Hepatitis B Virus
GENERAL PRINCIPLES
• The US is considered an area of low prevalence for the infection. Eight genotypes of HBV have been identified (A through H). The prevalence of HBV genotypes varies depending on the geographic location.
Genotypes A, B, and C are the most prevalent in the US.• Modes of transmission include vertical (mother to infant) and horizontal (person to person) via the following routes: parenteral or percutaneous (e.g., injection drug use, needlestick injuries), direct contact with the blood or open sores of an infected person, and sexual contact with an infected individual.
• The rate of progression from acute to chronic HBV is approximately 90% for a perinatal-acquired infection, 20%-50% for infections acquired between the age of 1 and 5 years, and lt;5% for an adult- acquired infection.
Diagnosis
Clinical Presentation
• Four different clinical phases of chronic hepatitis B have been defined (Table 19-3). Most patients fit into one of the following phases:
î Immune tolerant
TABLE 19-3
USE OF HEPATITIS B VIRUS (HBV) MARKERS IN CLINICAL PRACTICE
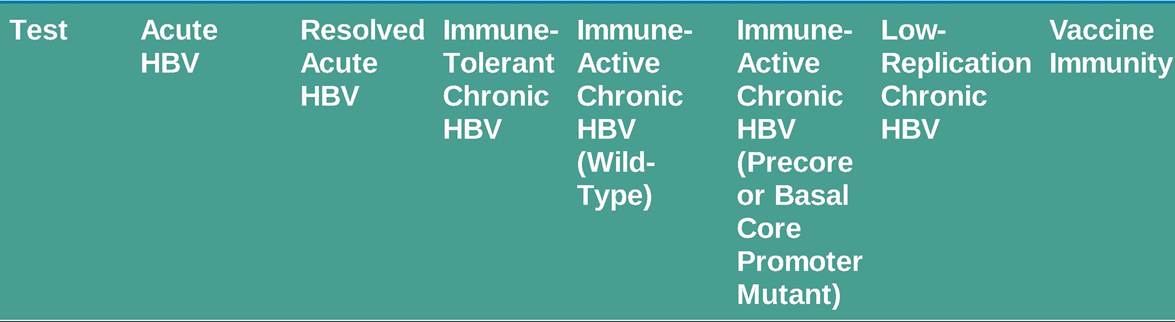
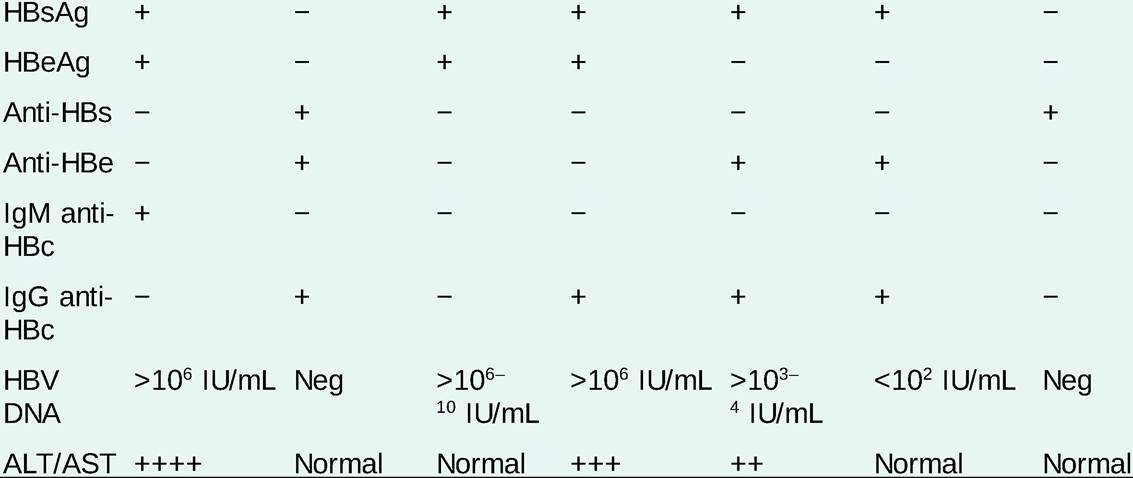
ALT, alanine aminotransferase; AST, aspartate aminotransferase; HBc, hepatitis B core antigen; HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; Neg, negative.
° Immune active (hepatitis B envelope antigen [HBeAg] positive)
î Inactive phase
î Immune reactivation phase (HBeAg negative)
• Extrahepatic manifestations include polyarteritis nodosa, glomerulonephritis, cryoglobulinemia, serum sickness-like illness, membranous nephropathy, membranoproliferative glomerulonephritis, and papular acrodermatitis (predominantly in children).
Diagnostic Testing
• HBV antigens (hepatitis B surface antigen [HBsAg] and HBeAg) are identified in the serum.
• HBV DNA is the most accurate marker of viral replication. It is detected by polymerase chain reaction (PCR).
• For use of HBV markers in clinical practice, see Table 19-3.
• Liver biopsy is useful to assess the degree of inflammation (grade) and fibrosis (stage) as well as other potential histologic abnormalities in patients with chronic hepatitis. Liver histology is an important adjuvant diagnostic test in guiding treatment decisions.
TREATMENT
The goal of treatment is viral eradication or suppression to prevent progression to ESLD and HCC. End points of treatment include the following (see Table 19-4):
TABLE 19-4
AASLD TREATMENT GUIDELINES FOR CHRONIC HEPATITIS B

12 mo.
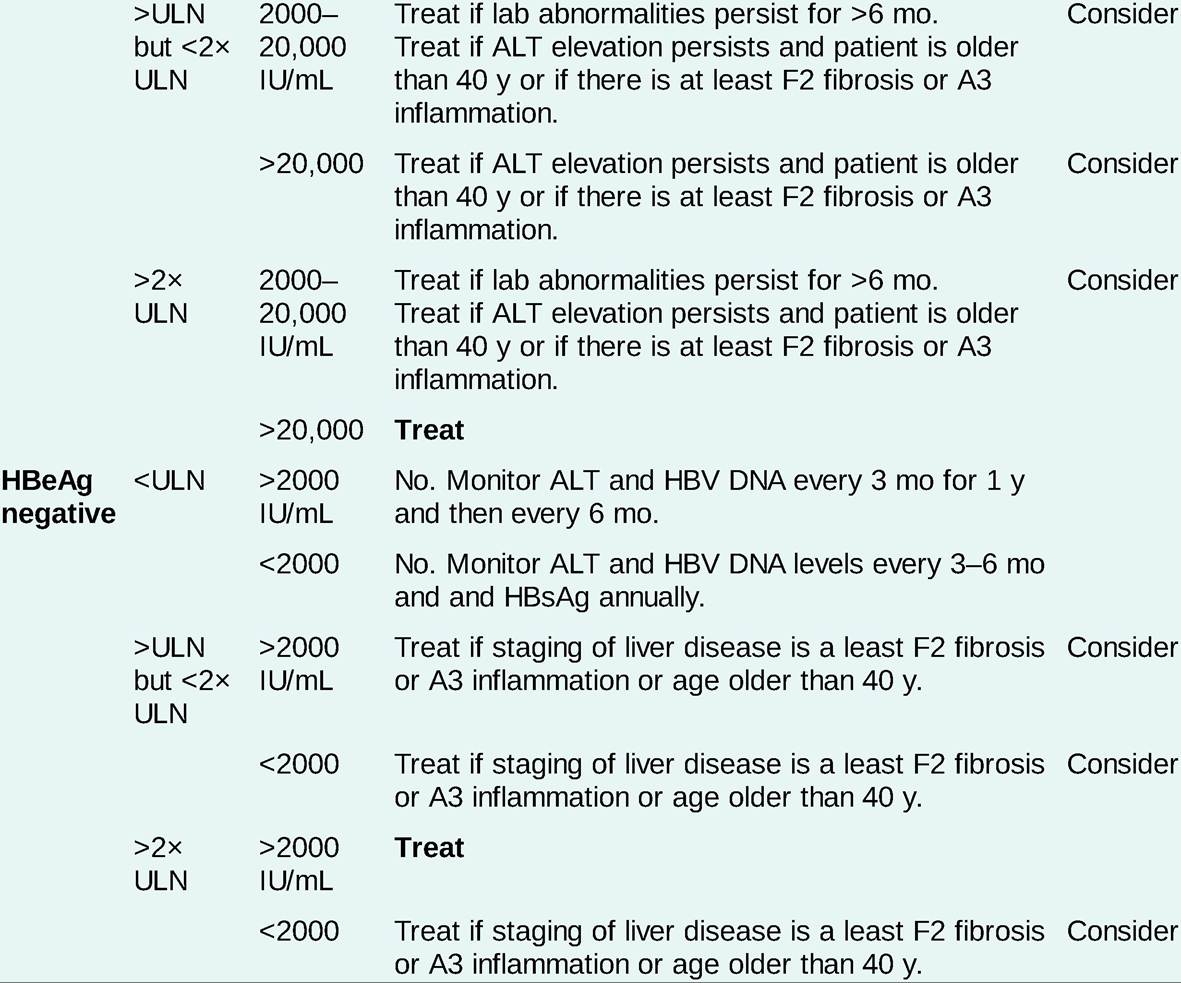
AASLD, American Association for the Study of Liver Diseases; ALT, alanine aminotransferase; HBeAg, hepatitis B e antigen; HBV, hepatitis B virus; ULN, upper limit of normal (ULN for AASLD: 35 units/L for males, 25 units/L for females).
aBiopsy indicated for patients older than 40 years, ALT persistently 1-2? ULN, and family history of hepatocellular carcinoma. Alternative methods of noninvasive fibrosis testing may be used.
• Normalization of serum ALT.
• Maintained suppression of serum HBV DNA levels to undetectable levels.
• HBeAg clearance and seroconversion to antibody anti-HBe.
• HBsAg clearance and seroconversion to antibody anti-HBs.
• Improvement in liver histology.
Medications
Medications for the treatment of hepatitis B are divided into three main groups: nucleoside analogs (entecavir, lamivudine [LAM], telbivudine), nucleotide analogs (tenofovir, adefovir), and the interferons (IFNs). Current practices recommend entecavir, tenofovir, and IFN.
• Entecavir is a potent anti-HBV oral nucleoside (guanosine) analog and is well tolerated. The dose is 0.5-1.0 mg daily in naive and LAM-resistant patients.
Entecavir has a high genetic barrier for resistance (1.2%) over several years. However, in patients resistant to LAM, the resistance to entecavir could be as high as 40%. In patients with renal impairment, dose adjustment is needed. Entecavir is pregnancy category C.• Tenofovir disoproxil fumarate (TDF) is a potent anti-HBV oral nucleotide (acyclic) analog and is well tolerated. The dose is 300 mg daily. Tenofovir has a high genetic barrier for resistance; no clinical resistance has been identified thus far. It is rarely reported to induce renal failure and Fanconi syndrome and may also lead to decreased bone density. Tenofovir is pregnancy category B.
• Tenofovir alafenamide (TAF) is preferred over TDF for patients with renal or bone disease and appears to have comparable efficacy with TDF. Consider TAF for patients with GFR lt; 60, chronic steroid use, osteoporosis, or history of fragility fractures. For patients who cannot tolerate TDF and who have previously been exposed to LAM, switching to TAF is preferred over switching to entecavir.
• Pegylated IFNs (#945;2a and #945;2b, in their pegylated form) are antiviral, immunomodulatory, and antiproliferative glycoproteins that have been used in the treatment of chronic HBV for several years. IFNs are parenteral agents and associated with a poor tolerability profile, especially in patients with advanced liver disease. Long-term studies have shown a durable benefit in responders. Neither IFN nor pegylated IFN-#945; induces antiviral resistance. The IFNs are pregnancy category C.
Prevention
• Preexposure prophylaxis
î Consider HBV vaccination in all patients, especially those from high-risk groups. HBV vaccines are made of inactivated viruses and are safe for immunocompromised patients.
î The vaccination schedule is three IM injections at 0, 1, and 6 months in infants or healthy adults. Protective antibody response (anti-HBs positive) is achieved in gt;90% after the third dose.
• Postexposure prophylaxis
î HBV positive mothers with viral load gt;200,000 should start antiviral therapy in the third trimester to decrease the risk of transmission.
î Infants born to HBsAg-positive mothers should receive HBV vaccine and hepatitis B immunoglobulin (HBIg), 0.5 mL, within 12 hours of birth. Immunized infants should be tested at approximately 12 months of age for HBsAg, anti-HBs, and anti-HBc.
î Persons who are unvaccinated or do not demonstrate anti-HBs, and have had sexual contact or needlestick with an individual with HBV, should receive HBIg (0.04-0.07 mL/kg) and the first dose of HBV vaccine at different sites. This should be done as soon as possible, preferably within 48 hours, but no more than 7 days after exposure. A second dose of HBIg should be administered 30 days after exposure, and the vaccination series should be completed.
î Persons who have received all three doses of a hepatitis B vaccination series and have confirmed anti-HBs positivity require no further treatment.
î Postexposure prophylaxis with HBIg plus a nucleotide or nucleoside analog should be used initially after liver transplantation to prevent HBV recurrence in certain patients.
Outcome and Prognosis
Chronic hepatitis B
• Morbidity and mortality in chronic HBV are linked to the level and persistence of viral replication. Spontaneous clearance of HBsAg occurs in 0.5% of patients annually.
• For HCV/HBV-coinfected individuals, there is a risk of HBV reactivation during HCV treatment with direct-acting antivirals (DAAs).
• Once the diagnosis of chronic HBV is established, the 5-year cumulative incidence of developing cirrhosis ranges from 8% to 20%.
• About 5%-10% cases of chronic HBV progress to HCC regardless of preceding cirrhosis.
More on the topic Hepatitis B Virus:
- Vasculitic Syndromes
- Polyarteritis Nodosa
- Disinfection
- Macrovascular Complications of Diabetes Mellitus
- Introduction
- Inflammatory Bowel Disease
- Conclusion
- Antiretroviral Therapy Today
- Sexually Transmitted Diseases
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025