LINKS BETWEEN FACTORS IMPLICATED IN DISEASE PROGRESSION AND APOPTOSIS
A number of the factors demonstrated to impact disease progression in cohorts of HIV-seropositive individuals also influence apoptosis (Table 21.2). Viral burden is clearly linked to disease progres- sion.67 Some studies have documented a correlation between viral load and level of activation- induced or Fas-mediated apoptosis,68,69 whereas other studies, including one that measured apoptosis in lymphoid tissue, have failed to demonstrate a relationship.70 These conflicting results may be explained by differences in methodologies and by the measurement of levels of activation-induced as opposed to spontaneous apoptosis.
HIV-2 infection is associated with a slower rate of disease progression than HIV-1.71 A study from Senegal suggests that HIV-2 is also associated with a lower level of CD4 T lymphocyte activation or apoptosis than is HIV-1 in the same population.72 As mentioned above, all the viral factors demonstrated to affect disease progression (Nef, Tat, Vpr, and Env) also influence apoptosis.1 Nef and Tat enhance Fas-mediated apoptosis.61,73 A deletion mutant of Nef has been associated with decreased apoptosis and disease progression in macaques, and Nef-deletion mutants are recognized in cohorts of LTNPs.Some of the strongest direct evidence for a direct relationship between apoptosis and a viral factor implicated in the rate of disease progression has been provided for Vpr. A specific Vpr R77Q mutation is overrepresented in LTNPs.20 Mutant Vpr resulted in less mitochondrial membrane permeabilization (MMP) and less caspase activation than did wild-type protein. Importantly, the mutant Vpr was associated with significantly less CD4 and CD8 T lymphocyte depletion when injected into Balb/c mice than was the wild-type protein.
In contrast, HIV Env encodes a selenoprotein that is homologous to human glutathione peroxidase (GPX) and that inhibits apoptosis induced by mitochondrial reactive oxygen species (ROS).74 Of interest is the observation that this gene is intact in isolates from most LTNPs but frequently demonstrates loss-of-function mutationsTABLE 21.2
Evidence for Linkage between Apoptosis and Disease Progression
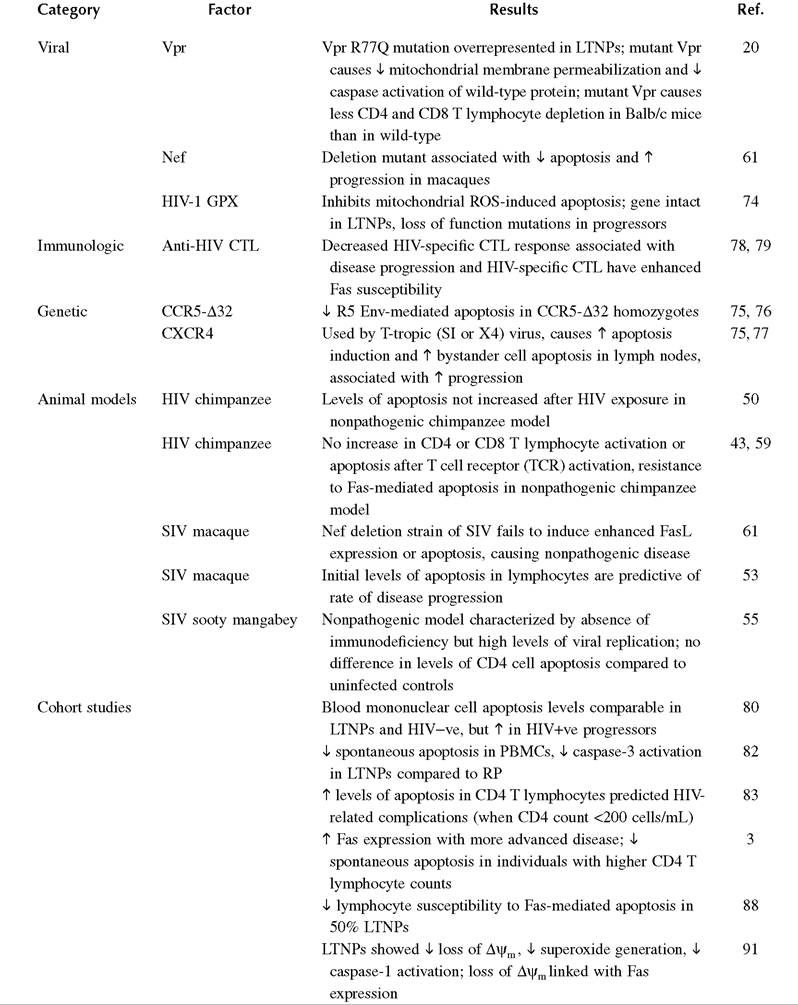
Key: ↑, increase; ¢, decrease; HIV+ve, HIV-seropositive; HIV-ve, HIV-seronegative; SIV, simian immunodeficiency virus; LTNP, long-term nonprogressor; RP, rapid progressor; CTL, cytotoxic T lymphocyte; Vpr, viral protein r; ∆ψm, inner mitochondrial transmembrane potential; ROS, reactive oxygen species.
in individuals with progressive disease. Hence, mutation in Vpr can reduce MMP, whereas maintenance of HIV-1 GPX can help prevent ROS-mediated MMP in LTNPs.
HIV Env also contributes to apoptosis induction, which might explain the relationship between changes in gp120 sequence or genetic variation in chemokine receptors and rates of disease progression. Experiments with lymphocytes derived from CCR5-∆32 homozygous individuals confirm that CCR5 contributes to R5 Env-mediated apoptosis.75,76 Furthermore, a T-tropic (SI or X4) virus that uses CXCR4 and that is associated with more rapid disease progression is also associated with greater levels of apoptosis induction75 and enhanced bystander cell apoptosis in lymph nodes.77
Many of the other host factors linked to disease progression have a potential direct or indirect link to CTL responses against HIV. Advanced stages of HIV infection may be associated with greater levels of CD8 T lymphocyte apoptosis and a lack of HIV-specific CTL responses.78 HIV- specific CD8 T lymphocytes have enhanced Fas susceptibility, as compared with CMV-specific T lymphocytes from the same individuals.79 Hence, levels of CTL apoptosis may have an indirect effect on disease progression.