Airway Management and Endotracheal Intubation
GENERAL PRINCIPLES
Airway Management Before Intubation
• Head and jaw positioning: First, the oropharynx should be inspected, and all foreign bodies should be removed. If the patient is unresponsive, the head tilt-chin lift maneuver should be performed.
If neck immobilization is required, jaw thrust should be performed.• Oral and nasopharyngeal airways: Airway adjunct devices can be used to maintain a patent airway. Initially inserted with the concave curve of the airway facing toward the roof of the mouth. The oral airway then is turned 180 degrees as it is inserted so that the concave curve of the airway follows the natural curve of the tongue. Careful monitoring of airway patency is required, as malpositioning can push the tongue posteriorly and result in oropharyngeal obstruction. Nasopharyngeal airways are made of soft plastic and passed easily down one of the nasal passages to the posterior pharynx after topical nasal lubrication and anesthesia with viscous lidocaine jelly.
• Bag-valve-mask ventilation: Ineffective respiratory efforts can be augmented with simple bag-valve- mask ventilation. Proper fitting and positioning of the mask using the “EC” hand position—thumb and index finger forming a “C” around the mask, and the remaining fingers forming an “E” to support the jaw—ensure a tight seal around the mouth and nose. This maneuver should be used in conj unction with proper positioning and airway adjuncts (e.g., an oral airway). If possible, two hands should be used to optimize seal while a second clinician ventilates the patient. Bag-valve-mask ventilation is a critical skill in airway management and is frequently incorrectly performed.
• Laryngeal mask airway (LMA): The LMA is a supraglottic airway device shaped like an endotracheal tube connected to an elliptical mask. It is designed to be inserted over the tongue and seated in the hypopharynx, covering the supraglottic structures and relatively isolating the trachea.
It is a temporary airway and should not be used for prolonged ventilatory support. LMAs can be lifesaving in establishing an airway when endotracheal intubation cannot be easily achieved.Endotracheal Intubation
• Indications: Refractory hypoxemic respiratory failure, hypercapnic respiratory failure, airway protection (e.g., intoxication, head trauma, severe upper GI bleeding with hematemesis), upper airway obstruction (e.g., angioedema, tumor), severe metabolic acidosis or shock (e.g., type 4 respiratory failure, severe diabetic ketoacidosis), and need for hyperventilation as a treatment for increased intracranial pressure.
• Before endotracheal tube intubation is attempted:
î Ensure that monitoring equipment is working (including pulse oximetry, telemetry, and blood pressure monitoring) and that the patient has adequate working intravenous (IV) access.
î Ensure that all necessary equipment is at the bedside including working suction equipment, endotracheal tube (with stylet, lubricant, and balloon tested), 10 mL syringe to fill endotracheal tube balloon, oral or nasopharyngeal airway, bag-valve-mask connected to 15 L/min oxygen, direct or video laryngoscope, end-tidal CO2 monitor, medications for intubation, and tape or endotracheal holder.
î Have the plan articulated and the equipment at the bedside (e.g., tracheal tube introducer and supraglottic device) in case of a difficult airway.
î Evaluate head and neck positioning: Oral, pharyngeal, and tracheal axes should be aligned by flexing the neck and extending the head, achieving the “sniffing” position. Obese patients may require a shoulder roll or ramp.
î The selected agents for intubation including neuromuscular blocking agents, opiates, and anxiolytics should be chosen based on their respective advantages and disadvantages in the given clinical situation. Commonly used agents for intubation are listed in Table 8-2.
TABLE 8-2
| DRUGS TO FACILITATE ENDOTRACHEAL INTUBATION | |||||||||||
| Drug | Action | Dose (IV) | Onset (s) | Duration (min) | Comment | ||||||
| Propofol | Sedation, amnesia | Unstable: 0.5 mg/kg Stable 1-1.5 mg/kg | 30-60 | 5-10 | Causes hypotension and bradycardia; beneficial in seizures | ||||||
| Midazolam | Sedation, amnesia | 0.02 0.08 mg/kg (generally 1 5 mg in adult) | 30-60 | 15-30 | Causes hypotension; beneficial in seizures | ||||||
| Fentanyl | Analgesia | ~2 μg∕kg | 15 | 30-60 | Causes hypotension; used at lower doses as an adjunctive agent | ||||||
| Etomidate | Sedation | Unstable: 0.15 mg/kg Stable 0.3 mg/kg | 15-45 | 3-12 | Hemodynamically neutral; inhibits cortisol synthesis; decreases seizure threshold | ||||||
| Ketamine | Sedation, amnesia, analgesia | 1-3 mg/kg | 30 | 5-10 | Increases HR and BP; bronchodilator; may elevate ICP | ||||||
| Succinylcholine | Paralytic | 1-1.5 mg/kg | 30-60 | 5-15 | Contraindicated in hyperkalemia, history of malignant hypothermia, myopathy | ||||||
| Rocuronium | Paralytic | 1 mg/kg | 45-60 | 30-45 | Caution if difficult intubation or bag-valve- mask ventilation anticipated | ||||||
BP, blood pressure; HR, heart rate; ICP, intracranial pressure.
î If patient not in extremis/cardiac arrest, a verbal time-out should be performed.
• Techniques
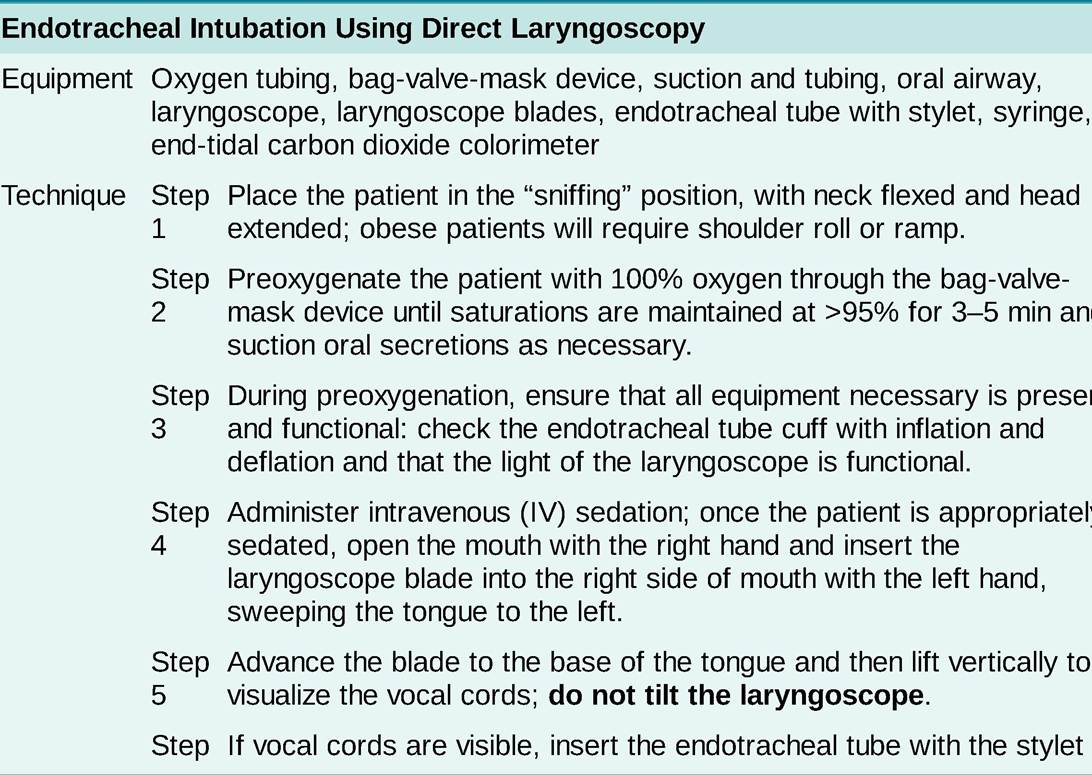
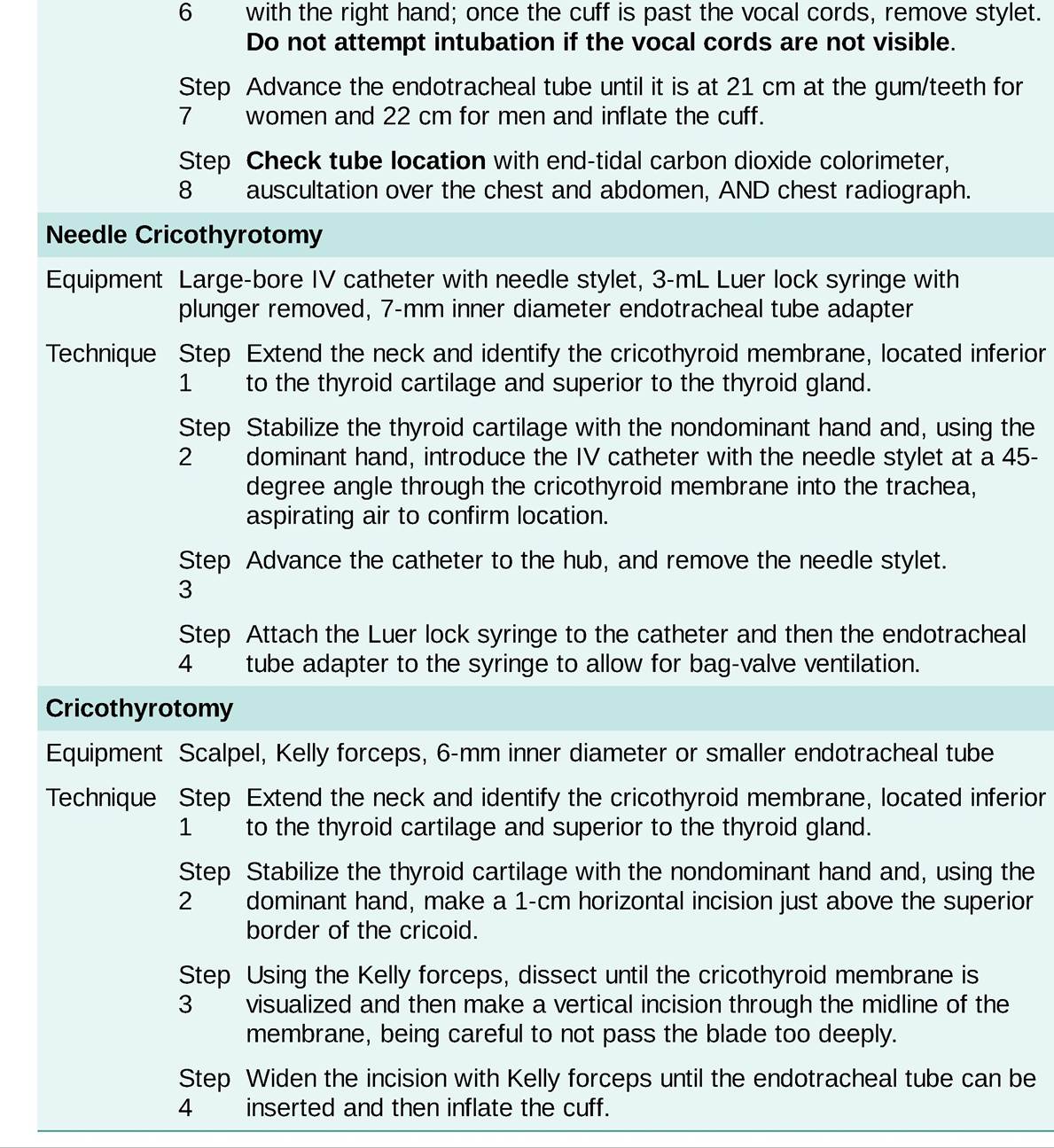
î Direct Iaryngoscopic orotracheal intubation: Most commonly used, requiring only a direct laryngoscope and light source. Procedure available in Table 8-3.
TABLE 8-3
PROCEDURE FOR ENDOTRACHEAL INTUBATION, NEEDLE CRICOTHYROTOMY, AND CRICOTHYROTOMY
î Video Iaryngoscopic orotracheal intubation: Allows for direct visual confirmation of intubation by a second observer via video monitoring and is particularly beneficial in more difficult airways.
î Advanced techniques for specialists include blind nasotracheal intubation and flexible fiber optically guided orotracheal or nasotracheal intubation.
• Verification of correct endotracheal tube location and positioning: Proper tube location must be ensured by:
° Fiber optic inspection of the airways through the endotracheal tube; or
î Direct visualization of the endotracheal tube passing through the vocal cords; and
î Use of an end-tidal CO2 monitor; and
î CXR.
î Clinical evaluation of the patient (i.e., listening for bilateral breath sounds over the chest and the absence of ventilation over the stomach) and radiographic evaluation alone are unreliable for establishing correct endotracheal tube location.
î The tip of the endotracheal tube should be 3-5 cm above the carina, depending on head and neck position.
• After successful intubation:
î Tracheal tube cuff pressures: Should be monitored at regular intervals and maintained below capillary filling pressure (25 mm Hg) to prevent ischemic mucosal injury.
î Sedation: Anxiolytics and opiates are frequently used to facilitate endotracheal intubation and mechanical ventilation. Commonly used agents are listed in Table 8-4.
TABLE 8-4
| COMMONLY USED SEDATION MEDICATIONS IN THE INTENSIVE CARE UNIT | |||
| Drug | Dose (IV) | Time to Arousal | Comment |
| Propofol | 20 100 μg∕kg∕min | 10 15 min | Causes hypotension, may cause hypertriglyceridemia or propofol-related infusion syndrome, beneficial in bronchospasm |
| Midazolam | 1-10 mg/h | 1-2 h | Arousal time can be prolonged; active metabolite accumulates in renal failure; associated with delirium |
| Fentanyl | 25-200 μg∕h | 15 s | Can cause chest wall rigidity and serotonin syndrome at higher doses |
| Ketamine | 0.5 3 mg/kg/h | 5 10 min | May cause hypertension and tachycardia; may experience reemergence hallucinations, beneficial in bronchospasm. |
| Dexmedetomidine | 0.1 1.5 mg/kg/h | 6 10 min | Does not cause respiratory depression, can cause hypotension and bradycardia |
• Complications: Improper endotracheal tube location or positioning is the most important immediate complication to be recognized and corrected.
î Esophageal intubation should be suspected if no end-tidal CO2 is detected after three to five breaths, hypoxemia persists or develops, there is a lack of breath sounds, or abdominal distention or regurgitation of stomach contents occurs.
° Mainstem intubation should be suspected if peak airway pressures are elevated or there are unilateral breath sounds.
î Other complications include dislodgment of teeth and upper airway trauma.
Surgical Airways
• Indications for surgical airways in critical care
î Life-threatening upper airway obstruction (e.g., epiglottitis, angioedema, facial burns, laryngeal/vocal cord edema) preventing bag-valve-mask ventilation and endotracheal intubation.
î Need for prolonged respiratory support.
• Needle cricothyrotomy: Indicated in emergency settings when the patient cannot be ventilated noninvasively, standard endotracheal intubation is unsuccessful, and a surgical airway cannot be immediately performed. The steps of the procedure are listed in Table 8-3.
î Cricothyrotomy: Indicated in emergency settings when the patient cannot be ventilated noninvasively and standard endotracheal intubation is unsuccessful. The steps of the procedure are listed in Table 8-3.
• Tracheostomy: Predominantly performed owing to need for prolonged respiratory support.
î The optimal time to perform a tracheostomy in a patient requiring prolonged respiratory support is somewhat controversial. A 2010 randomized controlled trial (RCT) did not demonstrate any benefit in regard to occurrence of ventilator-associated pneumonia (VAP) or long-term outcomes for those who received an early tracheostomy (after 6-8 days of intubation) compared with late tracheostomy (after 12-14 days of intubation).9 A 2013 multicenter RCT from the United Kingdom comparing early (within 4 days of intubation) vs late (after 10 days) tracheostomy found no difference in 30-day mortality, ICU length of stay (LOS), or hospital LOS between the two groups.10 Generally, tracheostomy should be considered if prolonged ventilatory support is anticipated after 10-14 days of endotracheal intubation.
î Complications: Tracheostomy sites require at least 72 hours to mature, and tube dislodgment before maturation can lead to serious and life-threatening complications.
■ A tracheostomy tube that has been dislodged before stoma maturation should not be reinserted owing to the risk of creating a false tract.
■ Standard endotracheal intubation should be performed if a tracheostomy tube is dislodged before stoma maturation.
■ Tracheoinnominate artery fistulas are an uncommon but life-threatening complication of a tracheostomy that occurs when an abnormal tract develops between the innominate artery and trachea, leading to hemorrhage. This complication most commonly occurs 7-14 days after the tracheostomy but can occur up to 6 weeks after the procedure. Immediate management includes overinflation of the tracheostomy tube cuff, digital compression of the stoma, and surgical exploration.11
More on the topic Airway Management and Endotracheal Intubation:
- Airway Management and Endotracheal Intubation
- Emergent Airway Adjuncts
- Anaphylaxis
- Macrovascular Complications of Diabetes Mellitus
- Head Trauma
- Hemoptysis
- Chronic Obstructive Pulmonary Disease