IMPACT OF ANTIRETROVIRAL THERAPY ON LEVELS OF LYMPHOCYTE APOPTOSIS
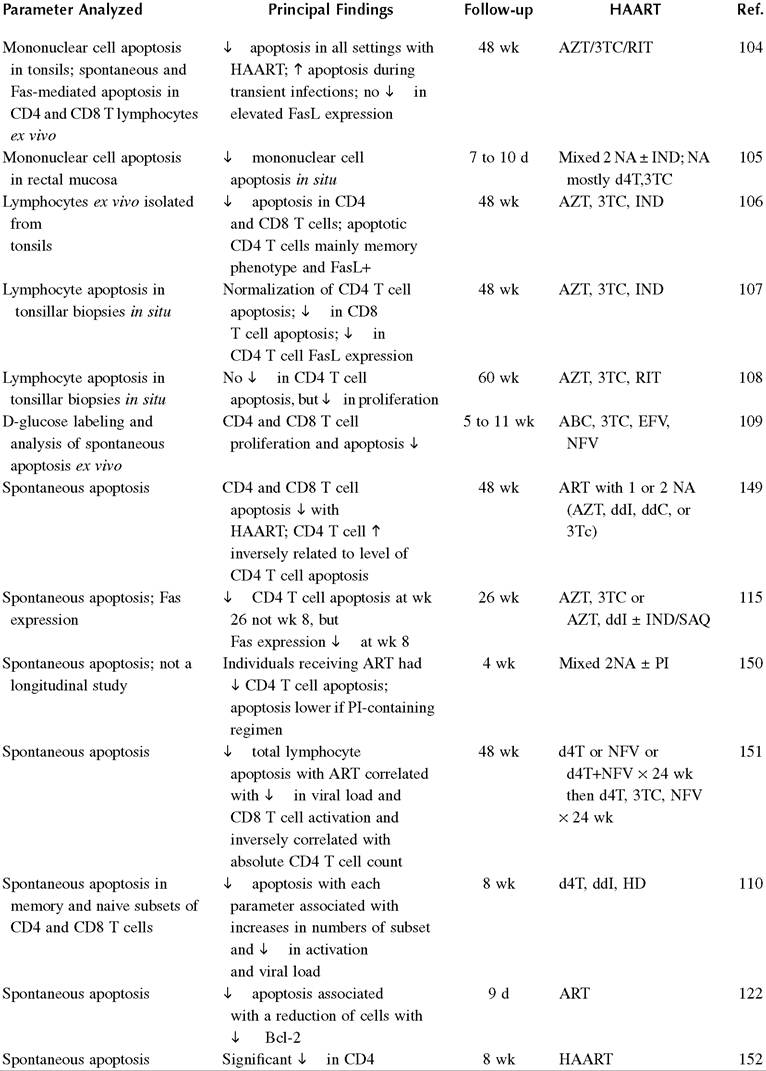
The benefits of combination antiretroviral therapy were demonstrated by improved survival and fewer opportunistic infections.101 These outcomes were associated with improvement in immunologic dysfunction, such as reduced markers of activation and improved CD4 T lymphocyte response to recall antigens.102 Despite this, several markers of defective cellular immune responses associated with HIV infection persist, despite the use of highly active antiretroviral therapy (HAART).103 A large number of studies have suggested that levels of apoptosis are decreased in association with HAART, and these are summarized in Table 21.3.
TABLE 21.3
Relationship of Lymphocyte Apoptosis Levels to Antiretroviral Therapy
T cell but not CD8 T cell or
PBMC apoptosis
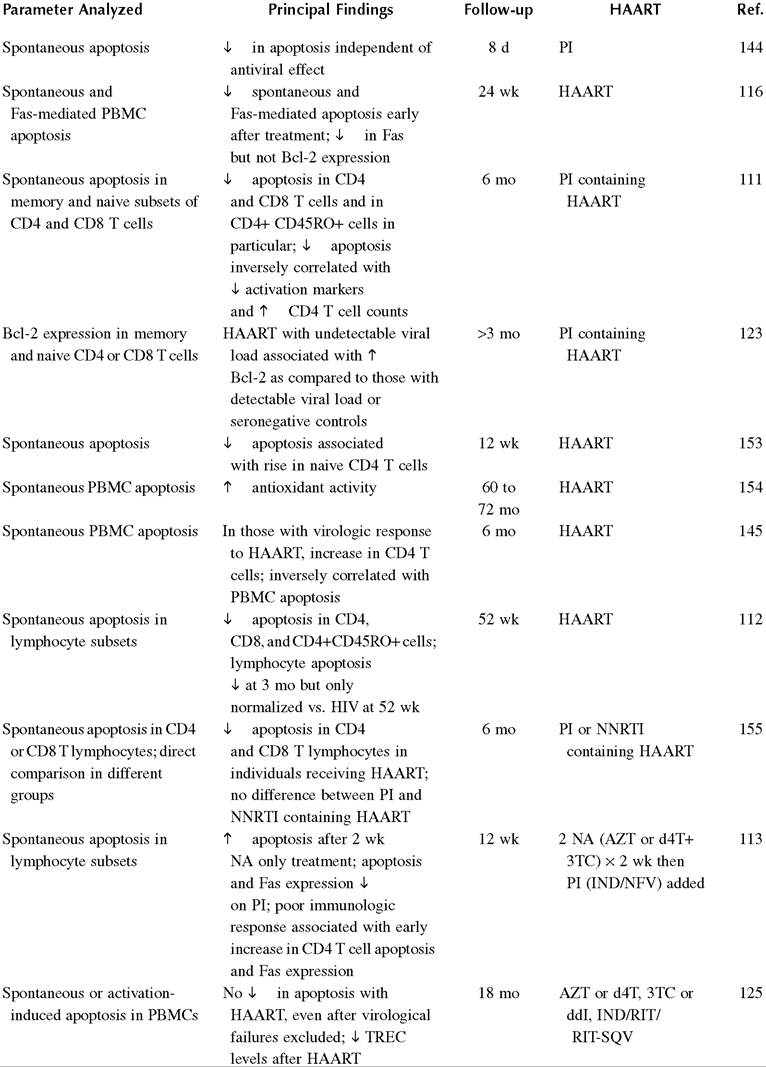
TABLE 21.3 (Continued)
Relationship of Lymphocyte Apoptosis Levels to Antiretroviral Therapy
(continued)
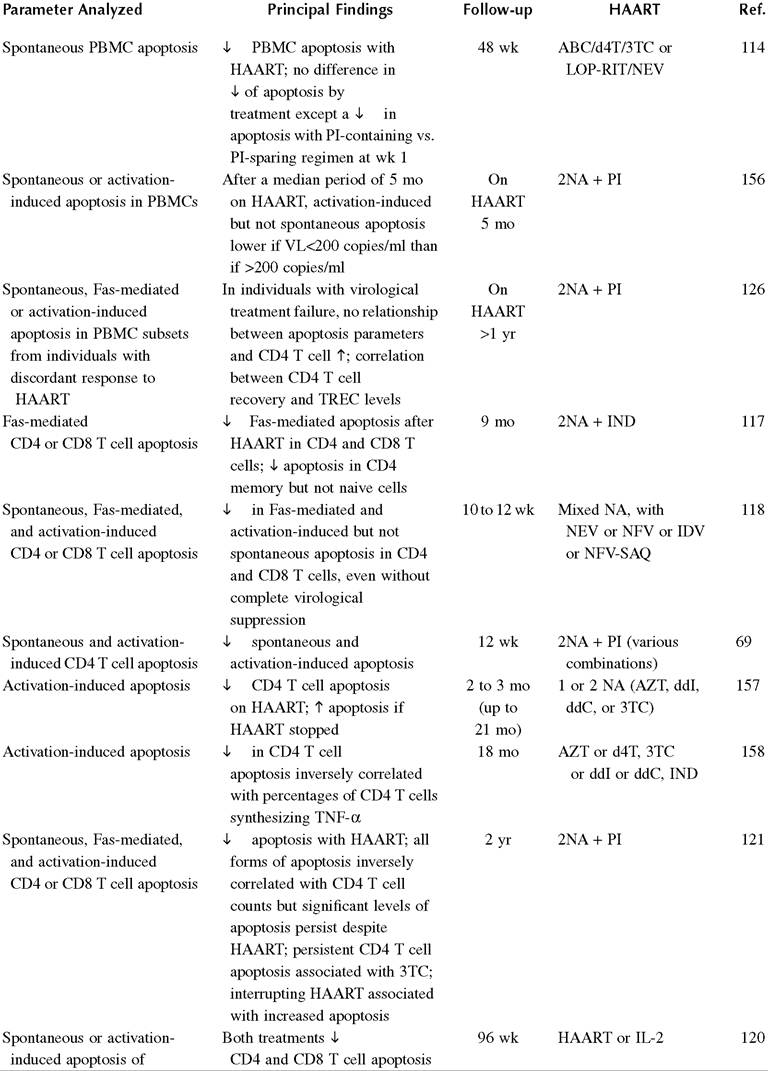
TABLE 21.3 (Continued)
Relationship of Lymphocyte Apoptosis Levels to Antiretroviral Therapy
CD4 and CD8 T cells
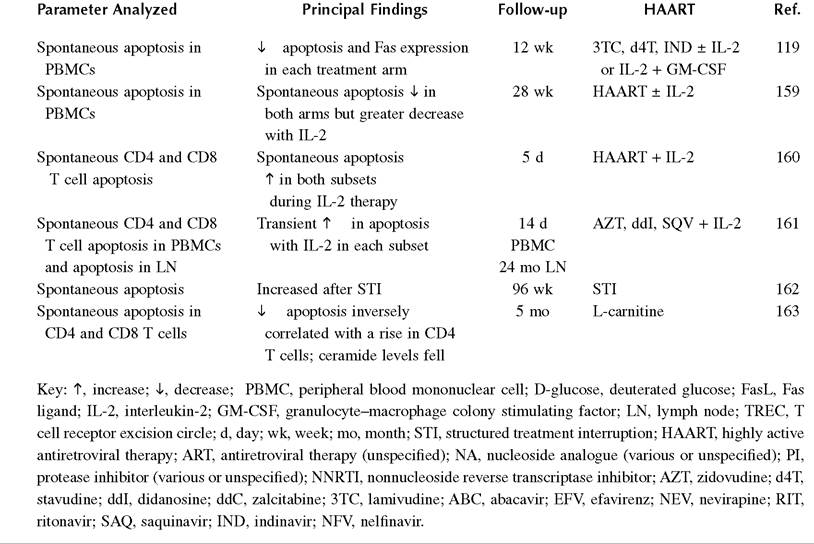
TABLE 21.3 (Continued)
Relationship of Lymphocyte Apoptosis Levels to Antiretroviral Therapy
An important source of information included analysis of apoptosis in vivo.
Analysis of tonsillar biopsies from a subset of individuals enrolled in ACTG 315 demonstrated decreased numbers of Terminal deoxynucleotidyltransferase dUTP nick and labeling (TUNEL) -positive mononuclear cells after initiation of antiretroviral therapy. This was associated with increased CD4 T lymphocyte counts and decreased viral loads, although the exact nature of the TUNEL positive cells was not determined.104 Kotler and colleagues demonstrated a decline in mononuclear cell apoptosis in the lamina propria of rectal mucosa in the first 7 days after initiation of antiretroviral therapy105 in association with increases in CD4 T cell numbers and declines in HIV viral burden. Others demonstrated declines in both CD4 and CD8 T lymphocyte apoptosis ex vivo, in response to HAART in lymphocytes isolated from tonsillar biopsies.106 The same group demonstrated decreased percentages of both CD4 and CD8 T lymphocyte apoptosis in situ in tonsillar biopsies with HAART. The levels of CD4 T lymphocyte apoptosis normalized, whereas the level of CD8 T lymphocyte apoptosis decreased with 48 weeks of HAART, in association with a decline in HIV viral load.107 However, another important study did not reach the same conclusion. Zhang and colleagues, analyzing tonsillar biopsies or lymph node biopsies from a group of individuals receiving HAART or seronegative controls, failed to demonstrate decreased CD4 T lymphocyte apoptosis, even though they noted decreased cell proliferation after HAART.108 In this study, levels of CD4 T lymphocyte apoptosis were enhanced in HIV-seropositive individuals compared with seronegative controls at baseline. The authors interpreted the continued elevation in TUNEL positive cells as reflecting a failure in clearance of early apoptotic cells.The majority of studies have, however, examined apoptosis ex vivo in PBMC or in lymphocyte subsets. The parameter measured was most often spontaneous apoptosis, but Fas-mediated apoptosis or activation-induced apoptosis was also measured. In elegant studies using deuterated glucose to label DNA in proliferating cells and ex vivo analysis of PBMC, followed by mathematical modeling, Mohri and colleagues demonstrated that antiretroviral therapy reduced both proliferation and apoptosis in CD4 T lymphocytes in association with increases in CD4 T lymphocyte numbers.109 This finding is in agreement with the majority of the 40 studies outlined in Table 21.2. Most of these studies show decreased levels of apoptosis either in PBMCs or, more specifically, CD4 and CD8 T lymphocytes. In most cases, this has occurred in response to protease inhibitor (PI)-based therapy.
Usually, decreased apoptosis correlated with the immunologic response to therapy, as defined by the increase in CD4 T lymphocyte counts. CD45RO+ memory cells constitute the subset most susceptible to HAART-induced inhibition of apoptosis,106,110-112 and markers of cell activation are decreased.106,110,113,114 Apoptosis reduction is associated with decreased Fas expression and decreased Fas-mediated apoptosis,69,113,115-121 but in a few studies, it is also associated with a rise in Bcl-2 expression.122,123 Recently, it was suggested that HIV Env can induce p53-mediated apoptosis with upregulation of the proapo- ptotic BH-3-only Bcl-2 family member Puma. In keeping with this observation, Puma is upregulated in antiretroviral naive, HIV-infected individuals, but this is reversed by initiation of HAART.124Not all studies confirm a beneficial effect of HAART on apoptosis. A number show no reduction in the level of apoptosis by HAART or persistent elevation of apoptosis for long periods after HAART initiation.115,121,125,126 Elevated sFas levels may not be corrected by up to a year of HAART.127 The reason for these differences is not immediately obvious, as similar parameters of apoptosis were measured in many studies. One source of variation is that intercurrent illnesses may cause transient elevations in apoptosis, just as they may cause viral blips.104 The effect of these may be quite marked in series containing small numbers of individuals. Another potentially confounding variable is the effect of antiretroviral therapy, as discussed elsewhere in this book. AZT or 3TC may enhance apoptosis,121,128 although a further study has suggested that AZT and 3TC may be associated with a more marked decrease in apoptosis than AZT and ddI.129 The nonnucleoside reverse transcriptase inhibitor (NNRTI) efavirenz may enhance caspase activation and mitochondrial membrane perme- abilization in vitro.130 Conversely, the protease inhibitors ritonavir, saquinavir, and nelfinavir were shown to decrease apoptosis in lymphocytes and bone marrow progenitors in vitro.131,132 PIs may prevent activation-associated mitochondrial hyperpolarization.132,133 Differences may exist between PIs, as evidenced by reports that Indinavir does not inhibit apoptosis.134,135 In one of these studies, low doses of Indinavir helped promote lymphoproliferation in vitro,135 whereas in a second study, using higher doses, lymphoproliferation was blocked.134 Although these findings could be interpreted as being due to differences between PIs of different structures, one of these studies also tested Saquinavir and the other Nelfinavir with similar results.134,135 One of these studies used short-term culture, and this might translate into a later inhibition of apoptosis.134 The other study involved up to 14 days of in vitro culture with PIs before apoptosis assessment and only detected reduced apoptosis with the highest dose of each PI, administered for 14 days to PBMCs from HIV-seropositive but not from HIV-seronegative individuals.135 The exact reasons for the different findings are unclear.136 However, a review of individuals receiving postexposure prophylaxis was unable to detect any alteration in apoptosis with AZT; AZT plus 3TC; or AZT, 3TC, plus Indinavir,137 whereas a different study of postexposure prophylaxis showed reduced susceptibility to apoptosis after Nelfinavir, AZT, and 3TC.138 This study does not exclude the possibility of an indirect effect on lymphocyte apoptosis in an activation-specific context, such as by HIV infection in vivo or by ex vivo culture of lymphocytes from HIV-seronegative individuals.
Nevertheless, a role for viral independent effects, which include apoptosis inhibition, is supported by reports that PI-based therapy may result in equivalent immunologic responses, despite inferior virological responses compared with regimens not containing a PI.139,140 Also, the observation that NNRTI-based therapy may be associated with lower levels of CD4 T lymphocyte recovery than PI-based regimens is consistent with this possibility.141 These findings may be partly explained by differing effects on reduction of apoptosis. The fact that the majority of regimens used in the studies in Table 21.2 contain PIs is in keeping with this observation.However, some of these studies do not involve PI-based therapy,110 and a study that compared PI- and NNRTI-based regimens found no differences in rates of CD4 T lymphocyte recovery or apoptosis.114 One interpretation for these apparently disparate findings is that direct induction of apoptosis, which kills viral-infected cells or depletes activated cells capable of becoming infected with HIV, might aid the virological response.142 Hence, this helps reduce apoptosis in bystander cells, whereas direct inhibition of bystander apoptosis, particularly in the context of suboptimal virological response by PI, might help boost CD4 T lymphocyte counts.
More on the topic IMPACT OF ANTIRETROVIRAL THERAPY ON LEVELS OF LYMPHOCYTE APOPTOSIS:
- Supportive Therapy
- HIV counselling and combination antiretroviral therapy
- Prognostic markers
- Twenty years after the first antibody test for the human immunodeficiency virus (HIV), highly active antiretroviral therapy (HAART) became available in Western countries.
- Antiretroviral Therapy Today
- Antiretroviral Therapy and Metabolic Disorders
- ALL REVVED UP WITH NO PLACE TO GROW—ACTIVATION- INDUCED CELL DEATH (AICD) and peripheral deletion
- HiV-I-INDUCED APOPTOSIS
- CD8+ T LYMPHOCYTES IN HIV-1 INFECTION
- IS CHRONIC IMMUNE ACTIVATION ALONE ENOUGH TO INDUCE CD4+ T CELL LOSS?