Mechanical Ventilation
GENERAL PRINCIPLES
Basic modes of ventilation: One can determine how the ventilator initiates a breath (triggering), how the breath is delivered, how patient-initiated breaths are supported, and when to terminate the breath to allow expiration (cycling).
• Initiation of a breath: Triggering of a ventilator occurs after a period of time has elapsed (time triggered) or when the patient has generated sufficient negative airway pressure or inspiratory flow exceeding a predetermined threshold (patient triggered).
• Modes of ventilation
î Assist-control (AC) ventilation: Ventilator delivers a fully supported breath whether time or patient triggered. Primary mode of ventilation used in respiratory failure.
î Synchronized intermittent mandatory ventilation (SIMV): Ventilator delivers a fully supported breath when time triggered. However, when the breath is patient triggered, the ventilator delivers a pressure-supported breath (at a level set by the clinician). The size of the patient-triggered breath depends on lung compliance and patient's effort. This mode is commonly used in surgical patients.
î Pressure support ventilation (PSV): Spontaneous mode of ventilation without a set respiratory rate. Delivers a clinician-determined inspiratory pressure during patient-triggered breathing. No respiratory rate is set, so there is no guaranteed minute ventilation.
• Type of breath delivered
î Volume control (VC): Ventilator delivers a clinician-determined tidal volume (Vt) for each breath regardless of whether the breath was time or patient triggered. When predetermined Vt is delivered, airflow is terminated and exhalation occurs.
î Pressure control (PC): Delivers a practitioner-determined inspiratory pressure for each breath. When inspiratory time has elapsed, inspiratory pressure is terminated and exhalation occurs.
The tidal volume varies based on lung compliance. PC ventilation does not deliver a guaranteed Vt or minute ventilation and may lead to hypoventilation. However, PC may improve patient synchrony and comfort while on the ventilator.• Basic ventilator terminology and management: Flow-time and pressure-time tracings are demonstrated in Figure 8-1.
î Minute ventilation: Defined as the product of Vt and respiratory rate (Vt ? RR). Normally between 5 and 10 L/min in resting adults, but may be much higher in high metabolic states, e.g., septic shock.
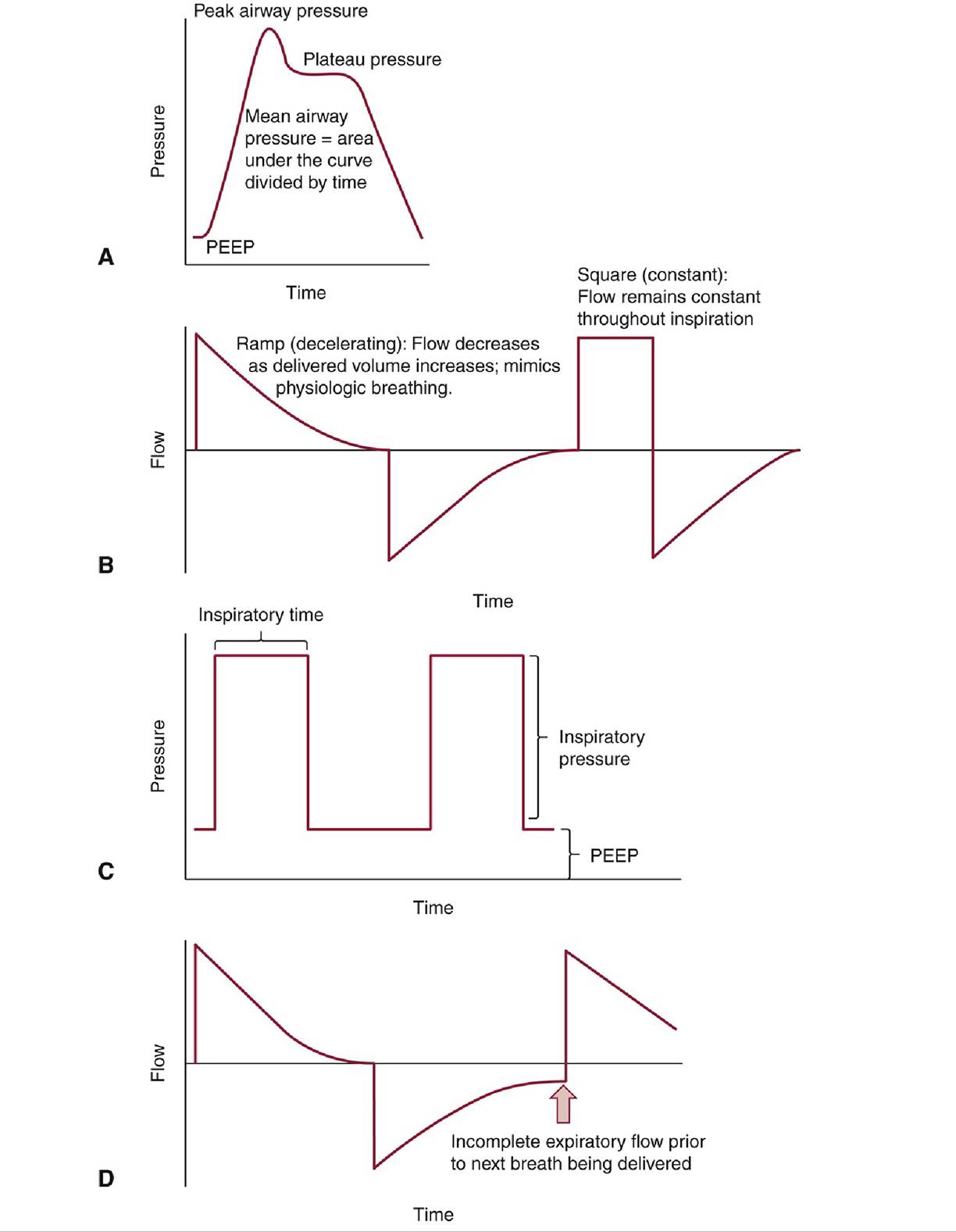
Figure 8-1 Flow-time and pressure-time tracings.A, Pressure-time curve for one breath. B, Flow-time curve for volume control ventilation. Pressure varies throughout inspiratory time, depending on lung compliance. C, Pressure-time curve for pressure control ventilation. Flow varies throughout inspiratory time, depending on lung compliance. D, Flowtime curve demonstrating auto-positive end-expiratory pressure (auto-PEEP).
î Peak airway pressure: Composed of pressures necessary to overcome inspiratory airflow resistance, chest wall recoil resistance, and alveolar opening resistance. Does not reflect alveolar pressure.
î Mean airway pressure: Mean pressures applied during the inspiratory cycle. Approximates alveolar pressure until overdistention occurs.
î Plateau pressure (Pp∣at): Reflects alveolar pressure. Checked by performing an end-inspiratory hold maneuver to allow pressures through the tracheobronchial tree to equilibrate.
Ventilator Settings
Initial ventilator settings: One must decide on a ventilator mode (AC vs. SIMV), control (VC vs. PC), respiratory rate, FIO2, and PEEP. AC/VC is the most commonly used mode.
• For VC, the following must be entered:
î Vt: Generally, begin at 6-8 mL/kg ideal body weight (IBW) to prevent barotrauma.
There is growing evidence that low tidal volume ventilation may be beneficial in patients whether or not they have acute ARDS and should be routinely used whenever possible.12 IBW can be calculated as follows: Male IBW = 50 kg + 2.3 kg/in. ? (Height in inches - 60) (imperial), 50 kg + 1.1 kg/cm ? (Height in cm - 152.4) (metric); Female IBW = 45.5 kg + 2.3 kg/in. ? (Height in inches - 60) (imperial), 45.5 kg + 1.1 kg/cm ? (Height in cm - 152.4) (metric).î Inspiratory flow rate: May be constant (square wave) or ramp (decelerating). Recommend 60 L/min or greater. Higher flow rates increase expiration time, which may be important in obstructive lung disease to prevent auto-PEEP (ventilator delivers a breath before the patient has been able to fully expire).
• FIO2: It is reasonable to start at 100%, but FIO2 should be weaned down quickly to maintain SaO2 >87% or PaO2 >55 mm Hg. There is growing evidence that tolerating hyperoxia after intubation may actually worsen patient survival.13 FIO2 can generally be quickly titrated down based on pulse oximetry alone.
• PEEP: It is generally reasonable to start at 5-10; however, higher values are frequently used in the treatment of ARDS.
î ARDSNet publishes recommended strategies for PEEP and FIO2 levels, which are available on their website (http://www.ardsnet.org).
î Morbidly obese patients may also require higher PEEP.
Advanced Modes of Ventilation
Advanced modes should generally only be used after discussion with higher level practitioners.
• Pressure-regulated VC ventilation: Ventilator determines, after each breath, if inspiratory pressure was sufficient to achieve targeted Vt; if insufficient or excessive, then ventilator will adjust inspiratory pressure to achieve desired Vt. PRVC applies a constant pressure throughout inspiration, resulting in a decelerating and variable flow pattern that is more comfortable for some patients.
• Inverse-ratio ventilation (IRV): A pressure-controlled method of ventilation most commonly used in ARDS. Inspiratory time exceeds expiratory time to improve oxygenation at the expense of ventilation; patients are permitted to become hypercapnic to pH 7.20. If obstructive lung disease is present, can cause auto-PEEP and excessive hypercapnia.
• Airway pressure release ventilation (APRV): An extreme version of IRV; inspiratory pressure (Phigh) applied for a prolonged period of time (Thigh) with a short expiratory time (Tlow, or release time)— usually with severe asthma exacerbations.22
Considerations in Acute Respiratory Distress Syndrome
• Fluids: Conservative fluid management (pulmonary capillary wedge pressure 1 week.
î A histamine-2 receptor antagonist or proton pump inhibitor can be used for prophylaxis with some controversy on what agent is preferred.
î The use of ulcer prophylaxis may increase the risk of nosocomial infections, but benefits are likely greater than risks in the above patients.
• Oxygen toxicity: Breathing high FIO2 can lead to excessive free radical generation and result in lung injury.
î Reducing FIO2 to the lowest tolerable oxygen saturation (O2 saturation of 90% or PaO2 of 65 mm Hg) is advisable. There is evidence that tolerating hyperoxia after intubation may worsen patient survival.13
Liberation From Mechanical Ventilation
• Parameters demonstrating readiness to wean: Daily assessment of readiness for extubation should be done once the underlying disease process begins to resolve and minimal ventilator support is required. The following criteria should generally be met before extubation:
î Minimal ventilator support: FIO2 ≤40%, PEEP 5 cm H2O to maintain SpO2 >90%.
° Arterial blood gas: pH and PaCO2 should be at the patient's baseline; particularly important for patients with chronic CO2 retention.
î Ventilation requirement: Minute ventilation should be easily suctioned; patient should not require suctioning more frequently than every 4 hours before extubation.
î Strength: Patient should have strong cough and be able to lift head off the bed and hold it in flexion for >5 seconds.
° Breathing trial: Patient should be able to generate spontaneous Vt >5 mL/kg IBW.
î Rapid shallow breathing index (RSBI): RSBI should be ≤105. Defined as ratio of respiratory rate to Vt in liters (f/VT). RSBI >105 accurately predicts weaning failure, but RSBI ≤105 is less accurate at predicting weaning success.33
î Patency of airway: In patients with concern for laryngeal edema (e.g., angioedema, traumatic intubation), cuff leak should be checked before extubation. Absence of cuff leak should generally preclude extubation, and patients should be treated with IV corticosteroids for 12-24 hours before extubation.34
î Some patients felt to be ready to extubate based on all objective criteria will still fail extubation. Failure rates as high as 23.5% have been reported.35
• Weaning strategies: Sedation interruption and breathing trials for 30-120 minutes should be done daily and is the most important predictor of timely liberation from mechanical ventilation.36 Weaning strategies include the following:
î PSV: No time-triggered breaths, but patient remains connected to the ventilator. PEEP is usually at 5 cm H2O, with low levels of pressure support (5-10 cm H2O) during spontaneous breathing.
î T-piece/spontaneous breathing trial: Patient is removed from the ventilator but remains intubated. Endotracheal tube is connected to a heated, humidified circuit with minimal or no supplemental oxygen. End-tidal CO2 monitoring may be used for additional safety.
î SIMV: Used most frequently in surgical and neurosurgical patients. Set respiratory rate is gradually decreased over hours to days until patient is primarily breathing spontaneously.
î SIMV has the poorest weaning outcomes of all techniques. However, neither T-piece nor PSV has proven to be more predictive of successful extubation.37
• Management following extubation: Patients need to be closely monitored following extubation. Good airway clearance and oxygenation decrease the risk of reintubation.
î Extubation to NPPV: In patients with COPD who are intubated for acute respiratory failure, extubation to NPPV is associated with a reduction in mortality and health care-associated pneumonia.38 More generally, in patients with chronic hypercapnic respiratory failure, two trials have found that the use of NPPV reduces rates of reintubation following extubation.39,40 Similar benefit of NPPV has not been demonstrated in other etiologies of respiratory failure.
î Extubation to HFNC: The use of HFNC may also have a beneficial role in the prevention of postextubation respiratory failure in select low-risk patients. When patients were randomly assigned to HFNC versus conventional oxygen therapy after extubation, patients who received HFNC were less likely to be intubated within 48-72 hours.41,42 Other studies have shown HFNC to be noninferior when compared with NPPV in preventing reintubation.43
• Failure to wean: Defined as inability to liberate from mechanical ventilation 48-72 hours after resolution of underlying disease process. Factors that should be considered include the following:
î Endotracheal tubes with smaller inner diameter increase airway resistance and may make breathing trials more difficult.
î Use of neuromuscular blockade is associated with prolonged weakness, particularly when used with corticosteroids.44
î Critical illness myopathy and polyneuropathy places the patient at risk for recurrent respiratory failure.
î Psychiatric illnesses (delirium, anxiety, PTSD, etc.) may interfere with SBTs and other standard weaning protocols.
î Acid-base disturbances may make liberation from mechanical ventilation difficult.
■ Non-anion gap metabolic acidosis causes compensatory increase in minute ventilation (respiratory alkalosis) to normalize pH, which can lead to tachypnea and respiratory fatigue upon extubation.
■ Metabolic alkalosis causes blunting of ventilatory drive and decrease in minute ventilation (respiratory acidosis) to maintain normal pH, which can lead to hypercapnia upon extubation.
More on the topic Mechanical Ventilation:
- ADMISSION CRITERIA FOR PICU
- Improving services
- Complications of neuraxial anaesthesia
- REFERENCES
- CONGENITAL LUNG MALFORMATIONS
- Management of preterm prelabour rupture of the membranes
- Cardiopulmonary Resuscitation
- 3 Critical Care
- Macrovascular Complications of Diabetes Mellitus
- 7 Complications of Labor and Delivery