Shock
GENERAL PRINCIPLES
• A process in which blood flow and oxygen delivery to tissues are deranged, leading to tissue hypoxia and resultant compromise of cellular metabolic activity and organ function.
• Main goal of therapy is rapid cardiovascular resuscitation to reestablish tissue perfusion.
• Definitive treatment requires reversal of underlying processes.
Classifications of Shock
Hemodynamic patterns associated with the different shock states are listed in Table 8-5.
TABLE 8-5
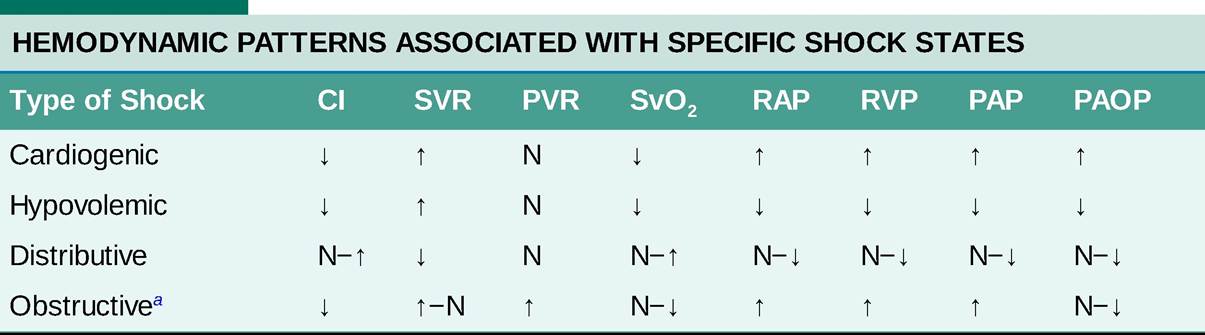
aEqualization of RAP, PAOP, diastolic PAP, and diastolic RVP establishes a diagnosis of cardiac tamponade.
CI, cardiac index; N, normal; PAOP, pulmonary artery occlusion pressure; PAP, pulmonary artery pressure; PVR, pulmonary vascular resistance; RAP, right atrial pressure; RVP, right ventricular pressure; SvO2, mixed venous oxygen saturation; SVR, systemic vascular resistance.
• Distributive: Shock caused by massive vasodilation and impaired distribution of blood flow, resulting in tissue hypoxia. Usually associated with hyperdynamic cardiac function, unless cardiac function is somehow impaired (see later discussion of cardiogenic shock).
î Primary etiologies are septic shock and anaphylactic shock. Septic shock is most commonly seen in medical ICUs and will be further discussed in the next section. Anaphylaxis is discussed in Chapter 11, Allergy and Immunology. Other less common types include neurogenic shock and adrenal shock.
° Hemodynamic parameters will generally demonstrate increased cardiac output (CO), decreased systemic vascular resistance (SVR) due to vasodilation, and elevated central venous oxygen saturation (ScvO2) due to ineffective oxygen extraction by tissue.
î Primary goals of therapy
■ Vblume resuscitation: Owing to massive peripheral vasodilation, patients have a functionally decreased oxygen-carrying capacity, requiring volume resuscitation.
IV crystalloid fluids are primarily used.■ Treatment of underlying infection: Inadequate initial antimicrobial therapy is an independent risk factor for in-hospital mortality in patients with septic shock, so timely, effective antimicrobial therapy is a cornerstone of treatment.
■ Removal of the offending agent in anaphylactic shock.
■ Cardiovascular support with vasoactive agents (e.g., norepinephrine). Vasoactive agents will be discussed in more detail in a later section.
• Hypovolemic: Shock caused by a decrease in effective intravascular volume and decreased oxygencarrying capacity.
o Primary etiologies are hemorrhagic (e.g., trauma, gastrointestinal bleeding) or fluid depletion (e.g., diarrhea, vomiting).
î Hemodynamic parameters will generally demonstrate a decreased CO, increased SVR, and decreased ScvO2 due to increased oxygen extraction by peripheral tissue.
î Primary goals of therapy
■ Volume resuscitation: IV blood product and crystalloid are used for resuscitation of hemorrhagic and fluid depletion shock, respectively, with goal mean arterial pressure (MAP) of 60-65 mm Hg. Overresuscitation may be detrimental in hemorrhagic shock and patients without significant comorbidities may tolerate lower hemoglobin levels (7 g/dL) than previously believed.
■ Definitive treatment of underlying etiology of volume loss: For hemorrhagic shock, surgical intervention may be necessary.
• Obstructive: Shock caused by obstruction of the heart or great vessels, resulting in decreased left ventricular filling and cardiovascular collapse.
î Primary etiologies are pulmonary embolism, cardiac tamponade, and tension pneumothorax.
î Hemodynamic parameters will generally demonstrate decreased CO, normal to increased SVR, and normal to decreased ScvO2.
î Primary goals of therapy
■ Supportive: Although patients are preload dependent, excessive fluid administration can lead to right ventricular overload and impairment of LV filling, thereby worsening shock.
■ Definitive therapy involves relieving the obstruction (e.g., thoracostomy in the case of a pneumothorax, and pericardiocentesis in tamponade).
■ In a carefully selected group of patients, thrombolytic therapy may be beneficial in patients with pulmonary emboli.
• Cardiogenic: Shock caused by left ventricular systolic failure, resulting in decreased CO and subsequent insufficient oxygen distribution.
î Primary etiologies are myocardial infarction, acute mitral regurgitation, and myocarditis.
î Hemodynamic parameters will demonstrate decreased CO, increased SVR, and decreased ScvO2.
î Primary goals of therapy
■ Mitigation of pulmonary edema: NPPV or endotracheal intubation with mechanical ventilation reduces afterload, thereby encouraging forward flow, as well as preload. Additionally, the application of positive pressure to the alveolar space causes pulmonary edema fluid to move to the interstitial space.
■ Careful fluid management: Adequate preload to optimize ventricular function is important, but volume overload will worsen respiratory status, so careful fluid management is necessary. Volume removal (whether via diuresis or hemodialysis) is often a critical component of early management.
■ Definitive therapy for underlying cardiac disease: In the event of myocardial infarction, percutaneous revascularization should be performed in a timely fashion.
■ Supportive: Inotropic agents such as dobutamine may be used to augment CO. Other inotropes are discussed in “Pharmacologic Therapies.” Mechanical circulatory assist devices, including left ventricular assist devices and intra-aortic balloon pumps, may be necessary in patients who do not respond to medical therapy.
Septic Shock
• Definition of sepsis: Sepsis is defined as a life-threatening organ dysfunction caused by dysregulation of the host response to an infection.
î Sepsis was previously identified based on the presence of at least two systemic inflammatory response syndrome (SIRS) criteria:
■ Tachypnea: Respiratory rate >20 breaths/min or PaCO2 90 bpm
■ Hypo- or hyperthermia: Temperature >38°C or 0.5 ng/mL is suggestive of a bacterial infection while a PCT 0.05 μg∕kg∕min), vasoconstriction predominates owing to increased α1 activity.
Preferred agent for anaphylactic shock, and is also frequently used in cardiogenic shock.• Phenylephrine: Selective α1-receptor agonist causing vasoconstriction of larger arterioles. Few studies supporting its use in septic shock.
• Angiotensin II: Recent studies have investigated angiotensin II which engages the renin-angiotensin- aldosterone system. These studies showed that angiotensin II increased blood pressure in patients with vasodilatory shock.59
• Dobutamine: Inotropic agent that reduces afterload and increases stroke volume and heart rate via β1- agonist activity. Good agent for cardiogenic shock but increases risk of cardiac arrhythmias.
• Dopamine: Has inotropic, vasodilatory, and vasoconstrictive properties in a dose-dependent fashion due to action on peripheral α1-receptors, cardiac β1-receptors, and renal and splanchnic dopaminergic receptors. At doses 10 μg∕kg∕min, behaves as a vasopressor. Is associated with a higher rate of cardiac arrhythmias than norepinephrine.50
• Milrinone: Phosphodiesterase III inhibitor that has positive inotropic effect, causing increase in CO. Also causes systemic vasodilation, which decreases afterload, making it an alternative option for cardiogenic shock.
• Regarding venous access, low-dose norepinephrine, phenylephrine, and epinephrine may be infused peripherally for a limited period of time. However, central access is preferred as medication extravasation can lead to local ischemia.
î If extravasation occurs, phentolamine (an «-antagonist) can be injected into the area of extravasation to reduce ischemic injury.
î Peripheral administration of vasopressin and angiotensin II is not recommended.
ADJUNCTIVE THERAPIES
• Corticosteroids: Relative adrenal insufficiency may contribute to refractory hypotension during septic shock. Data do not support the use of corticosteroids in mild septic shock.
However, corticosteroids should be considered on an individual basis in patients with more severe shock, particularly in patients chronically on steroids. Generally, hydrocortisone 200-300 mg daily divided on a q6-8h basis is given. Previous trials have shown faster resolution of shock when administering hydrocortisone, but no difference in mortality.60,61 Another recent trial showed a benefit in 90-day mortality when hydrocortisone (50 mg every 6 hours) and Audricortisone (50 μg daily) were administered in conjunction.62• Sodium bicarbonate: No evidence supports the use of bicarbonate therapy in lactic acidemia from sepsis with a pH ≥7.15. Effect of bicarbonate on hemodynamics and vasopressor requirements with more severe acidemia is unknown, but bicarbonate is often recommended in patients with severe lactic acidemia (pH Structures that reflect sound waves poorly; shows as gray on ultrasound. Deeper structures are also more hypoechoic owing to attenuation with distance (e.g., lymph nodes, adipose tissue, muscle).
î Anechoic: Containing structures that allow sound waves to pass through freely; shows as black on ultrasound (e.g., blood vessels, transudative pleural effusion).
• Ultrasound to facilitate vascular access: More detailed instructions are available in the Washington Manual of Critical Care, Section XIX. Use of ultrasound to guide central venous access results in increased success and reduced complication rates.
î Location: Ultrasound guidance is most commonly used for internal jugular and femoral venous access.
î Before starting the procedure: Both internal jugular and femoral veins should be scanned to evaluate for aberrant anatomy or venous thrombosis.
î After applying the sterile field: The probe is positioned so that the needle is visualized for the entire duration of accessing the vessel.
î During the procedure: Following insertion of the guidewire, the length of the vessel is scanned to ensure that the guidewire did not inadvertently enter any adjacent arteries.
î After the procedure: Lung ultrasound can be used to rule out a pneumothorax.
• Cardiac ultrasound: Includes five standard views, reviewed below. Uses body transducer. Intended to facilitate assessment of volume responsiveness, global left and right ventricular systolic function, and valvular function.
î Parasternal long-axis view: Probe is placed adjacent to the sternum in the left third to fifth intercostal space with the orientation marker pointing toward the patient's right shoulder. The right ventricular outflow tract, left ventricular cavity, ascending aorta, mitral valve, and left atrium should be visualized. Assesses for pericardial effusion, left and right ventricular dysfunction, and valvular pathologies.
î Parasternal short-axis view: Probe remains adjacent to the sternum in the left third to fifth intercostal space, but orientation marker is rotated 90 degrees clockwise to point at the patient's left shoulder. Cross-sectional view of the left and right ventricles at the level of the papillary muscles should be visualized. Assesses for pericardial effusion and left and right ventricular dysfunction.
î Apical four-chamber view: Probe is placed between the midclavicular and midaxillary lines of the left lateral chest between the fifth and seventh intercostal spaces, underneath the left nipple, with the orientation marker pointed at 3 o'clock. The left and right ventricles and atria, as well as the tricuspid and mitral valves, should be visualized. Assesses left and right ventricular size and function. See Figure 8-4.
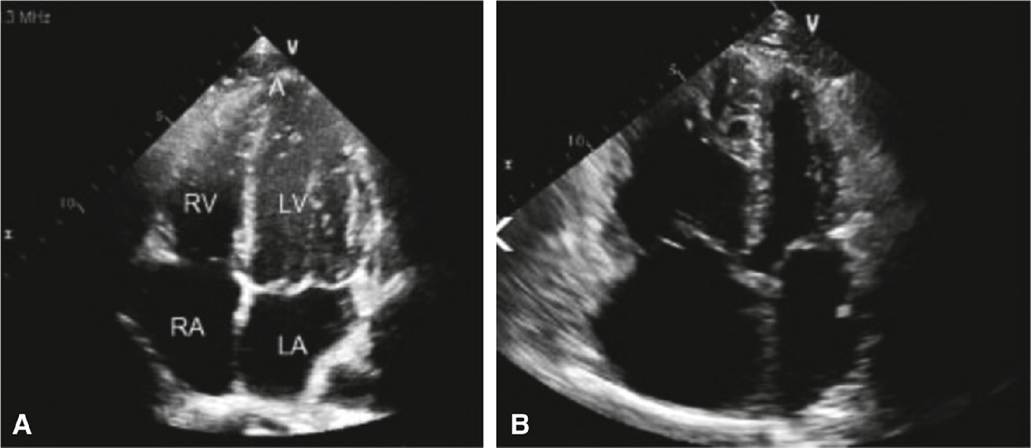
Figure 8-4 Cardiac ultrasound,Left (A): normal apical four-chamber view. A, apex; RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium. Right (B): demonstrates same view in a patient with right ventricular hypertrophy and dilation.
î Subcostal long-axis view: Probe is placed below the xiphoid process with the orientation marker pointed at 3 o'clock. The left and right ventricles and atria should be visualized. Assesses for pericardial effusion and left and right ventricular dysfunction. May be used for rapid assessment of cardiac function during performance of cardiopulmonary resuscitation.
î IVC longitudinal view: Probe remains below the xiphoid process, but orientation marker is rotated 90 degrees counterclockwise to point at 12 o'clock. IVC in the longitudinal axis should be visualized. Assesses IVC diameter during the respiratory cycle to determine volume responsiveness.
• Thoracic ultrasound: Includes four standard positions, performed bilaterally. Uses the body transducer on the abdominal setting to examine lung parenchyma; vascular transducer may be used for detailed examination of the pleura. Intended to facilitate the diagnosis of pleural effusion, pulmonary edema, pulmonary consolidation, and pneumothorax. Also used to guide a safe thoracentesis.
î Probe placement: Bedside lung ultrasound in emergency (BLUE)s protocol, intended for immediate diagnosis of acute respiratory failure, defines four areas for investigation.75 The orientation marker should be pointed toward the patient's head.
■ Upper BLUE point: Midclavicular line, second intercostal space
■ Lower BLUE point: Anterior axillary line, fourth or fifth intercostal space
■ Phrenic point: Midaxillary line, sixth or seventh intercostal space; location of the diaphragm
■ Posterolateral alveolar and/or pleural syndrome point: Posterior to the posterior axillary line, fourth or fifth intercostal space
î Anatomic landmarks and ultrasound appearance: Knowledge of the normal sonographic appearance of thoracic anatomy is paramount to identifying key structures.
■ Chest wall: Hypoechoic, linear shadows of soft tissue density.
■ Ribs: Hyperechoic, curvilinear structures with a deep, hypoechoic, posterior acoustic shadow.
■ Pleura: Bright, hyperechoic, roughly horizontal line located approximately 0.5 cm below rib shadows.
■ Diaphragm: Curvilinear, hyperechoic line that moves caudally with inspiration. In a seated patient, it is located caudad to the ninth rib.
■ Splenorenal and hepatorenal recesses: Should be confirmed before any procedure because its curvilinear appearance is similar to that of the diaphragm. Identified by visualization of the liver or spleen and the kidney caudally.
■ Lung: Air-filled lung appears hyperechoic due to the poor echogenicity of air. Atelectatic or consolidated lung appears hypoechoic relative to normal lung.
î Sonographic artifacts and terminology: A number of sonographic artifacts are caused by air-tissue interfaces, and presence or absence of these artifacts is indicative of disease.76
■ Pleural line: Brightly echogenic, roughly horizontal line; caused by parietopulmonary interface and indicating the lung surface.
■ A-lines: Brightly echogenic horizontal lines roughly parallel to the chest wall; caused by reverberations of the pleural line.
■ B-lines: Also called “comet tails”; a grouping within one intercostal space is called “lung rockets.” Hyperechoic line arising perpendicularly from the pleural line that extends across the whole screen without fading, erasing A-lines; moves with lung slide. Caused by thickened interlobular septa or ground-glass areas; isolated B-lines are a normal variant. See Figure 8-5.
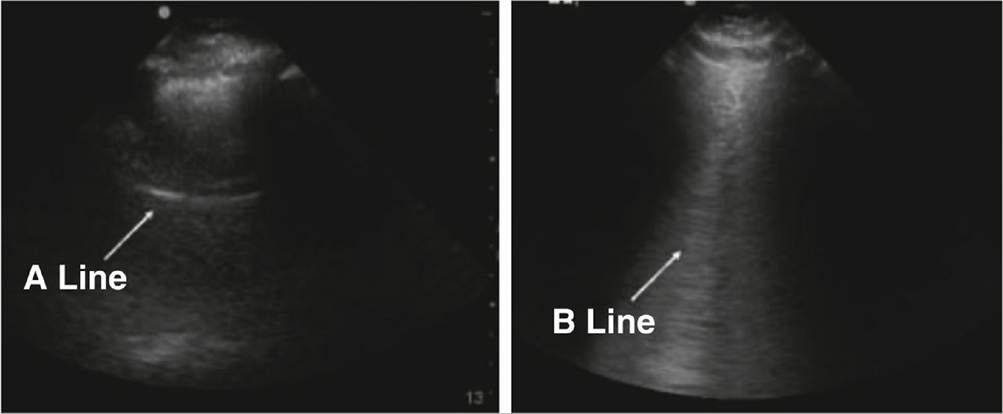
Figure 8-5 Lung ultrasound.A-lines demonstrated on left are equidistant horizontal lines created by reflections of the pleural line. B-lines demonstrated on the right are bright vertical lines that move with the pleura and extend to the bottom of the screen representing thickened fluid-filled interlobular septae.
■ Lung slide: “Twinkling” movement of the pleural line that occurs with the respiratory cycle; caused by movement of the lung along the craniocaudal axis during respiration. In M-mode, lung slide is visualized as the “seashore sign,” with the chest wall generating the “waves,” the aerated lung forming the “sand,” and the pleural line as the interface.
■ Lung pulse: Pulsation of the pleural line due to transmission of the heartbeat through noninflated lung.
î Ultrasonography of lung pathology
■ Pleural effusion: A fluid collection bordered by the diaphragm, chest wall, and lung surface.
Transudative effusions are typically anechoic; exudative effusions may have some echogenicity. If the effusion is loculated, septations—visualized as hyperechoic, weblike structures—may be seen. Atelectatic lung may be seen in the effusion.
■ Pneumothorax: Owing to air's poor echogenicity, diagnosis of pneumothorax on ultrasound is made by artifact analysis.
? The presence of lung slide or lung pulse effectively rules out pneumothorax in the location being investigated.
? Abolishment of lung slide has a characteristic stratosphere sign in M-mode, with loss of the “sand,” but is neither sufficient nor specific for diagnosis of pneumothorax.
? Lung point is pathognomonic for pneumothorax but has poor sensitivity. Occurs at the interface of the pneumothorax and aerated lung. Characterized by alternation between absent lung slide and present lung slide or B-lines in one location with respirations. In M-mode, will transition between seashore sign and stratosphere sign.
■ Pneumonia: Can only be visualized when the consolidation abuts the pleura. A heterogeneous, hypoechoic area with irregular margins where aerated lung abuts the consolidated area. Air bronchograms should be seen to make the diagnosis of pneumonia.
■ Pulmonary edema: Presence of multiple B-lines within one intercostal space (“lung rockets”) may indicate cardiogenic or noncardiogenic pulmonary edema. Corresponds to the Kerley B-lines seen on chest radiograph. Isolated B-lines are a normal variant.
• Abdominal ultrasound: Abdominal ultrasound in critical care is limited and intended to evaluate for intra-abdominal fluid and assess the urinary tract and abdominal aorta.
î Evaluating for intra-abdominal fluid: Standard evaluation of the trauma patient who may have intraabdominal bleeding includes the focused assessment with sonography for trauma (FAST) examination. The patient is in the supine position, and four views are obtained:
■ Hepatorenal space: The probe is placed on the right in the 10th or 11th intercostal space at the posterior axillary line with the orientation mark pointed cephalad.
■ Pelvis: The probe is placed in the suprapubic area with the orientation mark in the 3-o'clock position.
■ Perisplenic space: The probe is placed on the left in the 10th or 11th space at or slightly posterior to the posterior axillary line with the orientation mark pointed cephalad.
■ Pericardial space: The probe is placed in the subxiphoid position with the orientation marker in the 3-o'clock position.
î Paracentesis: Paracentesis should be performed under ultrasound guidance because there is evidence supporting a decrease in complications. More details can be found in the Washington Manual for Critical Care, Section XIX.
î Assessment of the urinary tract: Bedside ultrasonography can identify bladder distention or hydronephrosis.
■ Bladder distention: The probe is placed in the suprapubic position with the orientation marker pointed cephalad for longitudinal dimensions and in the 3-o'clock position for transverse dimensions.
■ Hydronephrosis: The probe should be placed slightly caudad to the locations used for examination of the hepatorenal and perisplenic spaces in the FAST examination. Hydronephrosis is characterized by thinning of the renal cortex as the collecting system dilates.
î Assessment of the abdominal aorta: The goal is to visualize the entire abdominal aorta to ensure that its diameter from outer wall to outer wall is Asthma Immunol. 2014;112:29-34.
23. National Heart Lung, and Blood Institute Acute Respiratory Distress Syndrome Clinical Trials
Network; Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. NEngl JMed. 2006;354:2564-2575.
24. Steinberg KP, Hudson LD, Goodman RB, et al. Efficacy and safety of corticosteroids for persistent
acute respiratory distress syndrome. N Engl J Med. 2006;354:1671-1684.
25. WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group; Sterne JAC,
Murthy S, Diaz JV, et al. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: a meta-analysis. J Am Med Assoc. 2020;324(13):1330.
26. Papazian L, Forel JM, Gacouin A, et al. Neuromuscular blockers in early acute respiratory distress
syndrome. NEngl J Med. 2010;363:1107-1116.
27. National Heart, Lung, and Blood Institute PETAL Clinical Trials Network; Moss M, Huang DT,
Brower RG, et al. Early neuromuscular blockade in the acute respiratory distress syndrome. N Engl JMed. 2019;380(21):1997.
28. Guerin C, Reignier J, Richard JC, et al. Prone positioning in severe acute respiratory distress
syndrome. NEngl JMed. 2013;368:2159-2168.
29. Noah MA, Peek GJ, Finney SJ, et al. Referral to an extracorporeal membrane oxygenation center and
mortality among patients with severe 2009 influenza A(H1N1). J Am Med Assoc. 2011;306:1659- 1668.
30. Combes A, Hajage D, Capellier G, et al. Extracorporeal membrane oxygenation for severe acute
respiratory distress syndrome. NEngl J Med. 2018;378:1965-1975.
31. Kollef MH. Health care-associated pneumonia: perception versus reality. Clin Infect Dis.
2009;49:1875-1877.
32. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and
ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63:e61-e111.
33. Yang KL, Tobin MJ. A prospective study of indexes predicting the outcome of trials of weaning from
mechanical ventilation. N Engl J Med. 1991;324:1445-1450.
34. Khemani RG, Randolph A, Markovitz B. Corticosteroids for the prevention and treatment of post
extubation stridor in neonates, children and adults. Cochrane Database Syst Rev. 2009; (3):CD001000.
35. Boles JM, Bion J, Connors A, et al. Weaning from mechanical ventilation. Eur Respir J.
2007;29:1033-1056.
36. Blackwood B, Burns KE, Cardwell CR, O’Halloran P. Protocolized versus non-protocolized weaning for reducing the duration of mechanical ventilation in critically ill adult patients. Cochrane Database SystRev. 2014;(11):CD006904.
37. Hess D. Ventilator modes used in weaning. Chest. 2001;120:474S-476S.
38. Burns KE, Meade MO, Premji A, Adhikari NK. Noninvasive positive-pressure ventilation as a
weaning strategy for intubated adults with respiratory failure. Cochrane Database Syst Rev. 2013; (12):CD004127.
39. Nava S, Gregoretti C, Fanfulla F, et al. Noninvasive ventilation to prevent respiratory failure after
extubation in high-risk patients. Crit Care Med. 2005;33:2465-2470.
40. Ferrer M, Sellares J, Valencia M, et al. Non-invasive ventilation after extubation in hypercapnic
patients with chronic respiratory disorders: randomised controlled trial. Lancet. 2009;374:1082- 1088.
41. Hernandez G, Vaquero C, Gonzalez P, et al. Effect of postextubation high-flow nasal cannula vs
conventional oxygen therapy on reintubation in low-risk patients: a randomized clinical trial. J Am Med Assoc. 2016;315:1354-1361.
42. Maggiore SM, Idone FA, Vaschetto R, et al. Nasal high-flow versus Venturi mask oxygen therapy after
extubation. Effects on oxygenation, comfort, and clinical outcome. Am J Respir Crit Care Med. 2014;190(3):282-288.
43. Hernandez G, Vaquero C, Colinas L, et al. Effect of postextubation high-flow nasal cannula vs
noninvasive ventilation on reintubation and postextubation respiratory failure in high-risk patients: a randomized clinical trial. J Am Med Assoc. 2016;316:1565-1574.
44. De Jonghe B, Sharshar T, Hopkinson N, Outin H. Paresis following mechanical ventilation. Curr
Opin Criti Care. 2004;10:47-52.
45. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis
and septic shock (Sepsis-3). J Am Med Assoc. 2016;315:801-810.
46. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis
and septic shock. NEngl J Med. 2001;345:1368-1377.
47. Levy MM, Evans LE, Rhodes A. The surviving sepsis campaign bundle: 2018 update. Crit Care Med.
2018;46:997-1000
48. Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults.
NEngl J Med. 2018;378:829-839.
49. Finfer S, Bellomo R, Boyce N, et al. A comparison of albumin and saline for fluid resuscitation in the
intensive care unit. N Engl J Med. 2004;350(22) :2247.
50. De Backer D, Biston P, Devriendt J, et al. Comparison of dopamine and norepinephrine in the
treatment of shock. NEngl J Med. 2010;362:779-789.
51. Liu VX, Fielding-Singh V Greene JD, et al. The timing of early antibiotics and hospital mortality in
sepsis. Am J Respir Crit Care Med. 2017;196:856-863.
52. Marshall JC, Maier RV, Jimenez M, Dellinger EP. Source control in the management of severe sepsis
and septic shock: an evidence-based review. Crit Care Med. 2004;32:S513-S526.
53. Pro CI, Yealy DM, Kellum JA, et al. A randomized trial of protocol-based care for early septic shock.
NEngl J Med. 2014;370:1683-1693.
54. ARISE Investigators; ANZICS Clinical Trials Group; Peake SL, Delaney A, Bailey M, et al. Goal-
directed resuscitation for patients with early septic shock. N Engl J Med. 2014;371:1496-1506.
55. Marty P, Roquilly A, Vallee F, et al. Lactate clearance for death prediction in severe sepsis or septic
shock patients during the first 24 hours in Intensive Care Unit: an observational study. Ann Intensive Care. 2013;3:3.
56. Wacker C, Prkno A, Brunkhorst FM, Schlattmann P. Procalcitonin as a diagnostic marker for sepsis: a
systematic review and meta-analysis. Lancet Infect Dis. 2013;13:426-435.
57. Schuetz P, Wirz Y, Sager R, et al. Procalcitonin to initiate or discontinue antibiotics in acute
respiratory tract infections. Cochrane Database SystRev. 2017;(10):CD007498. doi:10.1002/14651858.CD007498.pub3
58. Russell JA, Walley KR, Singer J, et al. Vasopressin versus norepinephrine infusion in patients with
septic shock. NEngl J Med. 2008;358:877-887.
59. Khanna A, English SW, Wang XS, et al. Angiotensin II for the treatment of vasodilatory shock. N Engl
J Med. 2017;377:419-430.
60. Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for patients with septic shock. NEngl J
Med. 2008;358:111-124.
61. Venkatesh B, Finfer S, Cohen J, et al. Adjunctive glucocorticoid therapy in patients with septic shock.
NEngl J Med. 2018;378:797-808.
62. Annane D, Renault A, Brun-Buisson, et al. Hydrocortisone plus fludrocortisone for adults with septic
shock. NEngl J Med. 2018;378:809-818.
63. Paciullo CA, McMahon Horner D, Hatton KW, Flynn JD. Methylene blue for the treatment of septic
shock. Pharmacotherapy. 2010;30:702-715.
64. Marik PE, Baram M, Vahid B. Does central venous pressure predict fluid responsiveness? A
systematic review of the literature and the tale of seven mares. Chest. 2008;134:172-178.
65. Antonelli M, Levy M, Andrews PJ, et al. Hemodynamic monitoring in shock and implications for
management. International Consensus Conference, Paris, France, 27-28 April 2006. Intensive Care Med. 2007;33:575-590.
66. Jones AE, Shapiro NI, Trzeciak S, et al.; Emergency Medicine Shock Research Network
(EMShockNet) Investigators. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. J Am Med Assoc. 2010;303(8):739-746.
67. Richard C, Warszawski J, Anguel N, et al. Early use of the pulmonary artery catheter and outcomes in
patients with shock and acute respiratory distress syndrome: a randomized controlled trial. J Am Med Assoc. 2003;290:2713-2720.
68. Dark PM, Singer M. The validity of trans-esophageal Doppler ultrasonography as a measure of
cardiac output in critically ill adults. Intensive Care Med. 2004;30:2060-2066.
69. Monnet X, Rienzo M, Osman D, et al. Esophageal Doppler monitoring predicts fluid responsiveness
in critically ill ventilated patients. Intensive Care Med. 2005;31:1195-1201.
70. Michard F, Boussat S, Chemla D, et al. Relation between respiratory changes in arterial pulse
pressure and fluid responsiveness in septic patients with acute circulatory failure. Am J Respir Crit Care Med. 2000;162:134-138.
71. Barbier C, Loubieres Y, Schmit C, et al. Respiratory changes in inferior vena cava diameter are
helpful in predicting fluid responsiveness in ventilated septic patients. Intensive Care Med. 2004;30:1740-1746.
72. Corl K, Napoli AM, Gardiner F. Bedside sonographic measurement of the inferior vena cava caval
index is a poor predictor of fluid responsiveness in emergency department patients. Emerg Med Australas. 2012;24:534-539.
73. Kupersztych-Hagege E, Teboul JL, Artigas A, et al. Bioreactance is not reliable for estimating cardiac
output and the effects of passive leg raising in critically ill patients. Br J Anaesth. 2013;111:961- 966.
74. Benomar B, Ouattara A, Estagnasie P, et al. Fluid responsiveness predicted by noninvasive
bioreactance-based passive leg raise test. Intensive Care Med. 2010;36:1875-1881.
75. Lichtenstein DA. Lung ultrasound in the critically ill. Ann Intensive Care. 2014;4:1.
76. Lichtenstein DA. Ultrasound in the management of thoracic disease. Crit Care Med. 2007;35:S250-
S261.