ANALYSIS OF APOPTOSIS IN PATIENT COHORTS WITH DEFINED RATES OF DISEASE PROGRESSION
Despite the indirect links between levels of apoptosis and markers of disease progression, there is much less information available from well-defined clinical cohorts. A study comparing a small number of LTNPs to individuals with progressive disease or HIV-seronegative controls found that spontaneous, activation-induced, and Fas-mediated apoptosis in unsorted peripheral blood mononuclear cells (PBMCs) was increased in HIV-seropositive individuals but comparable in LTNPs and HIV-seronegative individuals.80 Levels of spontaneous apoptosis correlated directly with T lymphocyte activation markers and inversely with the percentage of CD4 T lymphocytes.
Glutathione was reduced in lymphocytes from LTNPs compared with seronegative controls, suggesting that the LTNP lymphocytes were subject to greater oxidative stress, but the reduction in glutathione was even greater in lymphocytes from individuals with progressive disease. A larger cohort of HIV-seropositive individuals, some of whom were receiving antiretroviral therapy, was studied by Gougeon and colleagues.81 Culture ex vivo resulted in enhanced spontaneous and activation-induced apoptosis in CD4 and CD8 T lymphocytes from HIV-seropositive individuals. LTNPs had similar levels of apoptosis, and RPs had higher levels of apoptosis than in seronegative controls. Apoptosis correlated with activation markers and was inversely correlated with percentage of CD4 T lymphocytes.Another group analyzing a well-defined group of LTNPs from San Francisco documented decreased spontaneous apoptosis in PBMCs from LTNPs and decreased rates of caspase-3 activation compared with progressors.82 However, in this study, rates of activation-induced cell death using two separate stimuli (pokeweed mitogen and staphylococcal enterotoxin B) were no different between LTNPs and progressors, although by some, but not all, analyses performed, there was a significant increase in rates of activation-induced apoptosis between LTNPs and seronegative individuals.
This study examined only individuals who were not receiving antiretroviral therapy. It should be noted that this study measured apoptosis in PBMCs and used specific comparator groups. Comparator groups for LTNPs were either LTNPs who subsequently developed disease progression (SPs with a comparable duration of infection to LTNPs) or recent seroconvertors with comparable CD4 counts to the LTNPs. This allowed the authors to conclude that duration of infection was not associated with level of apoptosis. Increased levels of apoptosis were seen at an early stage of HIV infection in those with progressive disease. Viral load, which was significant in many of this cohort of LTNPs, was not correlated with level of apoptosis in the LTNP but was correlated with level of apoptosis in the recent seroconvertors. Furthermore, it was suggested that when the group with long-term infection was considered as a whole (LTNPs and SPs), spontaneous, but not activation- induced, apoptosis correlated with the likelihood of a decline in CD4 T lymphocyte count.Another study also noted increased spontaneous apoptosis in lymphocytes in asymptomatic seropositive individuals in early stages of disease but lower levels of spontaneous apoptosis in LTNPs.4 In a longitudinal follow-up of asymptomatic individuals, the rate of CD4 T lymphocyte decline was directly correlated with the level of spontaneous lymphocyte apoptosis. An additional study suggested that spontaneous ex vivo apoptosis correlated with complications during short-term follow-up. In this case, high levels of spontaneous apoptosis in CD4 T lymphocytes, as measured by Annexin-V binding, were predictive of HIV-related complications in the subset of individuals with CD4 T lymphocyte counts sFas level.86 In that study, sFasL correlated directly with viral load and inversely with total lymphocyte count. Again, the confounding effects of antiretroviral therapy are apparent, and these studies emphasize the discordance between sFas and sFasL and disease progression. As the function of membrane-bound FasL is better characterized than sFasL, the significance of findings relating levels of sFas and sFasL remains unclear.87 Intriguingly, decreased susceptibility of lymphocytes to Fas- mediated apoptosis was noted in 9 of 18 (50%) LTNPs in another study.88 In this study, parents of two of the LTNPs were analyzed, and in each case, one parent showed decreased Fas susceptibility.
Creation of a hybrid cell from Fas-susceptible cells and these Fas-resistant cells suggested that the Fas-resistant cells contained a molecule involved in Fas signal transduction that exerted a dominant negative effect. Fas ligation is associated with sphingomyelin breakdown and accumulation of intracellular ceramide.89 Analysis of a defined Italian cohort of LTNPs (infected by intravenous drug abuse and not receiving antiretroviral therapy) demonstrated lower levels of intracellular ceramide in PBMCs than in a group of individuals with AIDS, although the levels were higher in the LTNPs than in seronegative controls.90 In addition, LTNPs demonstrated lower percentages of apoptotic CD4 or CD8 T lymphocytes than did individuals with AIDS. In a separate study, the same cohort of LTNPs demonstrated a lower percentage of Fas or FasL positive cells than did the group with AIDS.91 Fas-mediated apoptosis was also observed to be associated with impairment of CD45 tyrosine phosphatase activity, and CD45 tyrosine phosphatase was not impaired in LTNPs.92 The impairment of CD45 tyrosine phosphatase activity may be related to oxidative stress and depletion of the intracellular antioxidant glutathione (GSH),93 although others failed to show restoration of CD45 phosphatase activity after antioxidant treatment.80Evidence was also presented for involvement of the mitochondrial pathway of apoptosis induction in HIV-associated lymphocyte apoptosis.1 In this regard, the same cohort of Italian LTNPs was studied for evidence of loss of inner mitochondrial transmembrane potential (∆ψm) and superoxide generation.91 In this study, LTNPs had less loss of ∆ψm and less superoxide generation as well as less caspase-1 activation. Loss of ∆ψm was associated with Fas expression, and lower levels of both
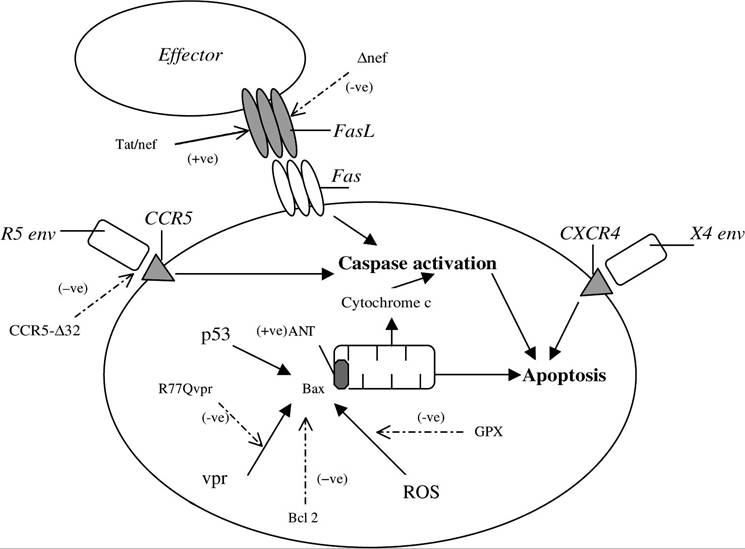
FIGURE 21.1 Factors influencing apoptosis and rate of progression.
Outlined are factors implicated in the induction of lymphocyte apoptosis. Factors that result in slower disease progression are represented by dashed arrows, (-ve). Mitochondrial permeabilization is shown in a simplified schematic, as many of the factors interact with each other. (Key: Vpr, viral protein r; ROS, reactive oxygen species; FasL, Fas ligand; GPX, human glutathione peroxidase; ANT, adenine nucleotide translocator.)parameters were apparent in LTNPs. Furthermore, Ledru and colleagues demonstrated that susceptibility to apoptosis in different lymphocyte subsets was related to the level of Bcl-2 expressed and that this correlated with disease progression.94 As expression of Bcl-2 family members regulates induction of MMP, this provides further insight into how molecular pathways that regulate apoptosis may influence rates of disease progression.95 The tumor suppressor p53 also plays a role in induction of mitochondrial pathways of apoptosis in certain settings, such as DNA damage pathways, via its effects on Bcl-2 family members.96-99 p53 is upregulated in HIV-seropositive progressors relative to LTNPs or seronegative controls.100 Figure 21.1 summarizes some of the main factors implicated in both modulating apoptosis and retarding disease progression.
More on the topic ANALYSIS OF APOPTOSIS IN PATIENT COHORTS WITH DEFINED RATES OF DISEASE PROGRESSION:
- LINKS BETWEEN FACTORS IMPLICATED IN DISEASE PROGRESSION AND APOPTOSIS
- RATES OF HIV DISEASE PROGRESSION
- EVIDENCE FOR AN INFLUENCE OF APOPTOSIS IN DISEASE PROGRESSION IN LENTIVIRUS INFECTION
- 21 Correlations between Apoptosis and HIV Disease Progression
- suPAR AND HIV DISEASE PROGRESSION
- HOST GENETIC FACTORS THAT INFLUENCE DISEASE PROGRESSION
- CONTRIBUTION OF VITAMIN D ON PROTECTION/RISK TO HIV INFECTION AND DISEASE PROGRESSION TO AIDS
- Evaluation of the Patient With Renal Disease
- APOPTOSIS IN ANIMAL MODELS OF HIV-1 DISEASE
- 18 Apoptosis in Organ Culture and Animal Models of HIV Disease
- Rates of return and investment rates in poor countries
- Understanding rates of return and investment rates in poor countries: aggregative approaches
- Understanding rates of return and investment rates in poor countries: non-aggregative approaches