Hypertension
GENERAL PRINCIPLES
Hypertension is defined as the presence of blood pressure (BP) elevation to a level that places patients at increased risk for target organ damage in several vascular beds including the retina, brain, heart, kidneys, and large conduit arteries (Table 3-1 and Table 3-2).
TABLE 3-1
MANIFESTATIONS OF TARGET ORGAN DISEASE
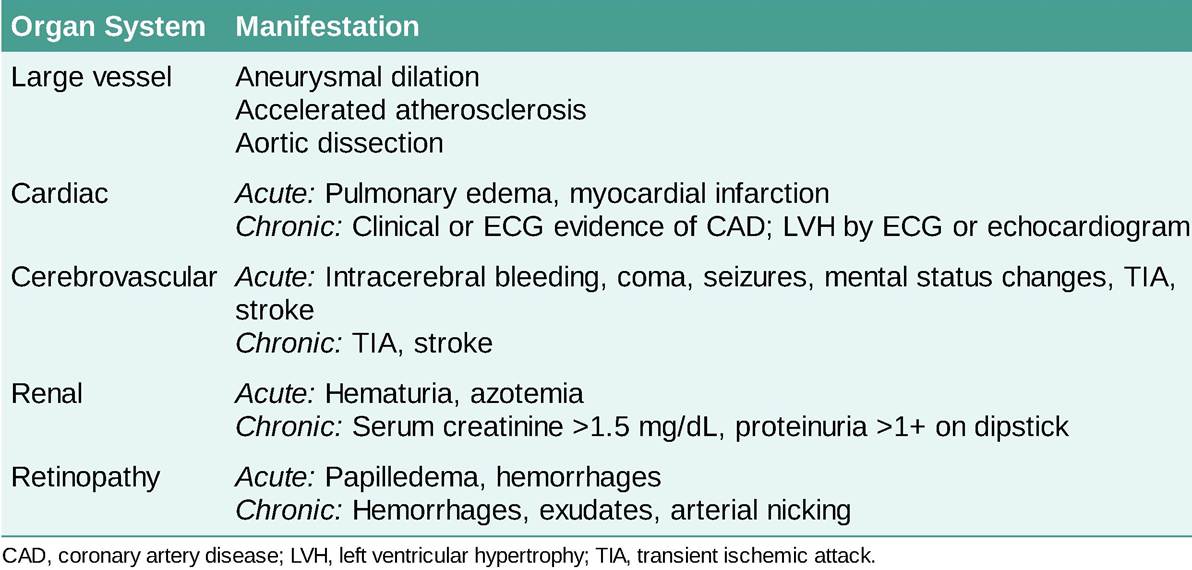
TABLE 3-2


aNot taking antihypertensive drugs and not acutely ill. When systolic and diastolic pressures fall into different categories, the higher category should be selected to classify the individual’s blood pressure status.
Data from Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2018;71:e127- e248.
Classification
• The following definitions and recommendations are based on the 2017 American College of Cardiology (ACC)ZAmerican Heart Association (AHA) guidelines. The 2018 European Society of Cardiology and European Society of Hypertension (ESCZESH) guidelines and 2019 National Institute for Health and Care Excellence (NICE) guidelines do differ, particularly in terms of treatment thresholds.1,3
• Normal BP is defined as systolic blood pressure (SBP) 3 antihypertensive agents, one of which is a diuretic, or controlled BP on >4 antihypertensive agents. All agents should be prescribed at maximally recommended (or maximally tolerated) doses.
Causes of pseudoresistance should be ruled out prior to diagnosis with resistant hypertension (inaccuracy in BP measurement, white coat hypertension, poor adherence, or poor regimen).12,13 Potential causes of resistant hypertension include ingestion of exogenous substances (e.g., decongestants, oral contraceptives, appetite suppressants, sympathomimetics, venlafaxine, tricyclic antidepressants, monoamine oxidase inhibitors [MAOIs], chlorpromazine, some herbal supplements [e.g.: ma huang], steroids, NSAIDs, cyclosporine, caffeine, thyroid hormones, cocaine, alcohol use, erythropoietin) and secondary causes of hypertension.1• White coat hypertension is defined as blood pressure that is consistently elevated by office readings but does not meet diagnostic criteria for hypertension based on out-of-office readings.
• Masked hypertension is defined as blood pressure that is consistently elevated by out-of-office measurements but does not meet the criteria for hypertension based on office readings.
Epidemiology
• The public health burden of hypertension is enormous. According to recent estimates from the National Health and Nutrition Examination Survey (NHANES) through the Centers for Disease Control and Prevention (CDC), hypertension affects an estimated 116 million American adults, up from 103 million per ACC/AHA guidelines in 2017.14,15 Of the population with hypertension, 73.9% of people with hypertension in the United States have uncontrolled hypertension. For nonhypertensive individuals aged 55-65 years, the lifetime risk of developing hypertension is 90%.16
• Data derived from the Framingham Study have shown that hypertensive patients have a fourfold increase in cerebrovascular accidents and a sixfold increase in congestive heart failure (CHF) when compared with normotensive control subjects.16
• Disease-associated morbidity and mortality, including ASCVD, stroke, heart failure (HF), and renal insufficiency, increase with higher levels of SBP and DBP.
Elevated blood pressure is the strongest modifiable risk factor for CVD worldwide.17• Over the last 3 decades, aggressive treatment of hypertension has resulted in a substantial decrease in death rates from stroke and coronary heart disease (CHD). Although the incidence of end-stage renal disease (ESRD) has stabilized and hospitalizations for CHF have overall decreased,18 BP control rates remain poor, with 53% of treated hypertensive patients having BP above target goal.15
Etiology
• BP rises with age. Other contributing factors include obesity, decreased physical activity, increased dietary sodium intake, increased alcohol consumption, and lower dietary intake of fruits, vegetables, and potassium.
• Of all hypertensive patients, more than 90% have primary or essential hypertension. The remainder have secondary hypertension due to renal parenchymal disease, renovascular disease, pheochromocytoma, Cushing syndrome, primary hyperaldosteronism, coarctation of the aorta, obstructive sleep apnea, and uncommon autosomal dominant or autosomal recessive diseases of the adrenal-renal axis, which result in salt retention.
DIAGNOSIS
Clinical Presentation
• BP elevation is usually discovered in asymptomatic individuals during routine health visits. However, appropriately measured out-of-office BP measurements should be used in complement with office readings for purposes of confirming the diagnosis of hypertension, titatring BP-lowering medication, and excluding white coat and masked hypertension.1,2,19
• Optimal detection and evaluation of hypertension require accurate noninvasive BP measurement, which should be obtained in a seated patient with the arm resting at heart level. The patient should be relaxed and sitting in the chair with their feet on the floor and back supported for more than 5 minutes prior to obtaining the blood pressure reading. They should avoid caffeine, exercise, and smoking for at least 30 minutes before measurement and should have an empty bladder.
A calibrated, appropriately fitting BP cuff (inflatable bladder encircling at least 80% of the arm) should be used because falsely high readings can be obtained if the cuff is too small. Neither the patient nor the observer should talk during measurement.• Two readings should be taken, separated by 2 minutes on two separate occasions. SBP should be noted with the appearance of Korotkoff sounds (phase I) and DBP with the disappearance of sounds (phase V).
• In certain patients, the Korotkoff sounds do not disappear but are present at 0 mm Hg. In this case, the initial muffling of Korotkoff sounds (phase IV) should be taken as the DBP. One should be careful to avoid reporting spuriously low BP readings because of an auscultatory gap, which is caused by the disappearance and reappearance of Korotkoff sounds in hypertensive patients and may account for up to a 25-mm Hg gap between true and measured SBP.
• Hypertension should be confirmed in both arms, and the higher reading should be used.
HISTORY
• History should seek to discover secondary causes of hypertension and note the presence of medications and supplements that can affect BP (see examples of substances above under “Resistant hypertension” definition).
• A diagnosis of secondary hypertension should be considered in the following situations:
î Age at onset younger than 30 years
î Onset of diastolic hypertension in persons older than 65 years
î Hypertension that is difficult to control after therapy has been initiated
î Stable hypertension that becomes difficult to control
î Resistant hypertension
î Clinical occurrence of a hypertensive emergency
î The presence of signs or symptoms of a secondary cause such as hypokalemia or metabolic alkalosis that is not explained by diuretic therapy
• In patients who present with significant hypertension at a young age, a careful family history may give clues to forms of hypertension that follow simple Mendelian inheritance.
• The 2011 ACC/AHA and 2017 ACC/AHA guidelines for peripheral vascular disease recommend diagnostic testing for renal artery stenosis in individuals with onset of hypertension at blood pressure.
• Barring an overt need for immediate pharmacologic therapy, or diagnosis of stage 2 hypertension, most patients should be given the opportunity to achieve a reduction in BP over an interval of a month by applying nonpharmacologic modifications prior to initiation of pharmacologic therapies.
Monitoring/Follow-Up
• BP measurements should be performed on multiple occasions under nonstressful circumstances (e.g., rest, sitting with legs uncrossed, empty bladder, comfortable temperature) to obtain an accurate assessment of BP in a given patient.
• Hypertension should not be diagnosed based on one measurement alone, unless it is >180/120 mm Hg or accompanied by target organ damage (i.e., hypertension urgency or emergency). Two or more abnormal readings should be obtained, preferably over a period of several weeks, before therapy is considered.
• Care should also be used to exclude pseudohypertension, which usually occurs in elderly individuals with stiff, noncompressible vessels. A palpable artery that persists after cuff inflation (Osler sign) should alert the physician to this possibility.
• Home and ambulatory BP monitoring can be used to assess a patient's true average BP, which correlates better with target organ damage.23-25
Medications
• Initial drug therapy.
• Drug interactions, cost, and coexistent factors such as age, race, angina, HF, renal insufficiency, LVH, obesity, hyperlipidemia, gout, and bronchospasm should be considered in initial drug choice. The amount of blood pressure reduction is the major determinant of reduction in cardiovascular risk, not the choice of antihypertensive drug. The BP response is usually consistent within a given class of agents; therefore, if a drug fails to control BP, another agent from the same class is unlikely to be effective. At times, however, a change within drug class may be useful in reducing adverse effects. The lowest possible effective dosage should be used to control BP, adjusted every 1-2 months as needed (Table 34).
5 mg PO daily
2.5-10
TABLE 3-4
COMMONLY USED ANTIHYPERTENSIVE AGENTS BY FUNCTIONAL CLASS
| Drugs by Class | Properties | Initial Dose | Dosage Range (mg) |
| β-Adrenergic Antagonists | |||
| Atenolola | Selective | 50 mg PO daily | 25-100 |
| Betaxolola | Selective | 10 mg PO daily | 5-40 |
| Bisoprolola | Selective | 5 mg PO daily | 2.5-20 |
| Metoprolol | Selective | 50 mg PO bid | 50-450 |
| Metoprolol XL | Selective | 50-100 mg PO daily | 50-400 |
| Nebivolola | Selective with vasodilatory properties | 5 mg PO daily | 5-40 |
| Nadolola | Nonselective | 40 mg PO daily | 20-240 |
| Propranolol | Nonselective | 40 mg PO bid | 40-240 |
| Propranolol LA | Nonselective | 80 mg PO daily | 60-240 |
| Timolol | Nonselective | 10 mg PO bid | 20-40 |
| Pindolol | ISA | 5 mg PO daily | 10-60 |
| Labetalol | α- and β-antagonist properties | 100 mg PO bid | 200-1200 |
| Carvedilol | α- and β-antagonist properties | 6.25 mg PO bid | 12.5-50 |
| Carvedilol CR | α- and β-antagonist properties | 10 mg PO daily | 10-80 |
| Acebutolola | ISA, selective | 200 mg PO bid, 400 mg PO daily | 200-1200 |
Calcium Channel Antagonists
Amlodipine DHP
| Diltiazem | 30 mg PO qid | 90-360 | |
| Diltiazem LA | 180 mg PO daily | 120-540 | |
| Diltiazem CD | 180 mg PO daily | 120-480 | |
| Diltiazem XR | 180 mg PO daily | 120-540 | |
| Diltiazem XT | 180 mg PO daily | 120-480 | |
| Isradipine | DHP | 2.5 mg PO bid | 2.5-10 |
| Nicardipine | DHP | 20 mg PO tid | 60-120 |
| Nifedipine | DHP | 10 mg PO tid | 30-120 |
| Nifedipine XL (or CC) | DHP | 30 mg PO daily | 30-90 |
| Nisoldipine | DHP | 20 mg PO daily | 20-40 |
| Verapamil | 80 mg PO tid | 80-480 | |
| Verapamil SR | 120 mg PO daily | 120-480 | |
| Angiotensin-Converting Enzyme Inhibitorsc | |||
| Benazepril | 10 mg PO bid | 10-40 | |
| Captopril | 25 mg PO bid-tid | 12.5-450 | |
| Enalapril | 5 mg PO daily | 2.5-40 | |
| Fosinopril | 10 mg PO daily | 10-40 | |
| Lisinopril | 10 mg PO daily | 5-40 | |
| Moexipril | 7.5 mg PO daily | 7.5-30 | |
| Quinapril | 10 mg PO daily | 5-80 | |
| Ramipril | 2.5 mg PO daily | 1.25-20 | |
| Trandolapril | 1-2 mg PO daily | 1-4 | |
| Perindopril | 4 mg PO daily | 2-16 | |
| Angiotensin II Receptor Blockersc | |||
| Azilsartanb | bgcolor=white>40 mg PO daily | 40-80 | |
| Candesartan | 8 mg PO daily | 8-32 | |
| Eprosartan | 600 mg PO daily | 600-800 | |
| Irbesartan | 150 mg PO daily | 150-300 | |
| Olmesartan | 20 mg PO daily | 20-40 | |
| Losartan | 50 mg PO daily | 25-100 | |
| Telmisartan | 40 mg PO daily | 20-80 | |
| Valsartan | 80 mg PO daily | 80-320 | |
| Direct Renin Inhibitorc | |||
| Aliskiren | 150 mg PO daily | 150-300 | |
| Angiotensin Receptor-Neprilysin Inhibitorc | |||
| SacubitrilZvalsartanb | 24Z26 mg PO BID | 24Z26-97Z103 | |
| Diureticsc | |||
| Chlorthalidone | Thiazide diuretic | 25 mg PO daily | 12.5-50 |
| Hydrochlorothiazide | Thiazide diuretic | 12.5 mg PO daily | 12.5-50 |
| Hydroflumethiazideb | Thiazide diuretic | 50 mg PO daily | 50-100 |
| Indapamide | Thiazide diuretic | 1.25 mg PO daily | 2.5-5 |
| Methyclothiazide | Thiazide diuretic | 2.5 mg PO daily | 2.5-5 |
| Metolazone | Thiazide diuretic | 2.5 mg PO daily | 1.25-5 |
| Bumetanide | Loop diuretic | 0.5 mg PO daily (or IV) | 0.5-5 |
| Ethacrynic acid | Loop diuretic | 50 mg PO daily (or IV) | 25-100 |
| Furosemide | Loop diuretic | 20 mg PO daily (or IV) | 20-320 |
| Torsemide | Loop diuretic | 5 mg PO daily (or IV) | 5-10 |
| Amiloride | Potassium-sparing diuretic | 5 mg PO daily | 5-10 |
| Triamterene | Potassium-sparing diuretic | 50 mg PO bid | 50-200 |
| Eplerenone | Aldosterone antagonist | 25 mg PO daily | 25-100 |
| Spironolactone | Aldosterone antagonist | 25 mg PO daily | 25-100 |
| α-Adrenergic Antagonists | |||
| Doxazosin | 1 mg PO daily | 1-16 | |
| Prazosin | 1 mg PO bid-tid | 1-20 | |
| Terazosin | 1 mg PO at bedtime | 1-20 | |
| Centrally Acting Adrenergic Agents | |||
| Clonidine | 0.1 mg PO bid | 0.1-1.2 | |
| Clonidine patch | TTS 1Zwk (equivalent to 0.1 mgZd release) | 0.1-0.3 | |
| Guanfacine | 1 mg PO daily | 1-3 | |
| Guanabenz | 4 mg PO bid | 4-64 |
| Methyldopaa | 250 mg PO bid-tid | 250-2000 |
| Direct-Acting Vasodilators | ||
| Hydralazinea | 10 mg PO qid | 50-300 |
| Minoxidil | 5 mg PO daily | 2.5-100 |
| Miscellaneous | ||
| Reserpine | 0.5 mg PO daily | 0.1-0.25 |
DHP, dihydropyridine; ISA, intrinsic sympathomimetic activity; TTS, transdermal therapeutic system.
aAdjusted in renal failure.
bAvailable only in brand name. Assume all drugs are available in generic form unless otherwise denoted by superscript “b." cRenal function should be considered before initiation.
• Thiazide or thiazide-like diuretics, calcium channel blockers (CCBs), angiotensin-converting enzyme (ACE) inhibitors, and angiotensin receptor blockers (ARBs) should be considered as first-line therapy for the general population (except for those from African descent), including those with diabetes. Multiple large randomized controlled trials have shown comparable effects on decreasing overall cardiovascular and cerebrovascular mortality for all four drug classes.5
• In patients from African descent, including those with diabetes, a thiazide or thiazide-like diuretic or CCB can be considered for first-line therapy. Data from the ALLHAT trial have shown decreased cardiovascular and cerebrovascular morbidity and mortality with the use of thiazide diuretics or CCB over an ACE inhibitor.26
• In patients with chronic kidney disease (CKD) stage 3 or higher, or CKD with albuminuria (>300 mg/d), initial or combination therapy with an ACE inhibitor or ARB is recommended.1
• Additional therapy: When a second drug is needed, it should generally be chosen from among the other first-line agents.
• Adjustments of a therapeutic regimen: Before considering a modification of therapy because of inadequate response to the current regimen, other possible contributing factors should be investigated. Poor patient compliance, use of antagonistic drugs (examples provided above), inappropriately high sodium intake, or increased alcohol consumption may be the cause of inadequate BP response. Secondary causes of hypertension should be considered when a previously effective regimen becomes inadequate and other confounding factors are absent.
• Diuretics (see Table 3-4) are effective agents in the therapy of hypertension and have been shown to reduce the incidence of stroke and cardiovascular events. Several classes of diuretics are available, generally categorized by their site of action in the kidney.
î Thiazides and thiazide-like diuretics (e.g., hydrochlorothiazide, chlorthalidone) block sodium reabsorption predominantly in the distal convoluted tubule by inhibition of the thiazide-sensitive sodium/chloride (Na/Cl) cotransporter. Thiazide diuretics can cause weakness, muscle cramps, and impotence. Metabolic side effects include hypokalemia, hypomagnesemia, hyperlipidemia (increased in low-density lipoproteins [LDLs] and triglyceride levels), hypercalcemia, hyperglycemia, hyperuricemia, hyponatremia, and rarely azotemia. Thiazide-induced pancreatitis has also been reported. Metabolic side effects may be limited when thiazides are used in low doses (e.g., hydrochlorothiazide, 12.5-25 mg/d). Chlorthalidone and indapamide, thiazide-like diuretics, are often the preferred diuretics for management of hypertension due to their longer duration of action. Thiazide-like diuretics are particularly useful in patients with osteoporosis, edema, and calcium nephrolithiasis with hypercalcemia. It should be noted that chlorthalidone is associated with greater risks of hypokalemia, glucose intolerance, and new-onset diabetes than hydrochlorothiazide.27
î Loop diuretics (e.g., furosemide, bumetanide, ethacrynic acid, torsemide) block sodium reabsorption in the thick ascending limb of the loop of Henle through inhibition of the Na∕K∕2Cl cotransporter and are the most effective agents in patients with renal insufficiency (estimated glomerular filtration rate [GFR] function (eGFR 400 mg/d), those with impaired renal or cardiac function, and those with the slow acetylation phenotype. Hydralazine should be discontinued if clinical evidence of a lupus-like syndrome develops and a positive ANA test result is present. The syndrome usually resolves with discontinuation of the drug, leaving no adverse long-term effects.
î Side effects of minoxidil include weight gain, hypertrichosis, hirsutism, ECG abnormalities, and pericardial effusions.
• Reserpine, guanethidine, and guanadrel (see Table 3-4) were among the first effective antihypertensive agents available. Currently, these drugs are not regarded as first- or second-line therapy because of their significant side effects. Side effects of reserpine include severe depression in approximately 2% of patients. Sedation and nasal stuffiness also are potential side effects. Guanethidine can cause severe postural hypotension through a decrease in cardiac output, a decrease in peripheral resistance, and venous pooling in the extremities. Patients who are receiving guanethidine with orthostatic hypotension should be cautioned to arise slowly and to wear support hose. Guanethidine can also cause ejaculatory failure and diarrhea.
• Parenteral antihypertensive agents are indicated for the immediate reduction of BP in patients with hypertensive emergencies. Judicious administration of these agents (Table 3-5) may also be appropriate in patients with hypertension complicated by HF or MI. These drugs are also indicated for individuals who have perioperative severe hypertension or need an emergency surgery. If possible, an accurate baseline BP should be determined before the initiation of therapy. In the setting of hypertensive emergency, the patient should be admitted to an intensive care unit for close monitoring, and an intra-arterial monitor should be used when available. Although parenteral agents are indicated as a first-line treatment in hypertensive emergencies, oral agents may also be effective in this group; the choice of drug and route of administration must be individualized. If parenteral agents are used initially, oral medications should be administered shortly thereafter to facilitate rapid weaning from parenteral therapy.
î Sodium nitroprusside, a direct-acting arterial and venous vasodilator, is the drug of choice for most hypertensive emergencies (see Table 3-5). It reduces BP rapidly and is easily titratable, and its action is short lived when discontinued. Patients should be monitored very closely to avoid an exaggerated hypotensive response. Therapy for more than 48-72 hours with a high cumulative dose or renal insufficiency may cause accumulation of thiocyanate, a toxic metabolite. Thiocyanate toxicity may cause paresthesias, tinnitus, blurred vision, delirium, or seizures. Serum thiocyanate levels should be kept at 2-3 μg∕kg∕min) or those with renal dysfunction should have serum levels of thiocyanate drawn after 48-72 hours of therapy. In patients with normal renal function or those receiving lower doses, levels can be drawn after 5-7 days. Hepatic dysfunction may result in accumulation of cyanide, which can cause lactic acidosis, dyspnea, vomiting, dizziness, ataxia, and syncope. Hemodialysis should be considered for thiocyanate poisoning. Nitrites and thiosulfate can be administered intravenously for cyanide poisoning.
TABLE 3-5
PARENTERAL ANTIHYPERTENSIVE DRUG PREPARATIONS
| Drug | Administration | Onset | Duration of Action | Dosage | Adverse Effects and Comments |
| Fenoldopam | IV infusion | irritation. Nicardipine should be administered via a central venous line. If it is given peripherally, the IV site should be changed q12h. Fifty percent of the peak effect is seen within the first 30 minutes, but the full peak effect is not achieved until after 48 hours of administration. Clevidipine, an IV calcium channel antagonist, has a quicker onset of action and shorter half-life than nicardipine. î Enalaprilat is the active de-esterified form of enalapril (see Table 3-5) that results from hepatic conversion after an oral dose. Enalaprilat (as well as other ACE inhibitors) has been used effectively in cases of severe and malignant hypertension. However, variable and unpredictable results have also been reported. ACE inhibition can cause rapid BP reduction in hypertensive patients with high renin states such as renovascular hypertension, concomitant use of vasodilators, and scleroderma renal crisis; thus, enalaprilat should be used cautiously to avoid precipitating hypotension. Therapy can be changed to an oral preparation when IV therapy is no longer necessary. î Diazoxide and hydralazine are only rarely used in hypertensive crises and offer little or no advantage to the agents discussed previously. It should be noted, however, that hydralazine is a useful agent in pregnancy-related hypertensive emergencies because of its established safety profile. ° Fenoldopam is a selective agonist to peripheral dopamine-1 receptors, and it produces vasodilation, increases renal perfusion, and enhances natriuresis. Fenoldopam has a short duration of action; the elimination half-life is class. In the presence of proteinuria, ACE inhibitors/ARBs should be considered because higher urinary excretion of protein is associated with a more rapid decline in GFR, regardless of the cause of renal insufficiency. More recently, an updated Kidney Disease Improving Global Outcomes BP guideline recommended more intensive BP control with a systolic target of commonly associated with centrally acting adrenergic agents (particularly clonidine) and β-adrenergic antagonists but has been reported with other agents as well, including diuretics. Discontinuation of antihypertensive medications should be done with caution in patients with preexisting cerebrovascular or cardiac disease. Management of AWS by reinstitution of the previously administered drug is generally effective.
More medical literature on Medic.Studio
More on the topic Hypertension:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|