Anorectal anatomy
The anatomy of the rectum and anus cannot be studied in isolation. They form part of the pelvic organs and pass through the pelvic diaphragm along with the urethra and the vagina.
Injury to any part of the pelvic floor during childbirth may result in dysfunction of one or more pelvic floor organs.The pelvic diaphragm or levator ani is funnel- shaped and made up of four striated muscles: ileococcygeus, pubococcygeus, coccygeus, and puborectalis. The puborectalis forms a complete sling around the anorectal junction with some fibres blending with the wall of the anal canal. There is evidence that the puborectalis may be a distinct muscle in its own right as its innervations and histology is different from the rest of the levator ani (1). The nerve supply to the levator ani is S4 through the ventral ramus and the perineal branch of the pudendal nerve. The function of the puborectalis is to maintain the angle between the anal canal and rectum—this is important in maintaining continence.
Rectum
The rectum starts at the point where the sigmoid colon loses its mesentery, at the level of the mid sacrum. It is 12-15 cm long and becomes the anus as the tube passes through the pelvic floor. The rectum is covered with peritoneum at its front and sides in its upper third, only the front in its middle third, and not at all in the lower third. The rectum is an extremely distensible chamber and when it is empty the walls collapse—it usually remains empty until just before defecation. The rectum has a variable shape and follows the sacral curve with three lateral flexures and corresponding transverse folds within the rectum (or valves of Houston) (Figure 58.1). These valves are thought to support the weight of faecal matter until it is time to defecate. The blood supply of the rectum is a superior rectal branch from the inferior mesenteric artery and middle and inferior rectal arteries from the internal iliac artery.
The lymphatic drainage follows the arterial supply. The nerve supply of the rectum consists of a sympathetic component, which follows the branches of the superior rectal artery (from the coeliac plexus), and a parasympathetic supply, which is derived from the second, third, and fourth sacral segments of the spinal cord and passes through the pelvic splanchnic nerves.Anus
The anal canal is approximately 4- 4.5 cm long (2). The proximal 1 cm ofthe anal canal is lined by columnar epithelium extending down from the rectum. Below this the mucous membrane becomes cuboidal and the lining forms anal valves. Just below the level of the valves there is an abrupt transition to stratified squamous epithelium—the dentate or pectinate line. The squamous epithelium lining the next part of the anal canal is thin and shiny and has no hair or sweat glands. The final 0.5-1 cm of the canal is lined by hair-forming skin. The anal cushions sit in the upper part of the anal canal and help create an airtight seal. These are classically described as being in the 4, 7, and 11 o'clock positions. When these cushions become swollen and symptomatic, they are described as piles or haemorrhoids.
The anal canal is surrounded by muscles. The outermost layer of muscles is the external sphincter. This is a somatic voluntary (striated) muscle. Its nerve supply is S3 and S4 via the pudendal nerve and perineal branch of the fourth sacral nerve (3). It is important to remember that the motor fibres of the right and left pudendal nerves have overlapping distributions within the external anal sphincter so that stimulation of the right pudendal nerve causes circumferential contraction of the external anal sphincter. This has clinical implications as damage to one side may leave a functional sphincter but also implantation of a neurostimulator can be unilateral and still result in an improvement of whole anal function.
The longitudinal muscle is a direct continuation of the smooth muscle coat of the rectum, reinforced in its upper part by some striated muscle fibres originating from the levator ani muscle.
These fibres split into multiple end septa and insert into the skin of the lower part of the anal canal. They provide a supportive mesh but also provide pathways for spread of infection into and from the intersphincteric space. An infection with an intersphincteric gland can spread and when it reaches the skin this may form a fistula track.During defecation the longitudinal muscle contracts, resulting in evertion of the anal margin, shortening of the canal, and flattening out of the anal cushions, allowing the passageway to open for the passing of stool.
The internal sphincter represents the continuation and thickened circular muscle coat of the rectum. This is a non-striated involuntary muscle and is supplied by autonomic nerves.
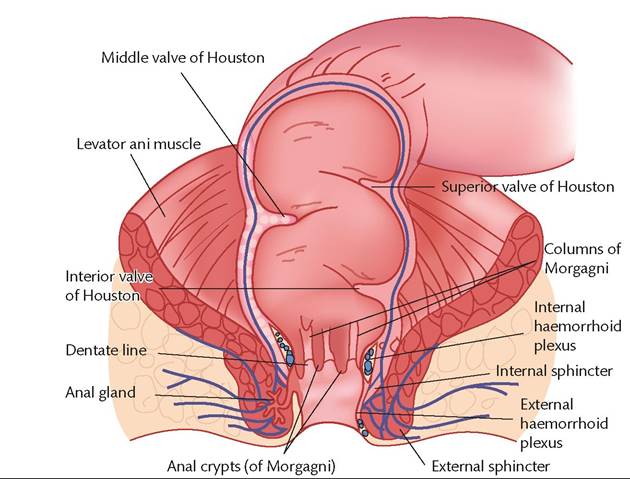
Figure 58.1 Anatomy of the anorectum and pelvic floor.
Anal glands may be found in the submucosa and intersphincteric space (there are normally between zero and ten glands). The glands drain via ducts into the anal sinuses at the level of the dentate line. They secrete mucin and it is thought that they lubricate the anal canal to ease defecation. When the drainage is blocked, abscesses can occur.