Intervention Criteria
Nutritional and Pharmacological Approach
No universally accepted guidelines exist for the nutritional treatment of lipid metabolism disturbances in HIV patients, but according to NCEP [25, 38], our own studies as well as the studies of others [21, 28, 36, 39-41, 52] of patients with preexisting CHD, we advise dietary intervention when the LDL cholesterol level ranges between 100 mg/dl and 130 mg/dl, adding drug therapy if LDL cholesterol exceeds 130 mg/dl.
Among patients without CHD, but presenting two or more risk factors (Fig. 2), dietary intervention is strongly indicated when the LDL cholesterol is between 130 and 160 mg/dl. Drug therapy must be added when the LDL exceeds 160 mg/dl. With fewer than two risk factors, dietary modifications should be recommended when LDL levels range between 160 and 190 mg/dl. Drug therapy should be considered with LDL levels over 190 mg/dl. For patients with very high TG levels (>400 mg/dl), the AACTG [39] suggests a dietary intervention when total cholesterol is higher than 240 mg/dl or HDL cholesterol is lower than 35 mg/dl. Patients with isolated hypertriglyceridemia (fasting serum levels >200 mg/dl) should follow an adequate diet and physical exercise program. If levels exceed 1,000 mg/dl, pharmacological therapy should be strongly suggested because of the risk of pancreatitis. The same indication is mandatory for patients with a history of pancreatitis having TG levels over 500 mg/dl.
To reduce hypercholesterolemia, dietary and exercise treatments are recommended before pharmacological intervention. In patients suffering from wasting and lipid disturbances, it seems preferable to treat the wasting first [36, 53, 54].
For each patient, the guidelines for nutritional intervention must consider RMR, gut functions, concomitant diseases, hormonal status, appetite, and social conditions, as previously described [28, 39, 41].
At the first sign of malnutrition, suitable nutritional treatment is advised [36] because of the positive effect on the infection and on the quality of life. A balanced supply of n-6 and n-3 polyunsaturated fatty acids (PUFA) including eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA; the main components of fish oil) may modulate cytokine production. EPA, as a direct suppressant of lipid mobilization factor, counteracts weight loss, lipolysis, and protein catabolism [55]. Amino acids (1.5-2 g/kg per day) must be administered to block protein loss. A quota of them (training, isometric (static) training, and isokinetic training.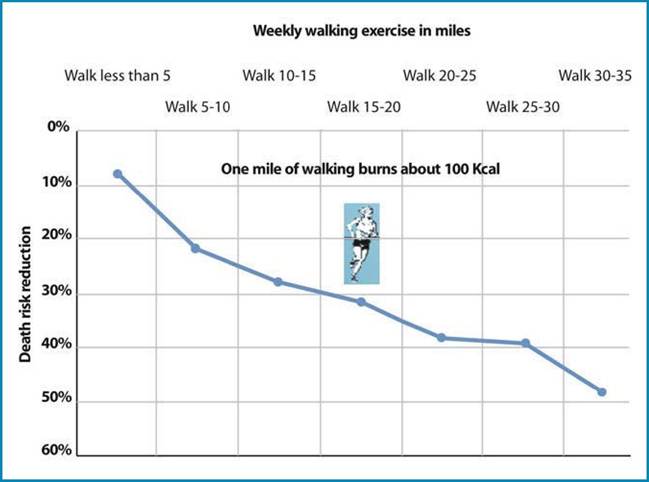
Fig. 4 Regularly walking/ jogging more than 3 miles a day proportionally reduces the risk of death. No additional benefits are obtained with energy expenditure beyond 3,500 kcal per week
Table 1 Beneficial effects of muscular exercise
Increases
> Resistance to fatigue
> Elasticity and flexibility
> Muscular mass and strength
> Respiratory capacity
> Appetite
> Intestinal functions
Decreases
< Stress and insomnia
The neck, arms, and shoulders; the chest, abdomen, and back; and the buttocks and legs can be conditioned separately by specific exercises. All our exercise programs include progressive resistance training of the major muscle groups, according to the studies and indications of many authorities in the field of physical activity in health and disease[19, 42-44, 76, 78-84].
HDL levels may be favorably increased in sedentary people who engage in aerobic training. Concurrently, the LDL levels are lowered so that the net result is a considerably improved ratio of HDL to LDL or HDL to total cholesterol. This exercise effect appears to be independent of whether or not the diet is low in fat or whether or not the exerciser is overweight. The effect of regular endurance-type exercise on the blood lipid profile is certainly a strong argument for incorporating vigorous physical activity into a total program of health maintenance in HIV patients receiving HAART.
It is well known that exercise improves myocardial circulation and metabolism and enhances vascularization, cardiac glycogen stores, and glycolitic capacity, which protects the heart from hypoxic stress [42, 75]. Mechanical and contractile properties of the myocardium are improved, enabling the conditioned heart to maintain or increase contractility during a specific challenge. Heart rate and blood pressure are favorably reduced so the work of the myocardium is significantly reduced at rest and during exercise.Exercise reduces the symptoms and medication doses needed and it corrects the nutritional imbalances and side effects of drugs and altered diet. Many clinical signs and symptoms are responsive to exercise: atrophy of muscle and bone, postural hypotension, joint stiffness, reflexes, cardiovascular deconditioning, anorexia, gastrointestinal motility, insomnia, and depression. Exercise is the way to stimulate the muscles not only to move the body better but also to increase biochemical reactions devoted to energy production. The predominant energy pathways required in physical activities are the ATP-CP system, the lactic acid system, and the oxygen or aerobic system that are often operative simultaneously (Fig. 5). However, their relative contributions to the total energy requirement during an exercise may differ markedly. This contribution is related directly to the length of time and intensity that a specific activity is performed.
Anaerobic Conditioning (Resistance Training or Dynamic-Anaerobic Strength Exercise)
During intense, maximal bursts of energy lasting no more than 6 s, the energy is provided anaerobically almost exclusively by the stored high-energy molecules of phos-
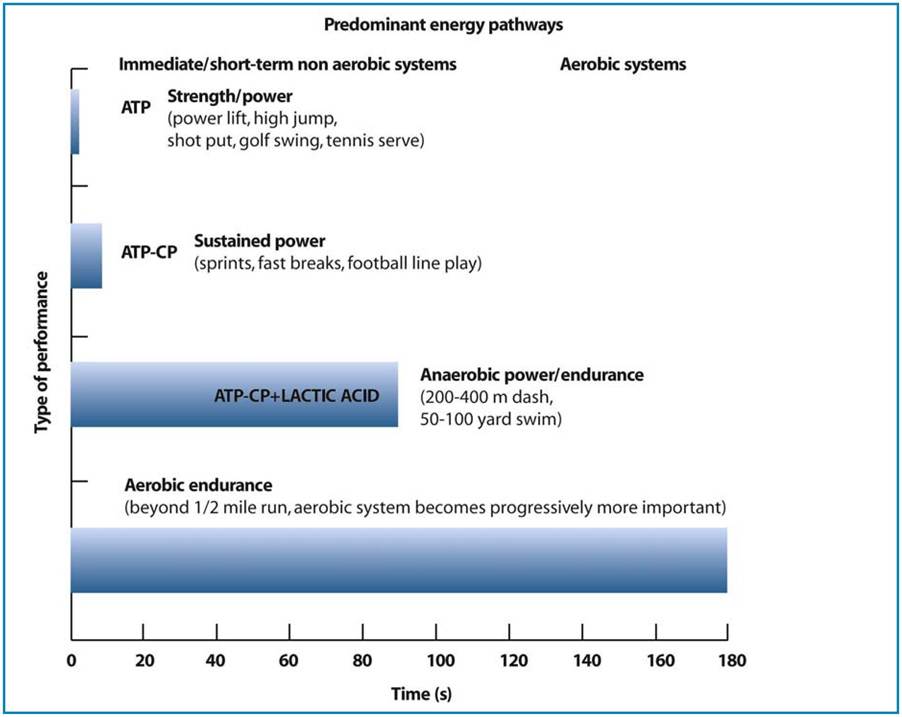
Fig. 5 The three energy systems (ATP-CP system, lactic acid system, aerobic system) are involved in some physical activities. In exercises with an intense, short burst of energy, the energy is provided anaerobically almost exclusively by the stored reserve of ATP and CP.
In performances lasting between 10 and 90 s, the energy from lactic acid production becomes an important source. After 2-4 min of continuous activity, the energy is released almost exclusively from aerobic reactionsphates (ATP and CP). Overload of the ATP- CP pool can be achieved by engaging specific muscles in maximum bursts of effort for 5 or 10 s. In physical activities chosen to enhance the ATP-CP energy capacity of specific muscles, the subject must perform numerous bouts of intense, short-duration exercise. The energy for performances lasting between 10 and 90 s is still supplied predominantly by anaerobic reactions, but lactic acid becomes a more important source of energy. To improve the lactic acid energy system, the training program must be of sufficient intensity and duration to stimulate lactic-acid production as well as to overload the ATP-CP energy system. An effective way to increase near-maximum levels and overload the lactic acid system is repeat bouts of up to 1 min of extreme running, swimming, or cycling, stopped 30-40 s before exhaustion. The exercise bout should be repeated several times after 1-2 min of recovery. Recovery time from the exercise can be considerable when large amounts of lactic acid are produced (Fig. 5).
Aerobic Conditioning (Endurance Exercise or Dynamic-Aerobic Exercise)
After 2-4 min of continuous exercise, any physical activity becomes progressively more dependent on aerobic energy for the resynthesis of the phosphates. Under aerobic conditions, pyruvic acid from carbohydrate metabolism and molecules from fat and protein are transformed into various intermediate substances with the final formation of CO2, H2O, and large amounts of energy. If the O2 supply and utilization are adequate, lactic acid does not accumulate and fatigue is absent. We can reach a condition of endurance or aerobic fitness in which the body’s ability to generate ATP aerobically exceeds the energy produced from anaerobic reactions.
To have a practical measure of cardiovascular capacity of the subject, we use the step-up test (Fig. 6), which provides the heart-rate response to aerobic exercise: a low heart rate during exercise and a small increment with more intense exercise reflect a high level of cardiovascular fitness. A simple method to recover heart rates for evaluation of relative fitness for aerobic exercise is the Tecumseh step test [72].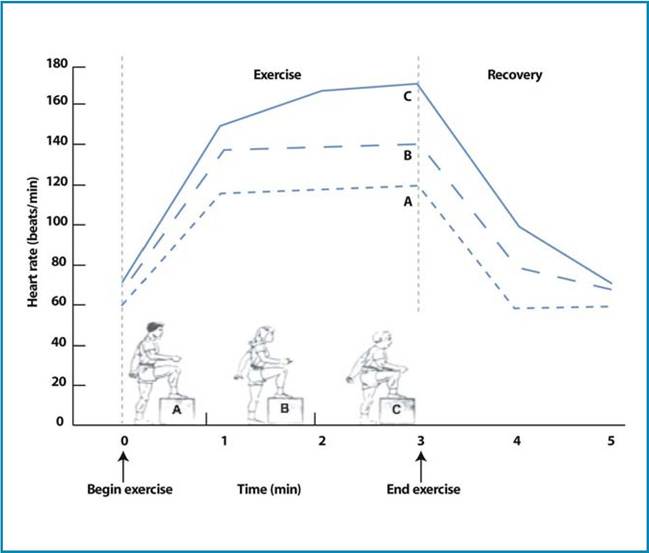
Fig. 6 Step-up exercise to evaluate the cardiovascular capacity: the different heart-rate responses of three individuals during 3 min of regular stepping. The subjects are basically conditioned differently: a professional football player, A, at the end of 3 min reaches a heart rate of 115 beats per minute; for B, a gym-trainer, the heart rate is 140 beats per minute, while C, a sedentary young person, reaches 170 beats per minute. Heart rate recovery is complete 2 min after the end of exercise
In the Tecumseh step test, the stepping cadence must be 22 steps per minute for women and 24 for men, with a stepping height of 20 cm. After 3 min of stepping and exactly 30 s after stopping, the subject must measure the pulse for 30 s in a standing position. The number of pulse beats, from the 30-s to the 1-min post-exercise period, is the heart rate score (Fig. 7). By means of special equations and the recovery heart rate, the maximal O2 consumption can be calculated [73]. Because aerobic capacity declines with age and the population of old HIV infected patients is growing older [29], particular attention must be devoted to prescribe adequate programs of physical activity in this group of patients.
Determination of Frequency, Duration, and Intensity of Training
The intensity of training is the most critical factor that influences successful aerobic conditioning and can be expressed in different ways: as calories consumed, as a percentage of maximal O2 consumption, as heart rate or percentage of maximum heart rate, or as multiples of RMR required to perform the work.
The exercise must be sufficient to produce an increase in heart rate to at least 130-140 beats per minute, equivalent to about 50-55% of the maximum aerobic capacity or about 70% of the maximum exercise heart rate (Fig. 8).121" class="lazyload" data-src="/files/uch_group75/uch_pgroup303/uch_uch7204/image/image116.jpg">
Fig. 7 Pulse rate self-taken at the a temporal, b carotid, and c radial arteries
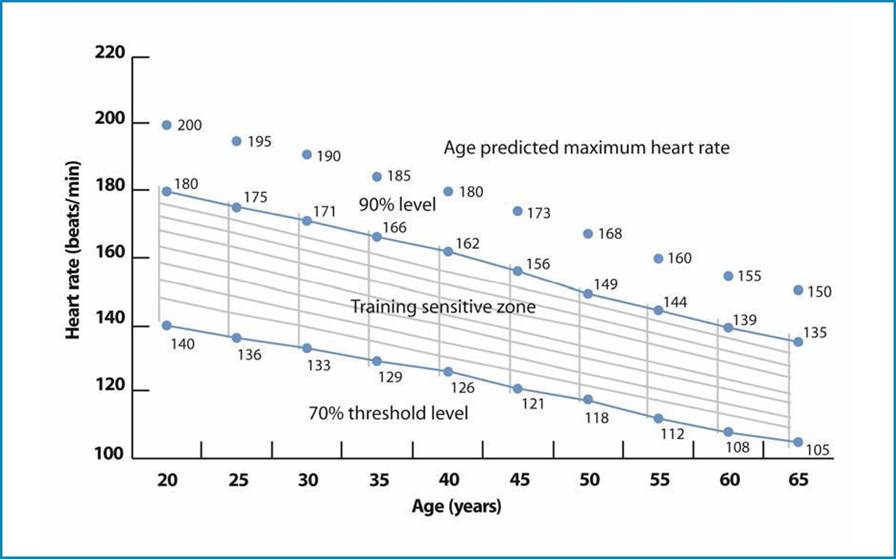
Fig. 8 The diagram shows the percentages (70-90%) of maximal heart rate (included in the depicted training zone) required to train aerobic systems of energy production in different age groups. The subject must exercise for 3-5 min in order to obtain a desired pulse rate, counting for 10 s after stopping. For example, a training heart rate equal to 70% of the age-related maximal value for a man of 40 years can be calculated using the formula (0.70¥180=126 beats per minute). Exercise must be performed at least for 20 min. A training response occurs if an exercise is performed two or preferably three times each week for at least 6 weeks. Both continuous as well as intermittent overload are effective in improving aerobic capacity. A single 3-5 min of vigorous exercise performed three times a week improves aerobic capacity as much as a less exhausting but steady-state exercise for 20 min. Our aerobic training program is conducted 3 days a week utilizing 20-30 min of continuous exercise of sufficient intensity to expend about 300 kcal. For example, subjects trained on a bicycle ergometer 20-30 min a day (~300 kcal), three times a week for 8 weeks, with a training intensity of 85% of maximum heart rate improved maximal O2 uptake by 7.8%
More on the topic Intervention Criteria:
- Risks and sources of policy failure
- Bovine Tuberculosis in Uganda
- REVIEW OF FORENSIC ASSESSMENT INSTRUMENTS
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- FIVE COMPONENTS OF LEGAL COMPETENCIES