Fluid Management and Perturbations in Volume Status
• Total body water (TBW): Water comprises approximately 60% of lean body weight in men and 50% in women. Two-thirds of TBW is intracellular fluid (ICF) and one-third is extracellular fluid (ECF).
ECF is further subdivided into intravascular and interstitial spaces in a ratio of 1:4.Example: For a healthy 70-kg man:
TBW= 0.6? 70 = 42 L
■ ICF = 2/3 TBW = 0.66 ? 42 = 28 L
■ ECF = 1/3 TBW = 0.33 ? 42 =14 L
■ Intravascular compartment = 0.25 ? 14 = 3.5 L
■ Interstitial compartment = 0.75 ? 14 = 10.5 L
The distribution of water between intravascular and interstitial spaces can be affected by changes to the Starling balance of forces. Low oncotic pressure (i.e., low albumin states) and high hydrostatic pressure (i.e., Na+-retentive states) increase the movement of fluid from vascular to interstitial compartments, which is an important step in the development of edema.
• Total body Na+ : 85%-90% of total body Na+ is extracellular and constitutes the predominate solute in the ECF. Changes to the body's total Na+ content typically results from a loss or gain of this Na+-rich fluid, leading to contraction or expansion of the ECF space.
The Euvolemic Patient
• In a euvolemic patient, the goal of fluid and electrolyte administration is to maintain homeostasis. The best way to accomplish this is to allow free access to food and oral fluids. Patients who are unable to tolerate oral intake require maintenance fluids to replace renal, gastrointestinal (GI), and insensible fluid losses.
• The decision to provide maintenance IV fluid should be thoughtfully considered and not administered by route. Fluid administration should be reassessed at least daily. Patient weight, which may indicate net fluid balance, should be monitored carefully.
• Table 12-1 provides a list of common IV solutions and their contents.
By combining the necessary components, one can derive an appropriate maintenance fluid regimen tailored for each patient.TABLE 12-1
COMMONLY USED PARENTERAL SOLUTIONS
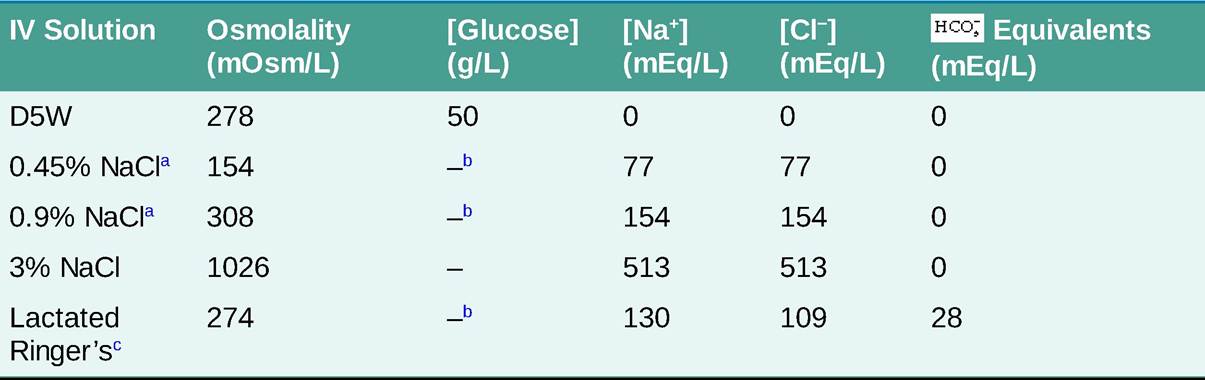
aNaCl 0.45% and 0.9% are half-normal and normal saline, respectively. bAlso available with 5% dextrose.
cAlso contains 4 mEq/L K+, 1.5 mEq/L Ca2+, and 28 mEq/L lactate. D5W, 5% dextrose in water.
The Hypovolemic Patient
GENERAL PRINCIPLES
Vblume depletion generally results from a deficit in total body Na+ content. Renal causes of Na+ loss include diuresis, salt-wasting nephropathies, and mineralocorticoid deficiency. Extrarenal causes include losses from the GI and respiratory tracts, hemorrhage, and severe third spacing of fluid in critically ill patients.
DIAGNOSIS
Clinical Presentation
Mild degrees of volume depletion are often not clinically detectable, whereas larger fluid losses can lead to fatigue, muscle cramps, and postural dizziness. Severe volume depletion can result in mental status changes, oliguria, and hypovolemic shock.
Diagnostic Testing
The following laboratory studies are consistent with volume depletion but are not required for the diagnosis:
• Urine Na+ Potassium-sparing diuretics have a comparatively small effect but are useful as adjunctive agents.
• Treatment of the underlying disease process is critical to prevent continued Na+ reabsorption in the kidney. Nephrotic syndrome is discussed in Chapter 13, Renal Diseases. Treatment of heart failure is discussed in Chapter 5, Heart Failure and Cardiomyopathy; and cirrhosis is addressed in Chapter 19, Liver Diseases.
More on the topic Fluid Management and Perturbations in Volume Status:
- Fluid Management and Perturbations in Volume Status
- WATER HOMEOSTASIS
- Volume Conduction
- Fluid and electrolyte composition of body is in a state of dynamic balance, regulated by various inter-related mechanisms.
- Contributors to Volume iii
- PARENTERAL FLUID THERAPY
- Contributors to Volume iv
- DISSEMINATED INTRAVASCULAR COAGULATION
- STATUS
- Disseminated Intravascular Coagulation