The Natural History of HIV Infection
In the years following the time when specific diagnostic molecular assays became available (HIV serology by means of ELISA and Western-Blot techniques), we eventually recognized the rather atypical clinical evolution of HIV infection.
With infectious diseases resulting in physicians being more accustomed (with notable exceptions) to deal with acute disease forms, the multi- phasic progression of HIV infection, with long-lasting asymptomatic periods, brought to our attention a totally new infectious disease model.Well before HIV was identified as the causative agent of AIDS, a clear-cut correlation was established between the downgrading tendency of immune surveillance and the increasingly severe clinical manifestations leading eventually to death [2]. It is worth noting that 26 years after the first five AIDS patients were described as individuals developing unusual opportunistic infections and neoplasms in association to extremely low numbers of circulating CD4+ T-lymphocytes, no immunological markers better than CD4+ cells have been identified as indicator of immune status in patients with HIV infection [3]. Although exceptions are not so uncommon, the relationship between the CD4+ cell count and the likelihood of developing specific opportunistic diseases is still the best clinical rule for clinicians to rely upon in the diagnostic workup of patients with HIV infection. There are no other human diseases in which the relationship between an immunological marker and a given clinical condition is so coherent. Although the distinction between HIV infection (defined by a positive HIV serology) and AIDS (defined by a positive serology in association with some major associated disorders) is still made on a clinical ground, reliance on the number of circulating CD4+ cells is pivotal in the process of choosing diagnostic procedures and taking therapeutic decisions [4].
Based on these two markers (serology and CD4+ count), a more than approximate description of the natural history of HIV infection can be easily plotted on a graph, with the time elapsing since infection on the x axis and the absolute number of CD4+ T-lymphocytes∕μl on the y axis (Fig. 1). In the 2nd half of the 90s, a molecular marker representing the plasma concentration of HIV-specific nucleic acids became available (HIV-RNA), which made it possible to quantify the presence of HIV in the blood and to successfully relate it to clinical and immune disease progression [5].
In clinical terms, the manifestations of HIV infection can be classified in four sequential phases. In the days following infection, an acute inflammatory syndrome may take place with a rather wide variety of signs and symptoms [6]. In more than 50% of symptomatic cases, fever, pharyngitis (“mononucleosis-like syndrome”), systemic adenopathy, cutaneous rash and diffuse musculoskeletal pain are usually present, but less common disease forms are also described, with involvement of the central nervous system [7]. Acute retroviral syndrome tends to subside in a few days to several weeks; and, depending on a variety of circumstantial factors (clinical presentation, physician’s experience), it may actually be recognized or simply interpreted as a common flu-like disease. Today it is common practice to rely upon plasma HIV-RNA assays when serology is still negative and the clinical picture suggests the possibility of acute retroviral syndrome. While antiHIV antibodies may take up to several months to become detectable, the molecular evidence of HIV infection in the plasma well anticipates seroconversion, thus allowing the diagnosis of newly acquired HIV infection in the absence of detectable antiHIV antibodies [8]. It must be recognized, however, that it is not easy to estimate the rate of newly acquired HIV infection cases producing acute symptomatic disease, and the proportion of newly diagnosed infections presenting with an acute inflammatory disease form is rather low.
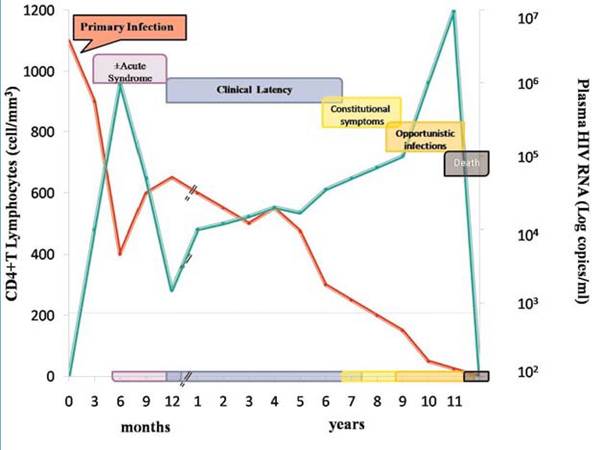
Fig.
1. The chronological relationship among immunological (CD4+T-cells) and virological (HIV-RNA) markers and the clinical evolution of HIV infection is represented. The red line refers to circulating CD4+T-lympho- cytes and the green line refers to plasma HIV-RNAAfter primary infection (which may thus pass unnoticed in a substantial proportion of cases) a prolonged asymptomatic phase follows, which usually lasts several years
[9]. With progression of immune decline, an early symptomatic phase may be recognized, with some minor clinical manifestations like pharyngeal candidiasis, systemic lymphadenopathy, seborrhoeic dermatitis
[10]. When immune deterioration gets below the threshold of 200 CD4+ T-lympho- cytes∕μl, the patient enters in the phase of highest vulnerability to opportunistic disorders, as the risk of developing overtly symptomatic opportunistic disorders increases in inverse relationship with decreasing CD4+ T-lymphocytes [11]. The clinical phase corresponding to a CD4+ cell count 10% of normal body weight), chronic fatigue and fever [16-18].
A particularly relevant position in the spectrum of the HIV-associated opportunistic infection is that of tuberculosis (TB). Active TB may develop in any human being regardless of the presence of specific immunosuppressant conditions, but as is the case with other predisposing factors, in the case of HIV infection, the risk increases several fold as compared to the general population [19]. In patients with HIV infection, the risk of developing active TB increases when the individual immune surveillance declines and such increased individual vulnerability has been demonstrated both in the case of reactivation of a pre-existing (latent) infection as well as in case of de novo exposure [20, 21]. Further to play the role of the most powerful factor predisposing to active TB, HIV infection was also found to alter the clinical presentation of the disease [22]. In a sizeable proportion of patients with low values of circulating CD4+ cells (have described a rather steady immunological condition up to 20 years since HIV was acquired [25, 26].
In the years preceding the release of effective antiretroviral regimens, the only therapeutic measures available to counteract the effects of the downgrading tendency of immune surveillance were drugs specifically active against opportunistic pathogens. Further to be used in the treatment of specific opportunistic infections, these drugs were also administered as prophylactic agents both for primary (e.g. for preventing P. jirovecii pneumonia in patients with less than 200 CD4+ T-lymphocytes/ö˛) or secondary prophylaxis (following the treatment of the first episode of opportunistic infection) of otherwise frequently occurring opportunistic infectious processes [27]. Although neither treatment or prophylaxis were able to reverse the tendency to lose immune competence over time, the life expectancy of HIV-infected patients who were carefully monitored on this basis was significantly increased in the years before HAART became available [15]. It is unclear to what extent the release of the first antiretroviral drugs contributed to this pre- HAART improvement in the life expectancy of AIDS patients. The use of azidothimidine (AZT) alone was found to delay the onset of AIDS, but no advantages were seen in terms of life duration [28].
More on the topic The Natural History of HIV Infection:
- Natural History of HIV Infection
- What is HIV counselling?
- Chapter 24 Infectious Diseases
- REFERENCES
- What Was It? What Was It Called?
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Intra-amniotic infection, meconium staining of the amniotic fluid, and meconium aspiration syndrome: what is the link?
- Interstitial Lung Disease