RESULTS
CD4+ Lymphocytes Increase and CD8+ Lymphocytes Decrease in Response to α1PI Replacement Therapy
To examine the interrelationship between α1PI concentration and CD4+ lymphocyte numbers, data were examined from a blinded study conducted to monitor hematologic changes following weekly infusions of α1PI (60 mg/kg) in 11 individuals with genetic α1PI deficiency (PIzz) who had never before received α1PI therapy.
Treatment with α1PI caused an increase in lymphocytes in 10 of these individuals (data not shown), suggesting that such treatment might benefit HIV-1+ patients.Two HIV-1 patients, Alpha and Beta at different stages of disease (Table 1) received weekly infusions of 120 mg/kg α1PI augmentation. Two additional HIV-1 patients, Gamma and Delta, with apriori evidence of abnormal immune status received the same therapy. The ability of Gamma to respond to antigen was impaired (positive PPD followed by negative PPD), and Delta exhibited systemic inflammation. Finally, 2 non-HIV-1 patients were included in the study, PIzz-1 and PIzz-2, who manifested normal numbers of CD4+ lymphocytes and a diagnosis of emphysema in the context of genetic α1PI deficiency. The PIzz patients received half-dose weekly infusions of 60 mg/kg α1PI augmentation. Patients Delta and PIzz-2 were included only in CD4+ lymphocyte functional analyses (see Methods).
HIV-1+ patients Alpha, Beta, and Gamma (Fig. 1) and both PIzz patients (not depicted) responded to therapy with an initial burst of lymphocytes. After 2 wks of therapy, patients Alpha and Beta achieved normal numbers of CD4+ lymphocytes with increases from 297 to 710 and from 276 to 393 cells/pl, respectively.
OiAntitrypsin Therapy Increases CD4+ Lymphocytes Soluble Factors Mediating Innate Immune Responses to HIVInfection 105
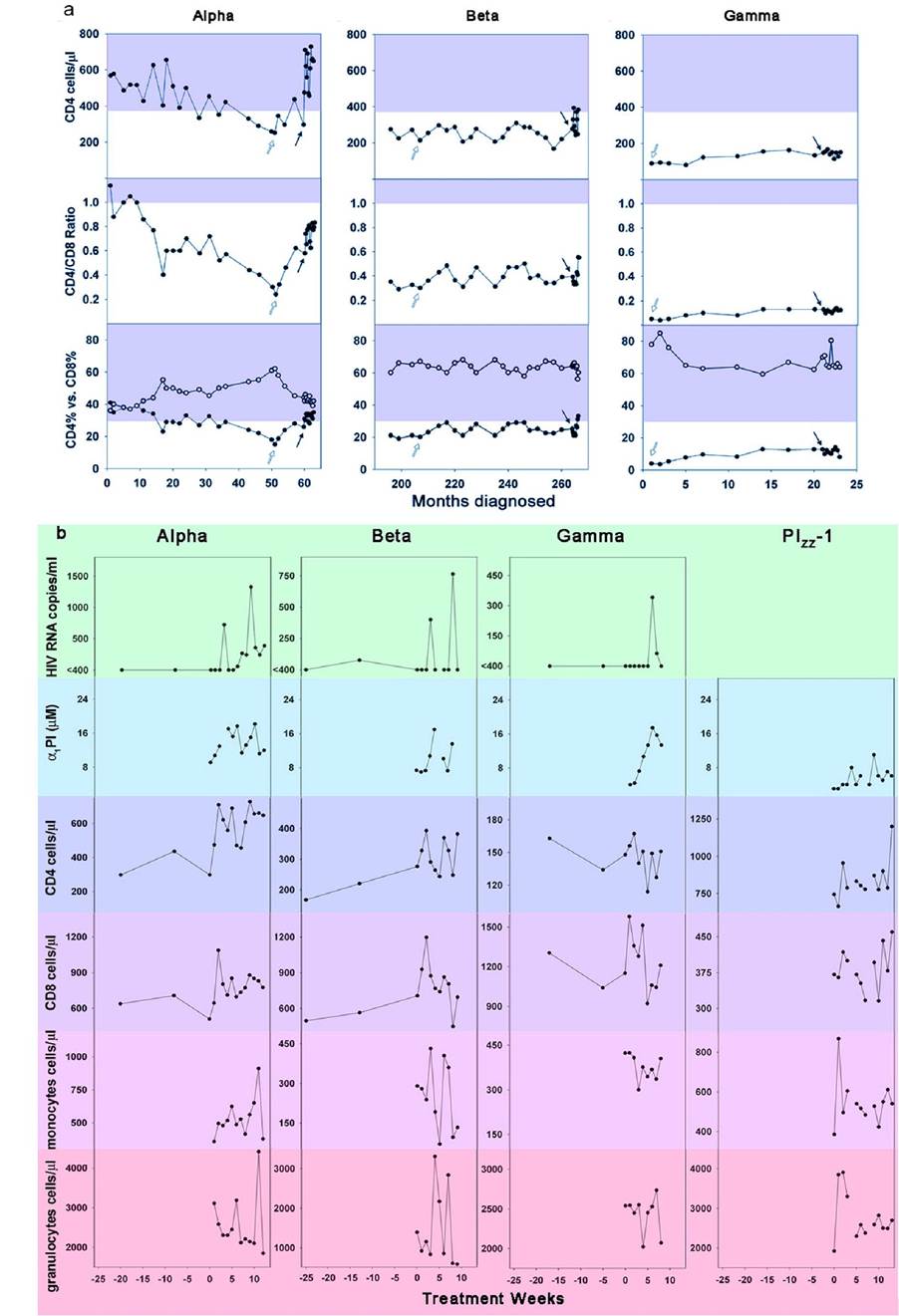
Figure 1: Corresponding cyclic variation in blood cells, α1PI, and viral load in patients treated with α1PI augmentation.
Baseline CD4+ lymphocyte levels were determined in patients Alpha, Beta, and Gamma to be 297, 276, and 148 cells∕μl, respectively. Blood was collected prior to infusion, and each data point represents patient status at 7 days post-infusion such that wk 9 represents patient status after the 8th wk of treatment. (a) CD4+ lymphocytes, CD4/CD8 ratios, and CD4% (•) vs. the corresponding CD8% (o) are presented with respect to months of disease diagnosis. Shaded areas represent normal reference ranges for CD4, CD4/CD8 ratio, and CD4%. Black arrows designate initiation of Zemaira® treatment. White arrows designate initiation of antiretroviral therapy. (b) Patients Alpha, Beta, Gamma, and PIzz-1 were monitored weekly for changes in blood cell subtypes and serum levels of α1PI. HIV-1+ patients were monitored for changes in HIV RNA. Treatment wk 0 represents baseline pre-treatment values. In some instances, blood samples were not acceptable for measuring blood cells, HIV RNA, or α1PI due to delay in sample delivery or hemolysis, and these are depicted as gaps in the line graphs.Patients PIzz-1 and PIzz-2 increased from 743 to 954 and from 899 to 1024 cells∕μl, respectively. Patient Beta, who had never exhibited CD4+ lymphocytes in the normal range in more than 20 years, even continued to exhibit the normal range of CD4+ lymphocytes 2 wks after treatment stopped with 382 cells∕μl. Using regression analysis, this duration of benefit was attributed to α1PI therapy (Fig. 2). Patient Alpha who was first infected 5 years prior to the study had not exhibited CD4+ lymphocytes within the normal range in 2 years. At 5 wks and 14 wks after treatment stopped, patient Alpha continued to be in the normal range with 470 cells∕μl. By regression analysis, this duration of benefit appeared to be related to antiretroviral medication as well as α1PI therapy (Fig.
2). Patient Gamma, who was known to have lost immune function, showed an increase from 148 to 167 cells∕μl and never achieved normal numbers of CD4+ lymphocytes.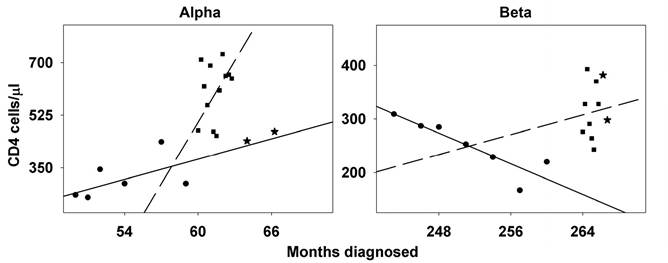
Figure 2: Duration of increase in CD4+ lymphocytes following α1PI therapy. Comparison of the change in CD4+ lymphocytes represented in Fig. 1 before (∙), during (■), and after (W) α1PI augmentation therapy demonstrates that the duration of benefit is 1 or 2 weeks post-treatment (Patient Beta), but not 5 or 14 weeks post-treatment (Patient Alpha). Linear regression of CD4+ lymphocyte changes before (solid line) and during (dashed line) show significant improvement.
CD4+ Lymphocyte Cycling is Sinusoidal. All Patients Exhibited Cyclic Changes in CD4+ Lymphocytes (Fig. 3).
Patients Alpha, Beta, and PIzz-1 exhibited sinusoidal changes in CD4+ lymphocytes with periodicity 23±3.5 days (Fig. 3). Patient Gamma exhibited sinusoidal changes in CD4+ lymphocytes with periodicity of 15 days. Of important note, patient PIzz-1, but none of the HIV-1 patients, exhibited sinusoidal changes in CD8+ lymphocytes. In patient Alpha, the sinusoidal wave was damped exhibiting decreased amplitude. In patients Beta and Gamma, the oscillations sloped downward. The 5 week treatment period for patient PIzz-2 was insufficient for determining the occurrence of periodicity. The CD4∕CD8 ratio in patients Alpha, Beta, and PIzz-1 increased following α1PI therapy at a rate of 0.02±0.008 per week (Figs. 1 and 3). The degree of increase in the CD4+ lymphocyte axis of oscillation in patients Alpha, Beta, Gamma, and PIzz-1 was inversely related to baseline CD8+ lymphocyte percentage (n=4, r2=0.99, pand PIzz-1 (d) over the course of Zemaira® therapy.
CD4+ lymphocyte oscillation is defined by f(x) = y0+ a Ć sin [(2πxZb)+c] where y0 = axis of oscillation, a = amplitude, x = days in treatment, b = wavelength, and c = phase shift from day 0. Each sine curve has a fit of r2>0.99, α=0.05, power of test = 1.0, and each variable contributed to the equation with pnormal numbers of CD4+ lymphocytes in a subset of HIV-1+ patients who are on antiretroviral therapy and have functioning lymphatic and hematopoietic tissue.Acknowldegements
We wish to thank CSL Behring for contributing Zemaira®; BioReferences Laboratories for performing routine patient analyses; M.A. Reeves for data analysis; P Quartararo and Dr. M. Murtiashaw for manuscript advice; the many volunteers and patients who participated by contributing their time and blood for this study; the InfusionZTransfusion Unit nurses and Drs. A. Distenfeld, E. Medina, and M. LaBrunda for assisting with patient follow-up. This study was supported by the Harry Winston Research Foundation.
author information
V.R. is Senior Vice President of Research and Development, CSL Behring. All other authors declare no competing financial interest.
REFERENCES
[1] Cepinskas G, Sandig M, Kvietys PR. PAF-induced elastase-dependent neutrophil transendothelial migration is associated with the mobilization of elastase to the neutrophil surface and localization to the migrating front. J Cell Sci. 1999;112 ( Pt 12):1937-1945.
[2] Lapidot T, Petit I. Current understanding of stem cell mobilization: the roles of chemokines, proteolytic enzymes, adhesion molecules, cytokines, and stromal cells. Experimental hematology. 2002;30(9):973-981.
[3] Bristow CL, Mercatante DR, Kole R. HIV-1 preferentially binds receptors copatched with cell-surface elastase. Blood. 2003;102(13):4479-4486.
[4] Cao C, Lawrence DA, Li Y, Von Arnim CA, Herz J, Su EJ, et al. Endocytic receptor LRP together with tPA and PAI-1 coordinates Mac-1-dependent macrophage migration.
The EMBO journal. 2006;25(9):1860-1870.[5] Kounnas MZ, Church FC, Argraves WS, Strickland DK. Cellular internalization and degradation of antithrombin III-thrombin, heparin cofactor II-thrombin, and alpha 1-antitrypsin-trypsin complexes is mediated by the low density lipoprotein receptor-related protein. The Journal of biological chemistry. 1996;271(11):6523-6529.
[6] Bristow CL, Patel H, Arnold RR. Self antigen prognostic for human immunodeficiency virus disease progression. Clinical and diagnostic laboratory immunology. 2001;8(5):937-942.
[7] Huber R, Carrell RW. Implications of the three-dimensional structure of alpha 1-antitrypsin for structure and function of serpins. Biochemistry. 1989;28(23):8951-8966.
[8] Bayer H. Prolastin Product Monograph.: www.talecris.com 2003.
[9] Bristow CL, Di Meo F, Arnold RR. Specific activity of alpha1proteinase inhibitor and alpha2macroglobulin in human serum: application to insulin-dependent diabetes mellitus. Clinical immunology and immunopathology. 1998;89(3):247-259.
[10] Krutzik PO, Nolan GP. Fluorescent cell barcoding in flow cytometry allows high-throughput drug screening and signaling profiling. Nature methods. 2006;3(5):361-368.
[11] Chrousos G. Adrenocorticoids & Adrenocortical Antagonists. In: Katzung B, ed. Basic & Clinical Pharmacology: McGraw-Hill Companies. 2007.
[12] Horwitz M, Benson KF, Person RE, Aprikyan AG, Dale DC. Mutations in ELA2, encoding neutrophil elastase, define a 21-day biological clock in cyclic haematopoiesis. Nature genetics. 1999;23(4):433-436.
[13] Congote LF, Temmel N. The C-terminal 26-residue peptide of serpin A1 stimulates proliferation of breast and liver cancer cells: role of protein kinase C and CD47. FEBS letters. 2004;576(3):343-347.
[14] Mehigan BJ, Hartley JE, Drew PJ, Saleh A, Dore PC, Lee PW, et al. Changes in T cell subsets, interleukin-6 and C-reactive protein after laparoscopic and open colorectal resection for malignancy. Surgical endoscopy.
2001;15(11):1289-1293.[15] Donskoy E, Foss D, Goldschneider I. Gated importation of prothymocytes by adult mouse thymus is coordinated with their periodic mobilization from bone marrow. J Immunol. 2003;171(7):3568-3575.
[16] Nakagawa T, Roth W, Wong P, Nelson A, Farr A, Deussing J, et al. Cathepsin L: critical role in Ii degradation and CD4 T cell selection in the thymus. Science. 1998;280(5362):450-453.
[17] He X, Kappes DJ. CD4/CD8 lineage commitment: light at the end of the tunnel? Current opinion in immunology. 2006;18(2):135-142.
[18] Tavor S, Petit I, Porozov S, Goichberg P, Avigdor A, Sagiv S, et al. Motility, proliferation, and egress to the circulation of human AML cells are elastase dependent in NOD/SCID chimeric mice. Blood. 2005; 106(6):2120- 2127.
[19] Bashir MS, Morrison K, Wright DH, Jones DB. Alpha-1 antitrypsin gene exon use in stimulated lymphocytes. Journal of clinical pathology. 1992;45(9):776-780.
[20] Winkler IG, Hendy J, Coughlin P, Horvath A, Levesque JP. Serine protease inhibitors serpina1 and serpina3 are down-regulated in bone marrow during hematopoietic progenitor mobilization. The Journal of experimental medicine. 2005;201(7):1077-1088.
More on the topic RESULTS:
- The Netherlands and the UK: The Witteveen Reports and their contradictory results
- Bovine Tuberculosis in Zambian Wildlife
- REFERENCES
- The Idiomorphic Constitution of Cyprus
- Diagnosis of Bovine Tuberculosis in Zambia
- Bovine Tuberculosis in Uganda
- Culture-Based Social Ecological Conflict Model: A New Model
- FIVE COMPONENTS OF LEGAL COMPETENCIES
- Public and professional ideas about ecology often differ
- ADDENDUM