior sagittal sinus thrombosis in a patient with acquired immunodeficiency syndrome. Arch Pathol Lab Med 118:844-846
45. Abuaf N, Laperche S, Rajoely B et al (1997) Autoantibodies to phospholipids and to the coagulation proteins in AIDS. Thromb Haemost 77:856-861
46. Shahnaz S, Parikh G, Opran A (2004) Antiphospholipid antibody syndrome manifesting as a deep venous thrombosis and pulmonary embolism in a patient with HIV. Am J Med Sci 327:231-232
47. Ramos-Casals M, Cervera R, Lagrutta M et al (2004) Clinical features related to antiphospholipid syndrome in patients with chronic viral infections (hepatitis C virus/HIV infection): description of 82 cases. Clin Infect Dis 38:1009-1016
48. Sugerman RW, Church JA, Goldsmith JC, Ens GE (1996) Acquired protein S deficiency in children infected with human immunodeficiency virus. Pediatr Infect Dis J 15:106-111
49. Melchior JC, Messing B (1999) Home parenteral nutrition in acquired immunodeficiency syndrome patients. Nutrition 15:68-69
50. Duerksen DR, Ahmad A, Doweiko J et al (1996) Risk of symptomatic central venous thrombotic complications in AIDS patients receiving home parenteral nutrition. JPEN J Parenter Enteral Nutr 20:302-305
51. George SL, Swindells S, Knudson R, Stapleton JT (1999) Unexplained thrombosis in HIV- infected patients receiving protease inhibitors: report of seven cases. Am J Med 107:624-630
52. Wilde JT, Lee CA, Collins P et al (1999) Increased bleeding associated with protease inhibitor therapy in HIV-positive patients with
bleeding disorders. Br J Haematol 107:556-559
53. Llibre JM, Romeu J, Lopez E, Sirera G (2002) Severe interaction between ritonavir and acenocoumarol. Ann Pharmacother 36:621-623
54. Rerolle JP, Canaud G, Fakhouri F et al (2004) Thrombotic microangiopathy and hypothermia in an HIV-positive patient: importance of cytomegalovirus infection. Scand J Infect Dis 36:234-237
55. Gervasoni C, Ridolfo AL, Vaccarezza M et al (2002) Thrombotic microangiopathy in patients with acquired immunodeficiency syndrome before and during the era of introduction of highly active antiretroviral therapy. Clin Infect Dis 35:1534-1540
56. Gruszecki AC, Wehrli G, Ragland BD et al (2002) Management of a patient with HIV infection- induced anemia and thrombocytopenia who presented with thrombotic thrombocytopenic purpura. Am J Hematol 69:228-231
57. Scaradavou A (2002) HIV-related thrombocytopenia. Blood Rev 16:73-76
58. Burbano X, Miguez MJ, Lecusay R et al (2001) Thrombocytopenia in HIV-infected drug users in the HAART era. Platelets 12:456-461
59. Carbonara S, Fiorentino G, Serio G et al (2001) Response of severe HIV-associated thrombocytopenia to highly active antiretroviral therapy including protease inhibitors. J Infect 42:251-256
More on the topic Coagulative Disorders in HIV-Infected Patients Leading to Hemorrhagic Condition:
- Coagulative disorders in human immunodeficiency virus (HIV)-infected patients can lead to two opposite conditions:
- Coagulative Disorders in HIV-Infected Patients Leading to Thrombotic Conditions
- In patients infected with HIV, the whole neuraxis is vulnerable to damage. Up to 10% of patients may present with a neurological disorder at seroconversion (Box 8.1).
- CASE 20: Leading a Bride into the Home
- Barbaro Giuseppe, Boccara Franc (eds.). Cardiovascular Disease in AIDS. 2nd edition. — Springer,2009. — 169 p., 2009
- The sixth leading jurisprudent: Sufyan b. Said al-Thawri al-Kufi (162/778)
- 2 The Agriculture Condition
- Humanity and the Human Condition
- In mental life nothing which had once been formed can perish - that everything is somehow preserved and that in suitable circumstances... it can once more be brought to light... on condition that the organ of the mind has remained intact and that its tissues have not been damaged by trauma or inflammation.
- 8 The Occupancy Condition