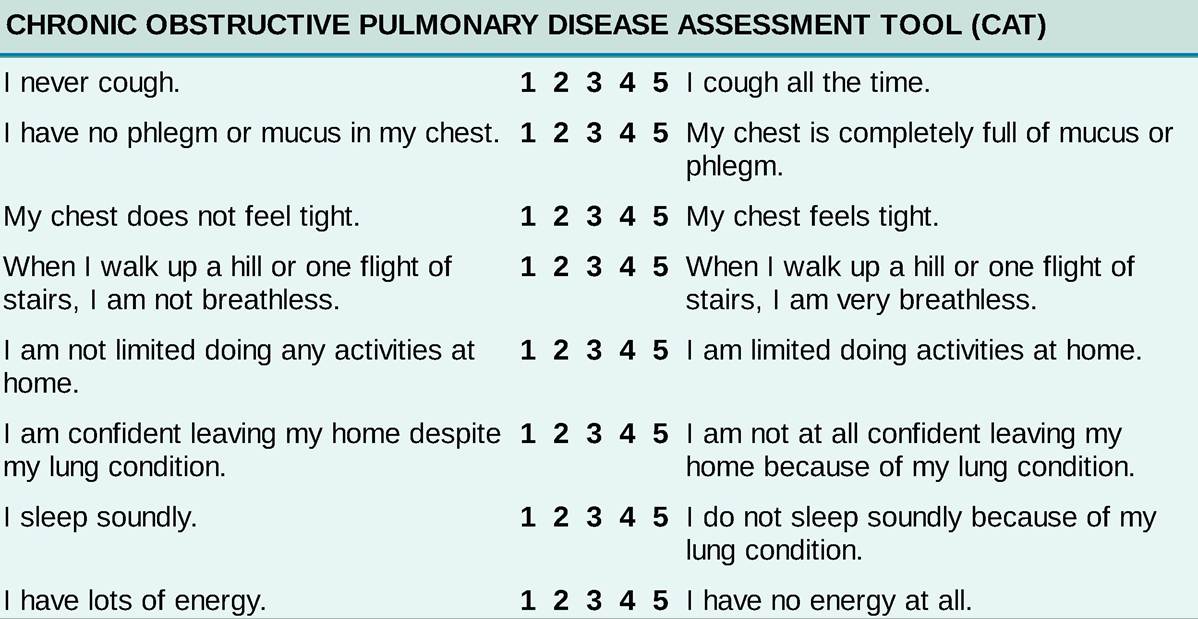
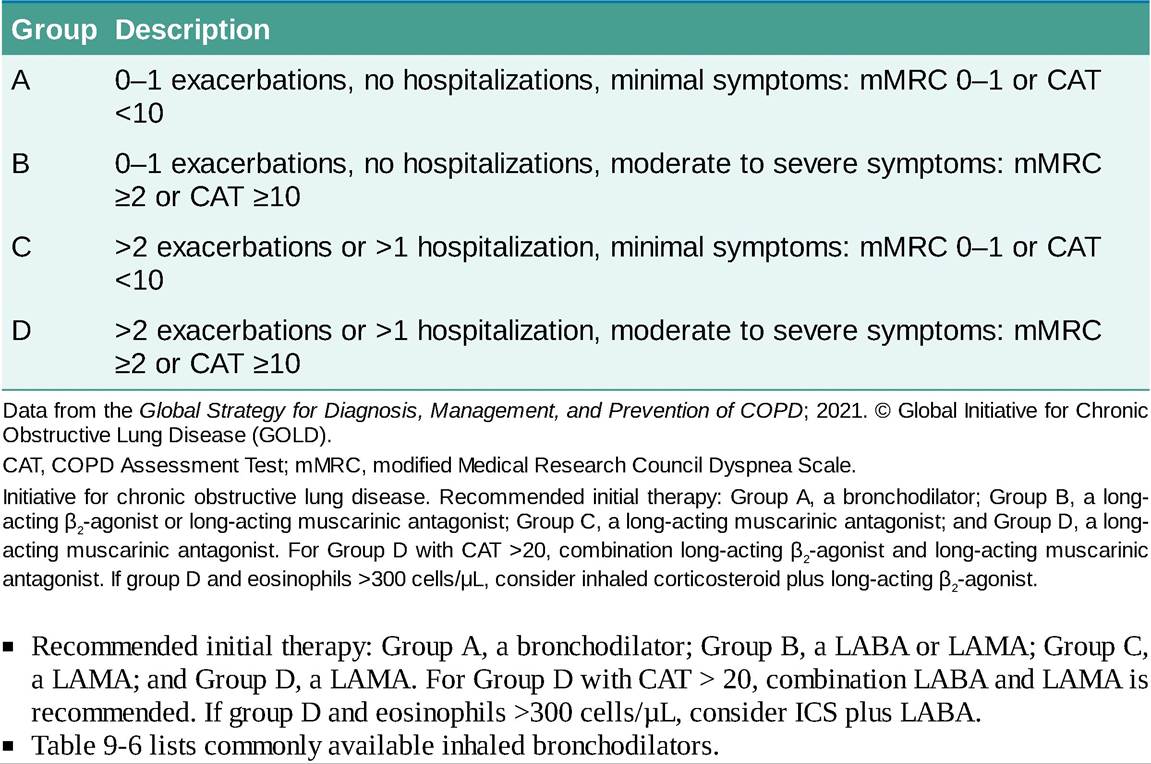
| 6 seconds) breath sounds on a maximal forced exhalation and decreased breath sounds. Expiratory wheezing and rhonchi may or may not be present. • Signs of pulmonary hypertension and right-sided heart failure may be present, and heart sounds may be muffled from the interposed hyperinflated lungs. • Clubbing is not a feature of COPD alone, so its presence should prompt an evaluation for other conditions, especially lung cancer. • Given the high incidence of cardiovascular comorbidities, an evaluation for signs of arrhythmias and decompensated heart failure is also paramount. Abnormalities of cardiac auscultation or significant lower extremity edema should trigger further investigation. Differential Diagnosis • Obesity hypoventilation syndrome is commonly misdiagnosed as COPD in patients admitted to the hospital with acute hypercapnic respiratory syndrome. • Debut presentation to the hospital with acute hypercapnic respiratory failure is common. In this scenario, pulmonary function tests (PFTs) are often not available and a careful evaluation of the clinical history, physical examination including bedside ultrasound, CT, and physiologic measurements while on mechanical ventilation (e.g., airway resistance, auto-PEEP [positive end-expiratory pressure]) can help narrow the differential diagnosis.9-11 On discharge, all such patients should be referred for PFTs. Diagnostic Testing Consider the diagnosis of COPD in any patient with chronic cough, dyspnea, or sputum production and a history of exposure to COPD risk factors, especially cigarette smoking. PULMONARY FUNCTION TESTING • A definitive diagnosis of COPD requires the presence of expiratory airflow limitation on postbronchodilator spirometry, measured using the FEV1∕FVC ratio, after 400 μg of albuterol is administered. Although a ratio of 0.7 is taken as the lower limit of normal for all adults, with advancing age, the ratio may decrease below 0.7 in individuals who are asymptomatic and have never smoked. Therefore, a reduced ratio should not be interpreted automatically as diagnostic of COPD. • The postbronchodilator FEV1 relative to the predicted normal defines the severity of expiratory airflow obstruction (Table 9-4) and is an independent predictor of COPD-associated mortality. TABLE 9-4 CLASSIFICATION OF SEVERITY OF AIRFLOW LIMITATION IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE (BASED ON POSTBRONCHODILATOR FEV1) In Patients With FEV1∕FVC 450 m. LABORATORY STUDIES • A baseline arterial blood gas (ABG) is recommended for patients with severe COPD to assess for the presence and severity of hypoxemia and hypercapnia. Annual monitoring may be considered. • Elevated venous bicarbonate may signify chronic hypercapnia. • Polycythemia may reflect a physiologic response to chronic hypoxemia and inadequate supplemental oxygen use. • Peripheral eosinophils >300 cells∕μL support the initial use of an inhaled corticosteroid (ICS). • A1AT levels: Because of its prognostic implications, unique set of comorbidities (e.g., liver disease), and the availability of A1AT replacement therapy, all COPD patients should be screened at least once for A1AT deficiency.12 IMAGING • CXRs are not sensitive for determining the presence of COPD, but they are useful for evaluating alternative diagnoses and to establish a baseline. • Chest CT without contrast can detect emphysema, changes in airway wall thickness, air trapping, and other conditions associated with tobacco smoking and COPD, such as lung cancer or atherosclerosis (see “Treatment” section). Symptomatic smokers with normal spirometry will often have CT abnormalities as listed above to explain their symptoms. • With increasing severity of COPD, patients often develop radiographic signs of thoracic hyperinflation, including flattening of the diaphragm, increased retrosternal∕retrocardiac air spaces, and lung hyperlucency with diminished vascular markings. Bullae may be visible. In severe disease, chest CT is used to determine candidacy for lung volume reduction surgery (LVRS) (see “Maximizing lung function” in “Treatment” section). TREATMENT • Long-term management of patients with COPD aims to improve quality of life, decrease the frequency and severity of acute exacerbations, slow the progression of disease, and prolong survival. These goals are pursued by decreasing exposures to noxious agents; maximizing lung function; maximizing/supplementing compensatory mechanisms; diagnosing and managing comorbidities; and implementing exacerbation prevention strategies. • Decreasing exposure to noxious agents ° Smoking cessation as detailed above (prevention). î Avoidance of biomass fuels at home and at work (e.g., avoiding the use of coal and wood to heat and cook). î Using personal protective equipment during activities that produce dust and fumes. î Improving ventilation and avoiding the use of caustic chemicals in home cleaning, hobbies, etc. • Maximizing lung function î Bronchodilators ■ The inhaled route maximizes drug levels in the airways and helps reduce systemic toxicities. ■ Inhaled bronchodilators work primarily by relaxing airway smooth muscle tone. This results in a reduction in expiratory airflow obstruction. Inhaled bronchodilators can be long-acting (e.g., muscarinic antagonists [LAMAs], β2-agonists [LABAs]) or short-acting (e.g., muscarinic antagonists and β2-agonists [SABAs]). ■ LAMAs and LABAs alone and in combination result in improvements in lung function, reductions in COPD exacerbations, and improvements in quality of life.13,14 However, they do not slow the rate of lung function decline and do not improve survival. î ICS ■ ICS are not recommended as monotherapy in COPD. Initial combination therapy with ICS/LABA can be considered in patients with peripheral eosinophil counts >300 cells∕μL.15 ■ ICS can be used in patients already on LAMA/LABA who have continued frequent COPD exacerbations, blood eosinophil counts >300 cells∕μL, or a history of asthma. ■ ICS withdrawal should be considered in patients with a history of Table 9-5. TABLE 9-5 REFINED ABCD ASSESSMENT TOOL FOR CHRONIC OBSTRUCTIVE LUNG DISEASE ![]()
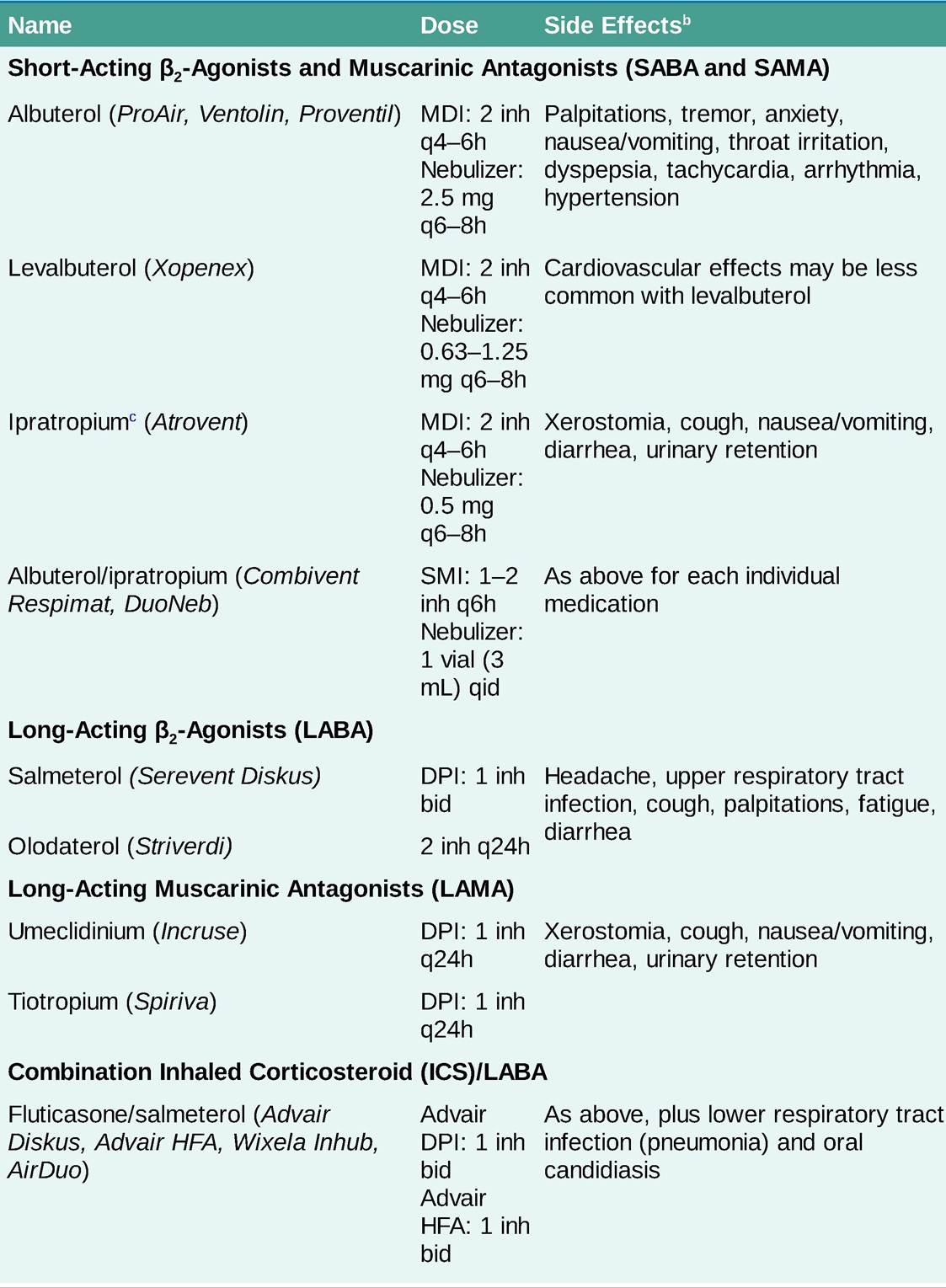
TABLE 9-6 ![]()
OBSTRUCTIVE PULMONARY DISEASEa ![]()
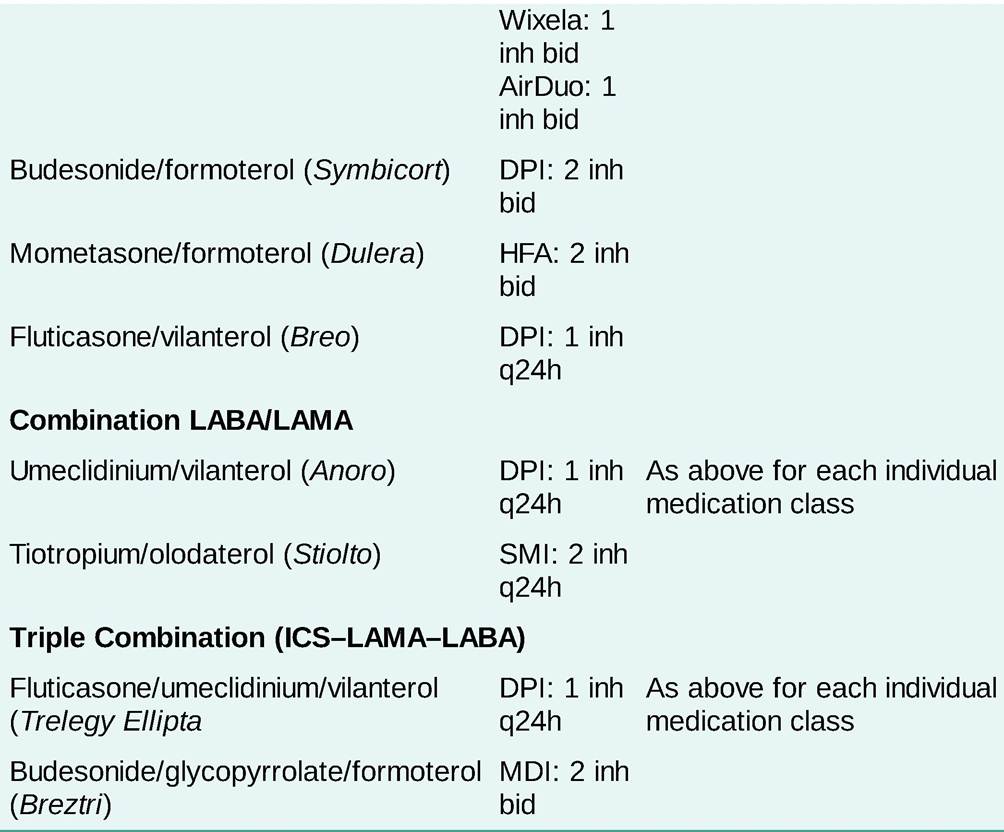
![]()
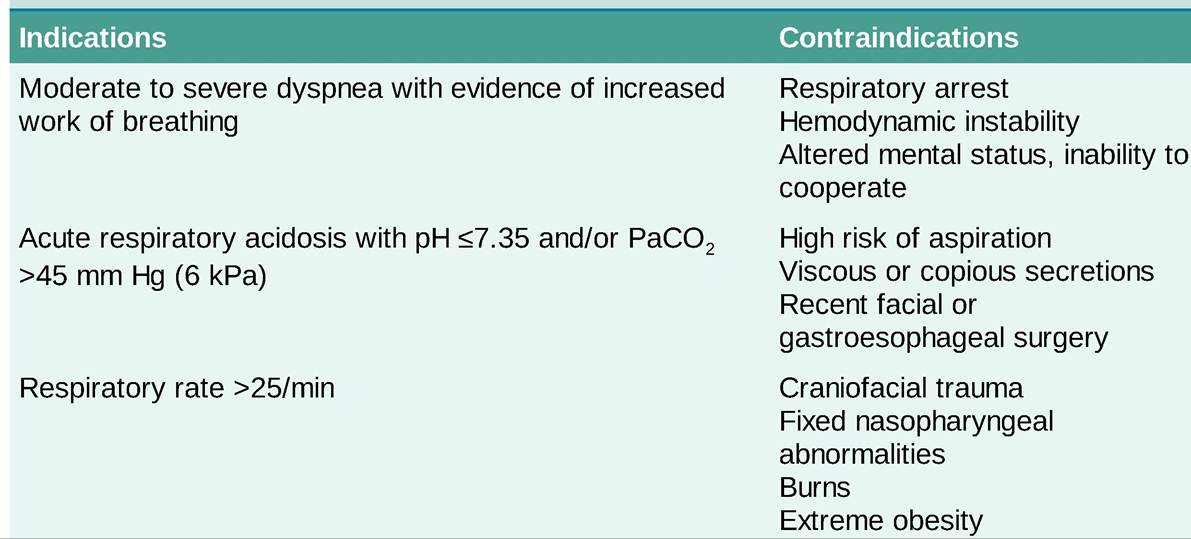
DPI, dry powder inhaler; inh, inhalation(s); MDI, metered-dose inhaler; SMI, soft mist inhaler. aTable is not exhaustive and only lists some commonly prescribed inhalers. Inhaled corticosteroid (ICS) monotherapy inhalers are listed in the “Asthma” section in Table 9-14. bOnly the most common side effects are listed. cShort-acting anticholinergic therapy (e.g., ipratropium) is usually discontinued with initiation of long-acting anticholinergic therapy (e.g., tiotropium), because minimal additional benefit is expected, side effects may increase, and use of two inhaled anticholinergic agents has had limited evaluation. ■ Providers should routinely assess a patient's inhaler technique and provide teaching. î Bronchoscopic and LVRS ■ In selected patients, LVRS or bronchoscopic lung volume reduction (such as using a one-way endobronchial valve) can improve FEV1, oxygenation, and functional outcomes. With these procedures, total thoracic lung volume is reduced, heathier lung is preferentially ventilated and perfused, and respiratory muscles may become more effective at ventilation. In a very carefully selected group of patients, LVRS may be associated with a survival benefit.17 î Lung transplantation ■ Lung transplantation in COPD is reserved for patients with advanced disease (BODE >7) and nonfatal comorbidities. Single and double lung transplant procedures can be performed in COPD with better long-term survival for double-lung transplantation.18 Transplantation is rare in patients older than 75 years. ■ Quality of life improves significantly for the vast majority of appropriately selected patients.19 ■ Median survival after transplantation is approximately 6 years. Importantly, survival is improved for some but not all patients with COPD after lung transplantation.20 • MaximizingZsupplementing compensatory mechanisms î Exercise training ■ When possible, exercise should be performed in the setting of a pulmonary rehabilitation program. ■ All patients being discharged from the hospital for a COPD exacerbation, at initial diagnosis, and prior to LVRS or lung transplantation should be referred to a pulmonary rehabilitation program. ■ Exercise training consists of aerobic exercise at 60%-80% of maximal exercise capacity. High intensity interval training can help achieve similar workloads in patients with limited mobility and exercise tolerance. Upper extremity strength training helps improve upper extremity specific task performance (e.g., laundry, doing dishes).21 î Supplemental oxygen ■ Oxygen supplementation improves survival and quality of life and reduces exacerbations. ■ The current indications for oxygen therapy in COPD are as follows: ? PaO2 ≤55 mm Hg or SpO2 ≤88% at rest. ? PaO2 56-59 mm Hg or SpO2 55%. ■ In patients with moderate resting desaturation (i.e., SpO2 89%-93%) or exercise-induced desaturation (i.e., SpO2 ≥ 80% for ≥5 minutes and 65 years or in younger patients in the presence of immunocompromising conditions or immunosuppression.29 ■ PCV13 and PPSV23 should not be administered during the same visit. ■ If both PCV13 and PPSV23 are to be administered, PCV13 should be administered first. ■ PCV13 and PPSV23 should be administered at least 1 year apart unless they are being administered to an immunocompromised patient in which case they can be administered 8 weeks apart.30 ■ COVID-19 vaccination is recommended to all patients with COPD.31 î Macrolide antibiotics (e.g., azithromycin 250 mg daily) ■ It may function as an anti-infective or direct anti-inflammatory in COPD. ■ In patients with previous exacerbations, the frequency of subsequent exacerbations is decreased by 19%; however, improvement in clinical symptoms was modest.32 ■ The benefit may be absent in current smokers and greater in older individuals (>65 years) and those with milder disease (FEV1 >50%). ■ Hearing loss in the absence of tinnitus was reported, suggesting routine monitoring with audiometry should be considered with chronic therapy. î Phosphodiesterase-4 inhibitors (e.g., roflumilast 500 μg daily) ■ The US Food and Drug Administration (FDA) approved for a relatively narrow indication of severe COPD (FEV1 65 years, comorbid conditions (especially cardiac disease), forced expiratory volume in 1 second (FEV1) should be guided by local resistance patterns, previous patient exposures, and severity of COPD. • Supplemental oxygen should be administered with a target oxygen saturation of 88%-92%. • Thromboprophylactic measures should be used given the increased risk of deep venous thrombosis in patients hospitalized for COPD exacerbations.37 • NIV (Table 9-8) should be considered the first mode of ventilator support as it reduces intubation rate, improves respiratory acidosis, decreases respiratory rate, and decreases hospital length of stay. TABLE 9-8 INDICATIONS AND CONTRAINDICATIONS FOR NONINVASIVE VENTILATION IN ACUTE EXACERBATIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE ![]()
Data from the Global Strategy for Diagnosis, Management, and Prevention of COPD; 2021. © Global Initiative for Chronic Obstructive Lung Disease (GOLD). • Endotracheal intubation and invasive mechanical ventilation are required in some patients (Table 99). TABLE 9-9 INDICATIONS FOR INVASIVE MECHANICAL VENTILATION IN ACUTE EXACERBATIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE Failure to improve with or not a candidate for noninvasive ventilation (see Table 9-8) Severe dyspnea with evidence of increased work of breathing Acute respiratory acidosis with pH 60 mm Hg (8 kPa) PaO2 35/min Coexisting conditions such as cardiovascular disease, metabolic abnormalities, sepsis, pneumonia, pulmonary embolism, pneumothorax, and large pleural effusion Data from the Global Strategy for Diagnosis, Management, and Prevention of COPD; 2021. © Global Initiative for Chronic Obstructive Lung Disease (GOLD). • Discharge criteria for patients with acute exacerbations of COPD include the need for inhaled bronchodilators less frequently than every 4 hours; clinical and ABG stability for at least 12-24 hours; the ability to eat, sleep, and ambulate fairly comfortably; adequate patient understanding of home therapy; and adequate home arrangements. Before discharging from the hospital, chronic therapy issues should be readdressed, including supplemental oxygen requirements, vaccinations, smoking cessation, assessment of inhaler technique, and referral to pulmonary rehabilitation.
More on the topic Chronic Obstructive Pulmonary Disease:
- Restrictive lung disease
- Macrovascular Complications of Diabetes Mellitus
- Chronic Allograft Dysfunction
- Emergent Airway Adjuncts
- 31 Urogynecology and Reconstructive Pelvic Surgery
- Respiratory Failure
- REFERENCES
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Interstitial Lung Disease
- Pelvic Mass
|