Diagnosis
History
• Assess for changes in diet pattern (size, number, and content of meals) and if present, the reason(s) for altered food intake.
• Unintentional weight loss of >10% body weight in the prior 6 months is associated with a poor clinical outcome.
This may not be due directly to malnutrition but rather to the underlying illness.7,8• Look for evidence of malabsorption (diarrhea, weight loss).
• For symptoms of specific nutrient deficiencies, see Table 2-3.
• Consider factors that may increase metabolic stress (e.g., infection, inflammatory disease, malignancy).
• Assess the patient's functional status (e.g., bedridden, suboptimally active).
Physical Examination
• By World Health Organization (WHO) criteria, patients can be classified by BMI as underweight (diets include a regular diet and those modified in either nutrient content (amount of fiber, fat, protein, or sodium) or consistency (liquid, pureed, soft). There are ways that food intake can often be increased:
• Aid at mealtime.
• Allow relatives and friends to supply food.
• Limit missed meals for medical tests and procedures.
• Avoid unpalatable diets. Milk-based formulas (e.g., Carnation Instant Breakfast™) contain milk as a source of protein and fat and are more palatable than many other formula diets.
• Use of calorically dense supplements (e.g., Ensure™, Boost™).
Defined Liquid Formulas (Table 2-6)
TABLE 2-6
ENTERAL FEEDING FORMULAS: COMPARING COMPOSITION
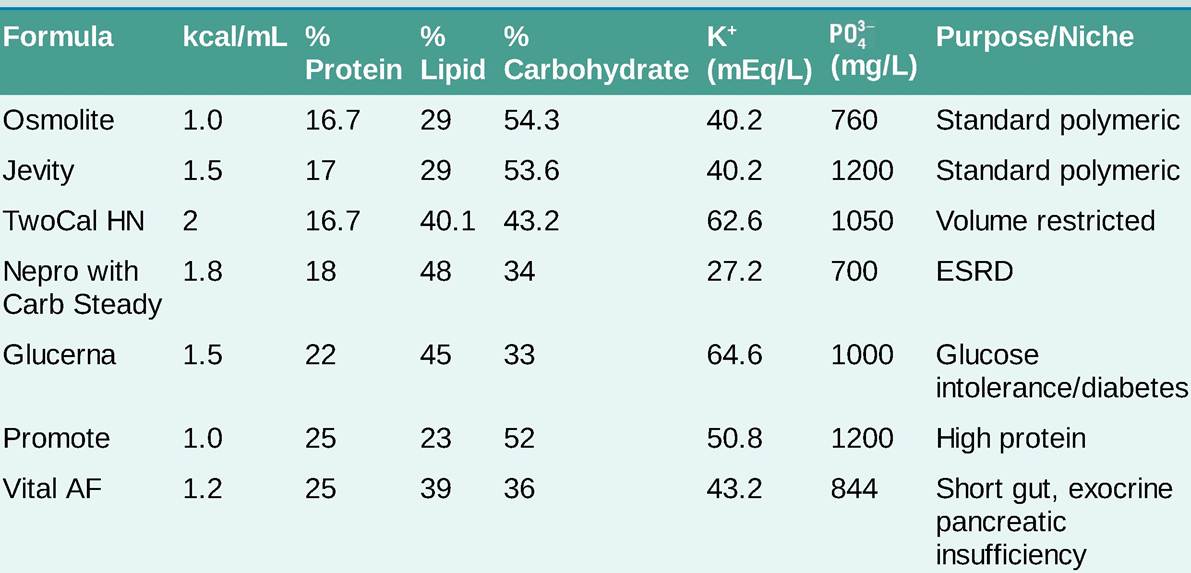

ARDS, acute respiratory distress syndrome; ESRD, end-stage renal disease; SIRS, systemic inflammatory response syndrome. Adapted from Barnes-Jewish Hospital Enteral Nutrition Formulary (2019).
• Polymeric formulas (e.g., Osmolite™, Jevity™) are appropriate for most patients. They contain nitrogen in the form of whole proteins and include blenderized food, milk-based, and lactose-free formulas. Other formulas are available with modified content including high-nitrogen, high-calorie, fiber-enriched, and low-potassium/phosphorus/magnesium.
• Semielemental oligomeric formulas (e.g., Peptamen™) contain hydrolyzed protein in the form of small peptides and free amino acids. Although these formulas may have benefit in those with exocrine pancreatic insufficiency or short gut, pancreatic enzyme replacement is a less expensive and an equally effective intervention in most patients.
• Elemental monomeric formulas (e.g., Vivonex™, Glutasorb™) contain nitrogen in the form of free amino acids and small amounts of fat (continuous (24 hours per day) feeding should receive basal and bolus insulin when clinically stable.
î For patients receiving nocturnal tube feeding, intermediate-duration insulin (e.g., NPH) administered with initiation of feeding is a reasonable approach; however, care should be taken to avoid nocturnal hypoglycemia.
î If tube feeds are interrupted and insulin has been given, an infusion of dextrose-containing fluid should be started at a rate to match the infusion rate of the scheduled tube feeds until the insulin has worn off.
• Pulmonary complications
î The etiology of pulmonary aspiration is often difficult to discern in tube-fed patients as it can occur both from refluxed tube feedings or oropharyngeal secretions unrelated to feedings. Recent evidence suggests that oral secretions play a far greater role in the development of ventilator-associated pneumonia than aspiration of tube feedings.19
î Gastric residuals are poorly predictive of aspiration risk.20
î Prevention of reflux: Decrease gastric acid secretion with H2 blockers or proton pump inhibitors, elevate head of bed during feeds, and avoid gastric feeding in high-risk patients (e.g., those with gastroparesis, frequent vomiting, gastric outlet obstruction).
• GI complications
î Nausea, vomiting, and abdominal pain are common.
î Diarrhea is often associated with antibiotic therapy and the use of liquid medications that contain nonabsorbable carbohydrates, such as sorbitol. If diarrhea from tube feeding persists after proper evaluation of possible causes, a trial of antidiarrheal agents or fiber is warranted. Diarrhea is common in patients who receive tube feeding and occurs in up to 50% of critically ill patients. Supplementation with fiber or switching to a fiber-enriched feed has not yielded consistent results. A change to an elemental feeding formula is rarely needed and likely will not resolve the issue unless significant impairment in absorption is well-documented.21
° Diarrhea in patients with short gut, who do not have other causes such as Clostridioides difficile infection, may be minimized using small, frequent meals that do not contain concentrated sweets (e.g., soda). Intestinal transit time should be maximized to optimize nutrient absorption using a tincture of opium, loperamide, or diphenoxylate. Low-dose clonidine (0.025-0.05 mg orally bid) may be used to reduce diarrhea in hemodynamically stable patients with short bowel syndrome.22 Intestinal ischemia/necrosis has been reported in patients receiving tube feeds. These cases have occurred predominantly in critically ill patients receiving vasopressors for blood pressure support in conjunction with enteral feeding. There are no reliable clinical signs for diagnosis, and the mortality rate is high. Caution should be used when enterally feeding critically ill patients requiring vasopressors.
More on the topic Diagnosis:
- Adhikari S.. Diagnosketch: A Visual Guide to Medical Diagnosis for the Non-Medical Audience Oxford: Oxford University Press,2022. — 665 p., 2022
- Diagnosis of Bovine Tuberculosis in Zambia
- Voluntary counselling and HIV testing
- Bovine Tuberculosis in Uganda
- Contents
- Contents
- Prevalence and Epidemiology of BTB in Rwanda