Description and Pathophysiology of the ART-Related Metabolic Alterations
Dyslipidemia
Increased levels of TG and cholesterol, together with decreased HDL and increased LDL cholesterol, have been described in HIV patients undergoing ART [31]. These alterations probably have multiple origins.
The HIV infection itself has been shown to be associated with increased levels of TG, decreased levels of HDL and, in patients with AIDS, of LDL cholesterol. These alterations could result from the high level of proinflam- matory cytokines (TNF-α, IL-6, IL-1) observed in these patients with an active infection, due to their increased secretion by activated monocytes and macrophages. TNF-α and IL-6 can decrease the expression and activity of lipoprotein lipase, which is involved in TG clearance from circulation lipoproteins. Moreover, acute-phase proteins can bind to HDL particles, promoting their uptake by macrophages and therefore increasing their clearance rate. These phenomena are seen in infection with severe inflammation whatever its origin [32].After the introduction of HAART, increased levels of lipids were constantly reported [31, 33]. Regarding the NRTIs, stavudine was associated with increased levels of TG [34]. However, the major contributor to dyslipidemia was the class of PIs. Studies performed in non-HIV-infected control subjects revealed that RTV was able, after a few days, to alter lipid parameters with hyper-TG and increased cholesterol levels. Similarly, boosting concentrations of RTV in association with LPV increased TG levels. By contrast, atazanavir was associated with a safe metabolic profile [35]. NNR- TIs are also able to modify lipid parameters: NVP increases total and HDL cholesterol levels but not TG [36]. EFV has a similar effect but increases cholesterol and TG. Various phenotypes of dyslipidemia were reported in patients undergoing ART with PIs, but the major alterations are increased levels of TG, decreased levels of HDL, and increased content in small dense LDLs, a profile very similar to that seen in the classic metabolic syndrome.
An important prevalence of lipid alterations was observed in PI-treated patients when first generation PI were introduced; in an Australian cohort, 14 months after initiating treatment with PIs, 50% of the patients had TG levels above2 mmol/L and 60% had cholesterol levels above 5.5 mmol/L, whereas these values were 22% and 11%, respectively, in patients under NRTI treatment without PIs [37]. In the French cohort APROCO-TM, after 1 and
3 years of PI treatment, respectively, the prevalence of hyper-TG increased from 26 to 36% in men and from 20 to 25% in women. The prevalence of hypercholesterolemia was elevated between 55 and 60% in both groups [34]. At present, the use of PI with a more friendly metabolic effect such as atazanavir and the more generalized dietary and lipid-lowering drugs prescriptions allowed a reduction of the lipid values in this population [31].
The PI-induced alterations could result from a direct effect of the drugs, particularly at the liver level, resulting in modified lipid metabolism (Fig. 7). The synthesis and secretion of apoB, the major VLDL-linked apoprotein, are partly regulated by the balance between the association to lipids and the degradation in the proteasome system involved in overall cellular protein degradation. Thus, it has been shown, in in vitro models of hepatic cells, that RTV and SQV could inhibit the degradation of apoB by inhibiting the proteasome, which results in increased VLDL secretion [38]. When animals were fed a high-fat diet, an increased synthesis of TG on VLDL was observed [39]. Moreover, RTV is able to increase VLDL secretion in mice through the activation of the lipogenic transcription factor SREBP-1 in the liver [40]. Regarding VLDL catabolism, Bonnet et al. presented interesting data [41] indicating that, in PI-treated patients, there was an accumulation of lipoparticles containing apoC-III and apo-E in association with apoB. These complex particles would represent persistent potentially atherogenic cholesterol-rich remnant particles derived from TG-rich lipoproteins.
The observed excess in apoC-III on lipoproteins might be a major determinant of a slower catabolism of TG-rich lipoproteins, since apoC-III is an inhibitor of lipoprotein lipase activity and it also impairs the interaction of apoB and apoE with the LDL- receptor and LRP. This will result in an increased level of remnant lipoprotein returning to the liver.In addition to a direct effect of some PIs on lipid metabolism, the altered repartition of body fat is probably also involved in lipid alterations. As explained above, for the metabolic syndrome, increased content in visceral fat as well as decreased peripheral adipose tissue are associated with an increased level of lipolysis and of FFA fluxes together with altered adipocytokine production: increased levels of TNF-α, IL-1, and IL-6 and decreased levels of adiponectin [42, 43]. Thus, even after the introduction of HAART, the severity of the inflammatory syndrome is markedly decreased as compared to the state of active infection. Patients with ART-related metabolic syndrome still present a state of low-grade inflammation with increased cytokines and acute-phase proteins such as CRP, which could contribute to the dyslipidemia observed in these patients.
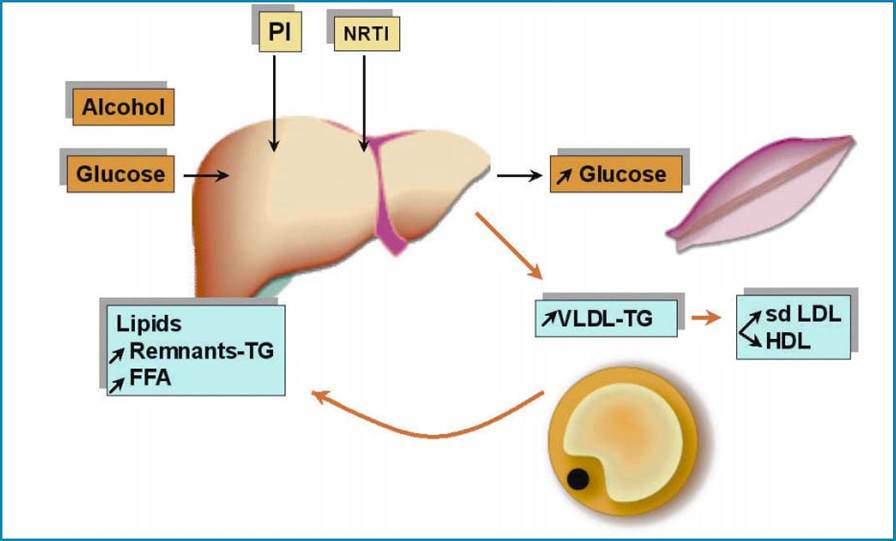
Fig. 7 Adverse effects of antiretroviral treatment on lipid and glucose metabolism. sdLDL, small dense LDL
Altered Glucose Tolerance, Diabetes and Insulin Resistance
The presence of altered glucose tolerance is observed in a minority of PI-treated patients, but its prevalence was high with the first generation PI and in particular with the wide use of indinavir. In the APRO- CO-TM French cohort, increased glycemia (either fasting hyperglycemia or glucose intolerance) increased from 17 to 27% in men after 1 and 3 years of treatment with PI, respectively, while diabetes increased from 4 to 9%. In women, alterations in glucose tolerance remained stable at 25% but the prevalence of diabetes increased from 2 to 11%.
More recent data, 6 years after the introduction of PI in the treatment of these patients, reveal that the incidence of diabetes is increased [44]. In a recent study on the Swiss cohort [45], an increased incidence of diabetes was noted in particular in the oldest patients as compared to the general population and the occurrence of diabetes was estimated at 4.4 cases per 1,000 person-years of follow-up (PYFU) and was strongly associated with the treatment with PI (except atazanavir), stavudine and didanosine. This incidence is much higher in the US population, with a higher BMI since it has been reported to be of 47 cases per 1,000 PYFU [46]. These data suggest that the prevalence and the severity of glucose alterations tend to increase with the duration of the treatment. Insulin resistance, which can be evaluated by the simple HOMA test, was highly prevalent in these patients when indinavir was used and is less frequent at present [31, 47].Studies performed with non-HIV-infected control subjects revealed that IDV was able to induce insulin resistance and to modify glycemia after a few days [48]. After a single dose, IDV was able to decrease glucose uptake during a clamp test, indicating insulin resistance, which was rapid and reversible [49]. It is hypothesized that this effect could be due to inhibition of the insulin-sensitive glucose transporter GLUT4 that has been evidenced in in vitro studies. Similarly, LPV boosted by RTV induced an increased glycemia and insulinemia after 4 weeks in normal volunteers [35].
The prevalence of glucose alterations and insulin resistance has been consistently found to be higher in patients with lipodystrophy than in patients without lipodystrophy. A role for adipose tissue in insulin resistance resulting from altered cytokine production and increased lipolysis can be easily hypothesized, which would accentuate the metabolic disorders. As explained below, lipodystrophic adipose tissue presents an altered profile of secreted cytokines with increased TNF-α and IL-6. These cytokines are responsible for insulin resistance at the adipocyte level resulting in increased lipolysis and FFA fluxes, which in turn induce insulin resistance at the level of the liver and muscles. In addition, lipodys- trophic adipose tissue has a decreased secretion of adiponectin, which could result in decreased lipid oxidation and glucose intake in the muscles, and in decreased lipid oxidation and increased glucose production in the liver as explained above. Therefore, the drug-induced alterations in glucose metabolism and in insulin sensitivity are aggravated by the altered adipose tissue function due to lipodystrophy.