Dyslipidemia
GENERAL PRINCIPLES
• Lipids are sparingly soluble macromolecules that include cholesterol, fatty acids, and their derivatives.
• Plasma lipids are transported by lipoprotein particles composed of apolipoproteins, phospholipids, free cholesterol, cholesterol esters, and triglycerides.
• Human plasma lipoproteins are separated into five major classes based on density:
î Chylomicrons (least dense)
î Very-low-density lipoproteins (VLDLs)
î Intermediate-density lipoproteins (IDLs)
î Low-density lipoproteins (LDLs)
î High-density lipoproteins (HDLs)
• A sixth class, lipoprotein(a) [Lp(a)], resembles LDL in lipid composition and has a density that overlaps LDL and HDL.
• Physical properties of plasma lipoproteins are summarized in Table 3-6.
TABLE 3-6
PHYSICAL PROPERTIES OF PLASMA LIPOPROTEINSa
| Lipoprotein | Lipid Composition | Origin | Apolipoproteins |
| Chylomicrons TG, 85%; chol, 3% | Intestine | A-I, A-IV; B-48; C-I, C-II, C-III; E | |
| VLDL | TG, 55%; chol, 20% | Liver | B-100; C-I, C-II, C-III; E |
| IDL | TG, 25%; chol, 35% | Metabolic product of VLDL | B-100; C-I, C-II, C-III; E |
| LDL | TG, 5%; chol, 60% | Metabolic product of IDL | B-100 |
| HDL | TG, 5%; chol, 20% | Liver, intestine | A-I, A-II; C-I, C-II, C-III; E |
| Lp(a) | TG, 5%; chol, 60% | Liver | B-100; Apo(a) |
Chol, cholesterol; HDL, high-density lipoprotein; IDL, intermediate-density lipoprotein; LDL, low-density lipoprotein; Lp(a), lipoprotein(a); TG, triglyceride; VLDL, very-low-density lipoprotein.
aRemainder of particle is composed of phospholipid and protein.
• Nearly 90% of patients with congestive heart disease (CHD) have some form of dyslipidemia. Increased levels of LDL cholesterol (LDL-C), remnant lipoproteins, Lp(a), and decreased levels of HDL cholesterol have all been associated with an increased risk of premature vascular disease.62,63 In addition, dyslipidemia is highly prevalent in children with nonalcoholic fatty liver disease and may play a role in its pathophysiology.64
• Clinical dyslipoproteinemias
î Most dyslipidemias are multifactorial in etiology and reflect the effects of genetic influences coupled with diet, inactivity, smoking, alcohol use, and comorbid conditions such as obesity and diabetes (DM).
î Differential diagnosis of the major lipid abnormalities is summarized in Table 3-7.
TABLE 3-7
| DIFFERENTIAL DIAGNOSIS OF MAJOR LIPID ABNORMALITIES | ||
| Lipid Abnormality | Primary Disorders | Secondary Disorders |
| Hypercholesterolemia | Polygenic, familial hypercholesterolemia, familial defective apo B-100; PCSK9 gain-of-function mutation | Hypothyroidism, nephrotic syndrome, anorexia nervosa |
| Hypertriglyceridemia | Lipoprotein lipase deficiency, apo C-II deficiency, apo A-V deficiency, familial hypertriglyceridemia, dysbetalipoproteinemia | Diabetes mellitus, obesity, metabolic syndrome, alcohol use, oral estrogen, renal failure, hypothyroidism, retinoic acid, lipodystrophies |
| Combined hyperlipidemia | Familial combined hyperlipidemia, dysbetalipoproteinemia | Diabetes mellitus, obesity, metabolic syndrome, nephrotic syndrome, hypothyroidism, lipodystrophies |
| Low HDL | Familial hypoalphalipoproteinemia, Tangier disease (ABCA1 deficiency), apoA1 mutations, lecithin— cholesterol acyltransferase deficiency | Diabetes mellitus, obesity, metabolic syndrome, hypertriglyceridemia, smoking, anabolic steroids |
apo, apolipoprotein; HDL, high-density lipoprotein.
î The major genetic dyslipoproteinemias are reviewed in Table 3-8.65,66
■ Familial hypercholesterolemia (FH) and familial combined hyperlipidemia are disorders that contribute significantly to premature CVD.
TABLE 3-8
REVIEW OF MAJOR GENETIC DYSLIPOPROTEINEMIAS
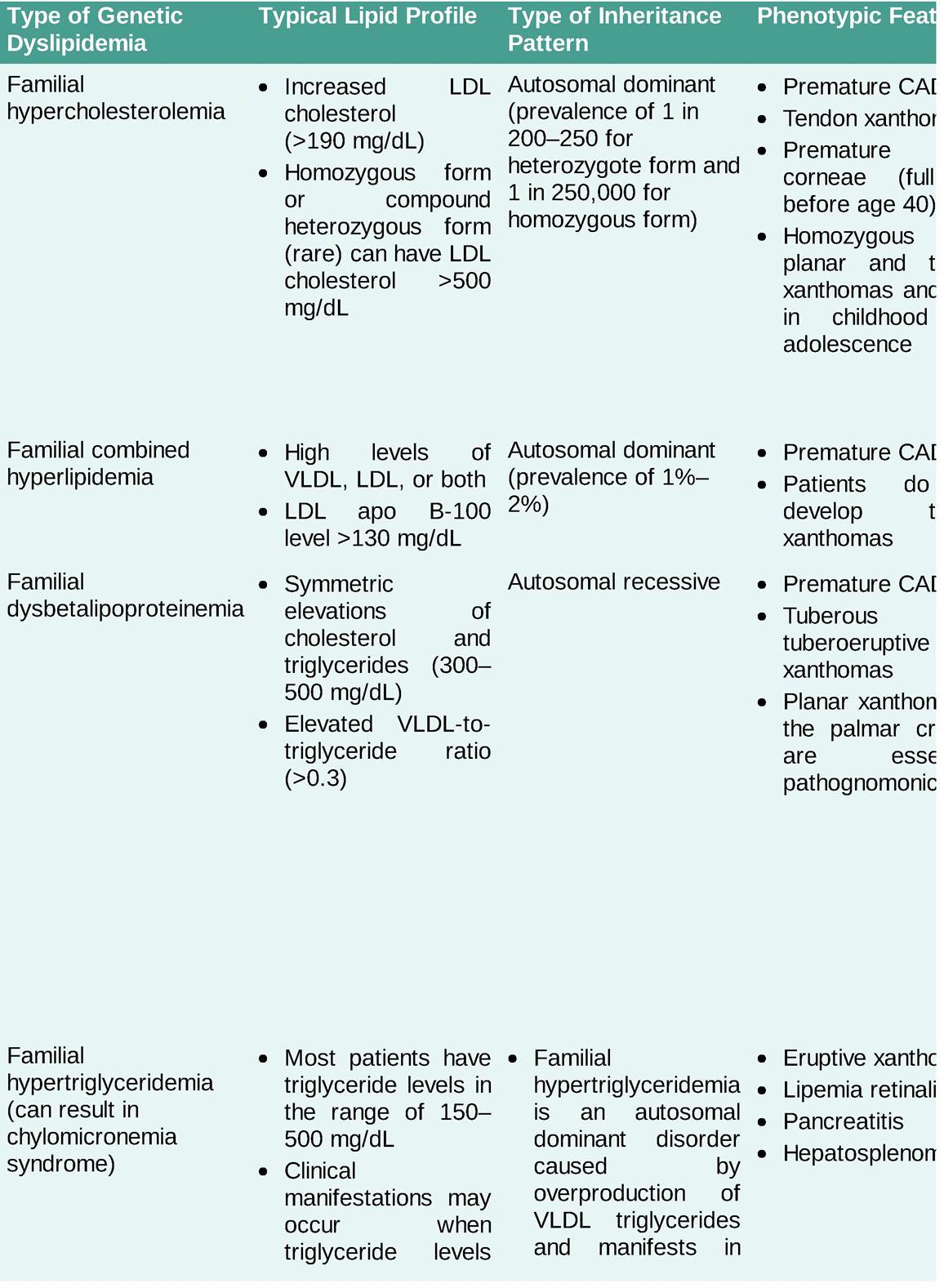
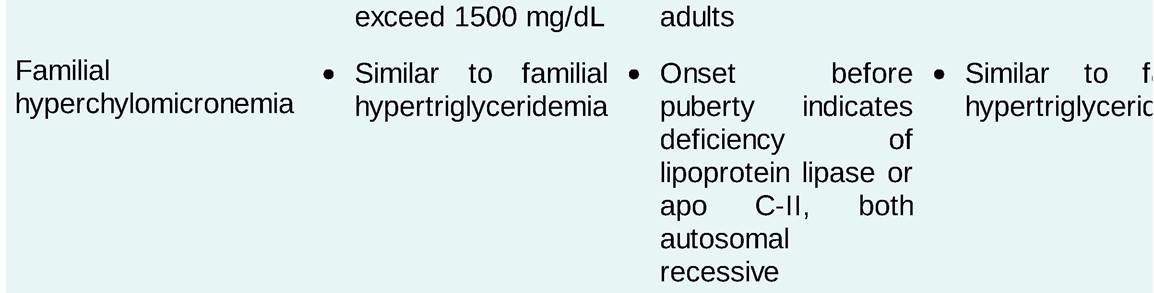
CAD, coronary artery disease; GHIHBP1, glycosylphosphatidylinositol-anchored high-density lipoprotein-binding protein 1; LDL, low-density lipoprotein; VLDL, very-low-density lipoprotein.
■ FH is an underdiagnosed, autosomal co-dominant condition with a prevalence of approximately 1 in 200 people that causes elevated LDL-C levels from birth.67,68 It is associated with significantly increased risk of early CVD.69
■ Familial combined hyperlipidemia has a prevalence of 1%-2% and typically presents in adulthood, although obesity and high dietary fat and sugar intake have led to increased presentation in childhood and adolescence.69
• Standards of care for hyperlipidemia
î LDL-C-lowering therapy, particularly with hydroxymethylglutaryl-coenzyme A (HMG-CoA) reductase inhibitors (commonly referred to as statins), lowers the risk of CHD-related death, morbidity, and revascularization procedures in patients with (secondary prevention) or without (primary prevention) known CHD.70-77 LDL-lowering therapy has proven beneficial even in patients at low risk for vascular disease.78
î Prevention of ASCVD is the primary goal of the 2018 ACC/AHA guidelines. These guidelines address risk assessment, lifestyle modifications, evaluation and treatment of obesity, and evaluation and management of blood cholesterol and aim for a more personalized and shared decision-making approach to risk management.79
Screening
• Screening for hypercholesterolemia should be done in all adults age 20 years or older.79
• Screening is best performed with a lipid profile (total cholesterol, LDL-C, HDL cholesterol, and triglycerides) obtained after a 12-hour fast.
• If a fasting lipid panel cannot be obtained, total and HDL cholesterol should be measured. Non-HDL cholesterol ≥220 mg/dL may indicate a genetic or secondary cause. A fasting lipid panel is required if non-HDL cholesterol is ≥220 mg/dL or triglycerides are ≥500 mg/dL.
• If the patient does not have an indication for LDL-lowering therapy, screening can be performed every 4-6 years between ages 40 and 75.79
• Patients hospitalized for an acute coronary syndrome or coronary revascularization should have a lipid panel obtained within 24 hours of admission if lipid levels are unknown.
• Individuals with hyperlipidemia should be evaluated for potential secondary causes, including hypothyroidism, DM, obstructive liver disease, chronic renal disease such as nephrotic syndrome, and medications such as estrogens, progestins, anabolic steroids/androgens, corticosteroids, cyclosporine, retinoids, atypical antipsychotics, and antiretrovirals (particularly protease inhibitors).
Risk Assessment
• The 2018 guidelines emphasize risk stratification based on predicted future risk, with further stratification using risk-enhancing factors to identify groups in whom the benefits of LDL-C-Iowering therapy with HMG-CoA reductase inhibitors (statins) clearly outweigh the risks and to aim for certain goals in the reduction of LDL-C. The more LDL-C is reduced, the greater the subsequent risk reduction.79 In all individuals, a heart healthy lifestyle should be encouraged as it reduces ASCVD risk at all ages.
• Areas in which treatment with statin therapy is recommended include the following:
î Patients with clinical ASCVD
î Patients with LDL-C ≥190 mg/dL
î Patients with DM age 40-75
î Patients age 40-75 with a calculated ASCVD risk ≥7.5% if a discussion of treatment options favors statin therapy
• For patients without clinical ASCVD or an LDL-C ≥190 mg/dL, the guidelines advise having a clinician-patient risk discussion before starting statin therapy.
This includes calculating a patient's risk for ASCVD based on age, sex, ethnicity, total and HDL cholesterol, SBP (treated or untreated), presence of DM, and current smoking status in addition to the presence of risk-enhancing factors.79• The ACC/AHA risk calculator is available at tools.acc.org/ASCVD-Risk-Estimator-Plus/.
î For patients of ethnicities other than African American or non-Hispanic white, risk cannot be well assessed with the risk calculator. Use of the non-Hispanic white risk calculation is suggested, with the understanding that risk may be lower than calculated in East Asian Americans and Hispanic Americans and higher in American Indians and South Asians.
î Ten-year risk should be calculated beginning at age 40 in patients without ASCVD or LDL-C ≥190 mg/dL.
î Lifetime risk may be calculated in patients age 20-39 and patients age 40-59 with a 10-year risk and multiple high-risk conditions (major ASCVD events are recent acute coronary syndrome [past 12 months], history of MI, history of ischemic stroke, symptomatic peripheral arterial disease).
î High-risk conditions include age >65 years, heterozygous FH, history of prior coronary bypass surgery or percutaneous intervention outside the major ASCVD event, DM, hypertension, CKD (eGFR 15-59 mL/min/1.73 m2), current smoking, persistently elevated LDL-C (>100 mg/dL) despite maximally tolerated statin therapy and ezetimibe, history of CHF.
î In patients with T2DM and known ASCVD, consider starting an SGLT2 inhibitor or GLP-1 RA for cardiovascular and renal benefits.82-84
• LDL-C ≥190 mg/dL
î These individuals have elevated lifetime risk because of long-term exposure to very high LDL-C levels, and the risk calculator does not account for this.
î LDL-C should be reduced with high-intensity statin therapy. If high-intensity therapy is not tolerated, maximum tolerated intensity should be used.
î If LDL-C on statin therapy remains >100 mg/dL (>2.6 mmol/L), adding ezetimibe is reasonable.
î If the LDL-C level on statin plus ezetimibe remains >100 mg/dL (>2.6 mmol/L) and the patient has multiple factors that increase subsequent risk of ASCVD event, a PCSK9 inhibitor may be considered, although the long-term safety (>3 years) is uncertain.
î LDL apheresis is an optional therapy in patients with homozygous FH and those with severe heterozygous FH with insufficient response to medication. Lomitapide, a microsomal triglyceride transfer protein inhibitor, and mipomersen, an apolipoprotein B antisense oligonucleotide, are medications indicated for the treatment of patients with homozygous FH.66
î Because hyperlipidemia of this degree is often genetically determined, discuss screening of other family members (including children) to identify candidates for treatment. In addition, screen for and treat secondary causes of hyperlipidemia.67
• Patients with diabetes, aged 40-75, LDL-C >70 mg/dL
î Moderate-intensity statin therapy is indicated regardless of estimated 10-year ASCVD risk.
î In patients with DM at higher risk, especially those with multiple risk factors or those aged 50-75, it is reasonable to use a high-intensity statin to reduce the LDL-C by >50%.
î Diabetes-specific risk enhancers: long duration (>10 years for T2DM or >20 years for T1DM), albuminuria (>30 μg of albumin/mg creatinine), eGFR 2.0 mg/L, ABI 50 mg/dL or 125 nmol/L.
î In intermediate-risk adults in whom high-intensity statins are advisable to reach goal reduction, but not acceptable or tolerated, it is reasonable to add a nonstatin drug (ezetimibe or bile acid sequestrant) to moderate-intensity statin.
• Other patient populations
î If a 10-year ASCVD risk is >7.5%-19.9% and decision about statin therapy is uncertain, consider measuring coronary artery calcium (CAC) to help identify risk. If the CAC is zero, it is reasonable to withhold statin therapy and reassess in 5-10 years, as long as higher risk conditions are absent. If CAC score is 1-99, it is reasonable to initiate statin therapy for patients >55 years. If CAC score is >100 and/or greater than 75th percentile, it is reasonable to initiate statin therapy.
î Patients with stage 3-5 CKD are high risk for ASCVD85 and the use of LDL-lowering therapy is indicated in patients with nondialysis-dependent CKD.86
î Use of statin therapy should be individualized for patients older than 75. In randomized controlled trials, patients older than 75 continued to have benefit from statin therapy, particularly for secondary prevention.73,87 In addition, many ASCVD events occur in this age group, and patients without other comorbidities may benefit substantially from cardiovascular risk reduction.
° In adults >75 years it may be reasonable to stop statin therapy when functional decline (physical or cognitive), multimorbidity, frailty, or reduced life expectancy limits the potential benefits of statin therapy.
î In adults with advanced kidney disease that requires dialysis treatment who are currently on LDL-
lowering therapy with a statin, it may be reasonable to continue the statin.
î In adults with advanced kidney disease who require dialysis treatment, initiation of a statin is not recommended.
î In patients with HF with reduced ejection fraction attributable to ischemic heart disease who have a reasonable life expectancy (3-5 years) and are not already on a statin because of ASCVD, clinicians may consider initiation of moderate-intensity statin therapy to reduce the occurrence of ASCVD events.66
• LDL-C reduction beyond statin therapy
î When statins are insufficient for LDL-C reduction, further therapy with nonstatins may be indicated. This would generally include ezetimibe, bile acid sequestrants, and PCSK9 monoclonal antibodies.88
• Hypertriglyceridemia
î Hypertriglyceridemia may be an independent cardiovascular risk factor.65,89-91
î Hypertriglyceridemia is often observed in the metabolic syndrome,91 and there are many potential etiologies for hypertriglyceridemia, including obesity, DM, renal insufficiency, genetic dyslipidemias, and therapy with oral estrogen, glucocorticoids, β-blockers, tamoxifen, cyclosporine, antiretrovirals, and retinoids.
î The classification of serum triglyceride levels is as follows: normal: acids) is the primary goal of therapy to prevent acute pancreatitis.
■ When patients have a lesser degree of hypertriglyceridemia, controlling the LDL-C level is the primary aim of initial therapy. Lifestyle changes are indicated to lower triglyceride levels.69
• Low HDL cholesterol
î Low HDL cholesterol is an independent ASCVD risk factor that is identified as a non-LDL-C risk and is included as a component of the ACC/AHA ASCVD risk scoring algorithm.92
î Etiologies of low HDL cholesterol include genetic conditions, physical inactivity, obesity, insulin resistance, DM, hypertriglyceridemia, cigarette smoking, high-carbohydrate (>60% of calories) diets, and certain medications (β-blockers, anabolic steroids/androgens, progestins). Acquired low HDL can also occur with plasma cell dyscrasias due to interference of paraproteins with the assay.93 î Because therapeutic interventions for low HDL cholesterol are of limited efficacy, the guidelines recommend considering low HDL cholesterol as a component of overall risk, rather than a specific therapeutic target.
î There are no clinical trial data showing a benefit of pharmacologic methods of elevating HDL cholesterol.
• Starting and monitoring therapy
î Before starting therapy, guidelines recommend checking alanine aminotransferase (ALT), hemoglobin A1C (if diabetes status is unknown), labs for secondary causes (if indicated), and creatine kinase (if indicated).
î Evaluate for patient characteristics that increase the risk of adverse events from statins, including impaired hepatic and renal function, history of statin intolerance, history of muscle disorders, unexplained elevations of ALT >3? the upper limit of normal, drugs affecting statin metabolism, Asian ethnicity, and age >75 years.79
î A repeat fasting lipid panel is indicated 4-12 weeks after starting therapy to assess adherence, with reassessment every 3-12 months as indicated.
î In patients without the anticipated level of LDL-C reduction based on intensity of statin therapy (≥50% for high intensity, 30%-50% for moderate intensity), assess adherence to therapy and lifestyle modifications, evaluate for intolerance, and consider secondary causes. After evaluation, if the therapeutic response is still insufficient on maximally tolerated statin therapy, it is reasonable to consider adding a nonstatin agent.88
î Creatine kinase should not be routinely checked in patients on statin therapy but is reasonable to measure in patients with muscle symptoms.
î In 2012, the FDA stated that liver enzyme tests should be performed before starting statin therapy and only as clinically indicated thereafter. The FDA concluded that serious liver injury with statins is rare and unpredictable and that routine monitoring of liver enzymes does not appear to be effective in detecting or preventing serious liver injury. Elevations of liver transaminases 2-3? the upper limit of normal are dose-dependent, may decrease on repeat testing even with continuation of statin therapy, and are reversible with discontinuation of the drug.
Treatment of Elevated LDL Cholesterol
• HMG-CoAreductase inhibitors (statins)
î Statins (see Table 3-10) are the treatment of choice for elevated LDL-C and usually lower levels by 30%-50% with moderate-intensity and ≥50% with high-intensity statin therapy79,94,95
î The lipid-lowering effect of statins appears within the first week of use and becomes stable after approximately 4 weeks of use.
î Statin therapy is effective in both men and women.96
° Common side effects (5%-10% of patients) include gastrointestinal upset (e.g., abdominal pain, diarrhea, bloating, constipation) and muscle pain or weakness, which can occur without creatine kinase elevations. Other potential side effects include malaise, fatigue, headache, and rash.95,97-99
î Myalgias are the most common cause of statin discontinuation and are often dose-dependent. They occur more often with increasing age and number of medications and decreasing renal function and body size.98-100
■ Discontinue statins in patients who develop muscle symptoms until they can be evaluated. For severe symptoms, a creatine kinase level can be measured.79
■ For mild to moderate symptoms, evaluate for conditions increasing the risk of muscle symptoms, including renal or hepatic impairment, hypothyroidism, vitamin D deficiency, rheumatologic disorders, and primary muscle disorders. Statin-induced myal gias are likely to resolve within 2 months of discontinuing the drug.
■ If symptoms resolve, the same or lower dose of the statin can be reintroduced.
■ If symptoms recur, use a low dose of a different statin and increase as tolerated.
■ If the cause of symptoms is determined to be unrelated, restart the original statin.
î Statins have been associated with an increased incidence of DM. However, the total benefit of statin use usually outweighs the potential adverse effects from an increase in blood sugar.101
° There is no aggregated evidence that statins have any negative impact on cognitive function.102
î Because a number of drug interactions are possible depending on the statin and other medications being used, drug interaction programs and package inserts should be consulted.103
î Because some statins undergo metabolism by the cytochrome P450 enzyme system, taking these statins in combination with other drugs metabolized by this enzyme system increases the risk of rhabdomyolysis.95,97,98 Among these drugs are fibrates (greater risk with gemfibrozil), itraconazole, ketoconazole, erythromycin, clarithromycin, cyclosporine, nefazodone, and protease inhibitors.98
î Statins may also interact with large quantities of grapefruit juice to increase the risk of myopathy.
î Simvastatin can increase the levels of warfarin and digoxin and has significant dose-limiting interactions with amlodipine, amiodarone, dronedarone, verapamil, diltiazem, and ranolazine. Rosuvastatin may also increase warfarin levels.
î The use of statins is contraindicated during pregnancy and lactation.
• Bile acid sequestrant resins
î Currently available bile acid sequestrant resins include the following:
■ Cholestyramine: 4-24 g/d PO in divided doses before meals.
■ Colestipol: tablets, 2-16 g/d PO; granules, 5-30 g/d PO in divided doses before meals.
■ Colesevelam: 625 mg tablets, three tablets PO bid or six tablets PO daily (maximum of seven tablets daily) with food, or one packet of oral suspension daily.
î Bile acid sequestrants typically lower LDL-C levels by 15%-30% and thereby lower the incidence of CHD.95,104
î These agents should not be used as monotherapy in patients with triglyceride levels >250 mg/dL because they can raise triglyceride levels. They may be combined with statins or nicotinic acid.
î Common side effects of resins include constipation, abdominal pain, bloating, nausea, and flatulence. î Bile acid sequestrants may decrease oral absorption of many other drugs, including warfarin, digoxin, thyroid hormone, thiazide diuretics, amiodarone, glipizide, and statins.
■ Colesevelam interacts with fewer drugs than do the older resins but can affect the absorption of thyroxine.
■ Other medications should be given at least 1 hour before or 4 hours after resins.
• Nicotinic acid (niacin)
î Niacin can lower LDL-C levels by ≥15%, lower triglyceride levels by 20%-50%, and raise HDL cholesterol levels by up to 35%.89,105 The use of niacin is limited by its side effect profile.
î Crystalline niacin is given 1-3 g/d PO in two to three divided doses with meals. Extended-release niacin is dosed at night, with a starting dose of 500 mg PO, and the dose may be titrated monthly in 500 mg increments to a maximum of 2000 mg PO (administer dose with milk, applesauce, or crackers).
î Common side effects of niacin include flushing, pruritus, headache, nausea, and bloating. Other potential side effects include elevation of liver transaminases, hyperuricemia, and hyperglycemia.
■ Flushing may be decreased with the use of aspirin 325 mg 30 minutes before the first few doses.
■ Hepatotoxicity associated with niacin is partially dose-dependent and appears to be more prevalent with some over-the-counter time-release preparations.
î Avoid use of niacin in patients with gout, liver disease, active peptic ulcer disease, and uncontrolled DM.
■ Niacin can be used with care in patients with well-controlled DM (hemoglobin A1C level ≤7%).
■ Serum transaminases, glucose, and uric acid levels should be monitored every 6-8 weeks during dose titration and then every 4 months
î The use of niacin in patients with well-controlled LDL-C levels (with statins) has not been shown to be of benefit in clinical trials.106,107 Niacin can be useful as an additional agent in patients with severely elevated LDL-C levels.
• Ezetimibe
î Ezetimibe is currently the only available cholesterol-absorption inhibitor. It appears to act at the brush border of the small intestine and inhibits cholesterol absorption.
î Ezetimibe may provide an additional 25% mean reduction in LDL-C when combined with a statin and provides an approximately 18% decrease in LDL-C when used as monotherapy.107-111
î The recommended dosing is 10 mg PO once daily. No dosage adjustment is required for renal insufficiency and mild hepatic impairment or in elderly patients. It is not recommended for use in
patients with moderate to severe hepatic impairment.
î Side effects are infrequent and include gastrointestinal symptoms (e.g., diarrhea, abdominal pain) and myalgias.
î In clinical trials, there was no excess of rhabdomyolysis or myopathy when compared with statin or placebo alone.
î Liver enzymes should be monitored when used in conjunction with fenofibrate but are not required in monotherapy or with a statin.
î A clinical outcome trial showed decreased reduction of cardiovascular events with the combination of simvastatin and ezetimibe compared with placebo in patients with chronic renal failure.112 The IMPROVE-IT trial showed a reduction in cardiovascular end points when ezetimibe was added to simvastatin in high-risk patients with already low LDL levels.113
î Ezetimibe is useful in patients with FH who do not achieve adequate LDL-C reductions with statin therapy alone.114
• Bempedoic acid
î Bempedoic acid is an inhibitor of adenosine triphosphate citrate lyase, an enzyme upstream of the target of statins (3-hydroxy-3-methylglutaryl-CoA reductase) in the cholesterol biosynthesis pathway.
î Bempedoic acid alone or in combination with a statin or ezetimibe (combination bempedoic acid- ezetimibe tablet with FDA approval is available) safely lowers LDL-C as shown in the CLEAR Harmony and CLEAR Wisdom randomized controlled trials in 2019.115,116
î In patients with gout, serum uric acid levels should be measured and stabilized prior to initiation.
• PCSK9 inhibitors
î Monoclonal antibodies have been developed that lower LDL-C. They work by inhibiting the PCSK9 enzyme, which is involved in breaking down the LDL-C receptor. Their use increases the number of available cell surface LDL receptors and subsequently remove more LDL from circulation. Major studies have shown significant reduction in LDL-C when PCSK9 inhibitors were added to statin therapy.117
î These agents have shown great ability in further reducing LDL-C in high-risk patients and are approved for use as adjuncts in patients with clinical ASCVD and heterozygous FH and as monotherapy for homozygous FH.
î Two PCSK9 inhibitors are approved for clinical use, evolocumab and alirocumab. Evolocumab is dosed at 140 mg subcutaneously every 2 weeks or 420 mg every 4 weeks. Alirocumab is dosed at 75 or 150 mg every 2 weeks or 300 mg every 4 weeks.
î Evolocumab has been shown to decrease major cardiovascular events.117 The more recent ODYSSEY OUTCOMES trial showed alirocumab significantly reduces ischemic events, all-cause mortality, and MI among patients with an acute coronary syndrome event within the preceding 1-12 months.118
• Evinacumab
î Evinacumab is a human monoclonal antibody against ANGPTL3, a angiopoietin-like protein (ANGPTLs) that regulates lipoprotein metabolism.
î A recent phase 2 trial in 2020 showed reduction in hepatic VLDL-C production and secretion and consequently lowered LDL-C when safely used in combination with a PCSK9 inhibitor and statin, with or without ezetimibe.119
Treatment of Hypertriglyceridemia
• Nonpharmacologic treatment
• Nonpharmacologic treatments are important in the therapy of hypertriglyceridemia. Approaches include
the following:
î Changing oral estrogen replacement to transdermal estrogen
î Decreasing alcohol intake
î Encouraging weight loss and exercise
î Controlling hyperglycemia in patients with DM
î Avoiding simple sugars and very-high-carbohydrate diets69,91
• Pharmacologic treatment
î Pharmacologic treatment of severe hypertriglyceridemia consists of fibric acid derivative (fibrates), niacin, or ω-3 fatty acids.
î Patients with severe hypertriglyceridemia (>1000 mg/dL) should be treated with pharmacotherapy in addition to reduction of dietary fat, alcohol, and simple carbohydrates to decrease the risk of pancreatitis.
î Statins may be effective for patients with mild to moderate hypertriglyceridemia and concomitant LDL-C elevation.69,91,120
î Fibric acid derivatives
■ Currently available fibric acid derivatives include the following (bezafibrate is not available in the United States):
? Gemfibrozil: 600 mg PO bid before meals
? Fenofibrate: available in several forms, dosage typically 48-145 mg/d PO
■ Fibrates generally lower triglyceride levels by 30%-50% and increase HDL cholesterol levels by 10%-35%. They can lower LDL-C levels by 5%-25% in patients with normal triglyceride levels but may actually increase LDL-C levels in patients with elevated triglyceride levels.120,121
■ Common side effects include dyspepsia, abdominal pain, cholelithiasis, rash, and pruritus.
■ Fibrates may potentiate the effects of warfarin.95 Gemfibrozil given in conjunction with statins may increase the risk of rhabdomyolysis.99,122-124
î ω-3 fatty acids
■ High doses of ω-3 fatty acids from fish oil can lower triglyceride levels.125,126
■ The active ingredients are eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA).
■ To lower triglyceride levels, 1-6 g of ω-3 fatty acids, either EPA alone or with DHA, is needed daily.
■ Main side effects are burping, bloating, and diarrhea.
■ Prescription forms of ω-3 fatty acids are available and are indicated for triglyceride levels >500 mg/dL. One preparation contains EPA and DHA; four tablets contain about 3.6 g of ω-3 acid ethyl esters and can lower triglyceride levels by 30%-40%. Other preparations contain only EPA or contain unesterified EPA and DHA.
■ Three recent large cardiovascular outcomes trials (ASCEND, VITAL, REDUCE-IT) showed clear benefits for ω-3 fatty acid intake for CVD, including risk reduction for heart attack, other major cardiovascular events, and death from CVD.127-130
■ Applying the results of these trials to clinical practice, the addition of 4 g/d of EPA should be considered for statin-treated patients who have CVD or diabetes plus elevated triglycerides. All adults should consume at least one to two servings of fish/seafood per week, with additional primary prevention benefits conferred by consuming 1 g/d of EPA and DHA.
■ In addition, EPA and DHA may help preserve physical function in CAD patients.131
■ The combination of ω-3 fatty acids plus a statin has the advantage of avoiding the risk of myopathy seen with statin-fibrate combinations.132,133
Treatment of Low HDL Cholesterol
• Low HDL cholesterol often occurs in the setting of hypertriglyceridemia and metabolic syndrome. Management of accompanying high LDL-C, hypertriglyceridemia, and the metabolic syndrome may result in improvement of HDL cholesterol.134
• Nonpharmacologic therapies are the mainstay of treatment, including the following:
î Smoking cessation
î Exercise
î Weight loss
• In addition, medications known to lower HDL levels, such as β-blockers (except carvedilol), progestins, and androgenic compounds, should be avoided if possible.
• No clinical outcomes trials have shown a clear benefit to pharmacologic treatment for raising HDL cholesterol.
More on the topic Dyslipidemia:
- Chronic Pancreatitis
- Antiretroviral Therapy and Metabolic Disorders
- Glucocorticoids
- Macrovascular Complications of Diabetes Mellitus
- Conclusion