Anorectal physiology and function
The resting pressure of the anal canal should be high enough to maintain an air- and watertight seal during rest and activity. Penninckx et al. (4) estimated that the resting tone was generated by nerve- induced activity of the internal sphincter (45%), myogenic tone of the internal sphincter (10%), tone of the external sphincter (35%), and the anal cushions (15%).
These values are difficult to assess and are only estimates. The anal resting pressure is not constant during the day. It exhibits circadian variations and slow waves are seen when measuring the pressure using high-resolution anorectal manometry (HRAM) (Figure 58.2).When the rectum is distended there should be a compensatory relaxation of the internal sphincter muscle. This is known as the rectoanal inhibitory reflex and is mediated by intrinsic nerves as evidenced by the fact that the reflex remains after spinal cord transection. The reflex is probably mediated by nitric oxide and possibly by other non-adrenergic and non-cholinergic neurotransmitters. The reflex is absent in Hirschsprung’s disease.
The squeeze pressure is mediated by the external sphincter; it can be voluntary, induced by cough or an increase in intra-abdominal pressure, or by digitating the anal canal. At the time of defecation the external sphincter relaxes.
Puborectalis is tonically active and maintains the resting anorectal angle. Further contraction will occur in response to a sudden rise in abdominal pressure and this reduces the anorectal angle further and helps preserve continence.
Measurement
Anorectal physiology
The function of the anus and rectum can be measured using a variety of physiological tests. HRAM can be performed using water- perfused or solid-s tate catheters. The catheter provides a single pressure, averaged around the circumference at 6 mm intervals, and measures values along the entire length of the anal canal; it is also fitted with an inflatable balloon at the end.
Although attempts have been made to define normal resting and squeeze pressures there is considerable overlap between asymptomatic and symptomatic patients. Using HRAM it is possible to measure an average resting pressure, a maximum and sustained squeeze pressure, as well as examining the effect of attempting to expel a balloon filled with water. Rectal volume at first sensation, first urge, and maximum tolerated volume is usually assessed giving some indication as to whether a patient has a hypo-sensate or hyper-sensate rectum. Anal sensation is usually recorded and pudendal nerve latency can also be measured. Anorectal manometry can also be used to identify the very small minority of patients with Hirschsprung’s disease. These patients are usually diagnosed in childhood and it is rare to find a patient with Hirschsprung’s disease reaching adult life without a prior diagnosis. The rectoanal inhibitory reflex is absent in Hirschsprung’s disease. This reflex is elicited by placing the catheter into the anus and inflating a balloon within the rectum with air. There is a reflex decrease in the anal sphincter tone on inflation of the balloon. HRAM is also used in treatment; it is often used to start a biofeedback or retraining programme by showing a patient how to improve their squeeze pressure or method of defecation.Anal ultrasound
The structure of the anal canal can be visualized using threedimensional anal ultrasound (Figure 58.3). Ultrasound is useful, safe, and well tolerated by patients. Anal ultrasound is the preferred investigation to detect sphincter defects but insertion of the
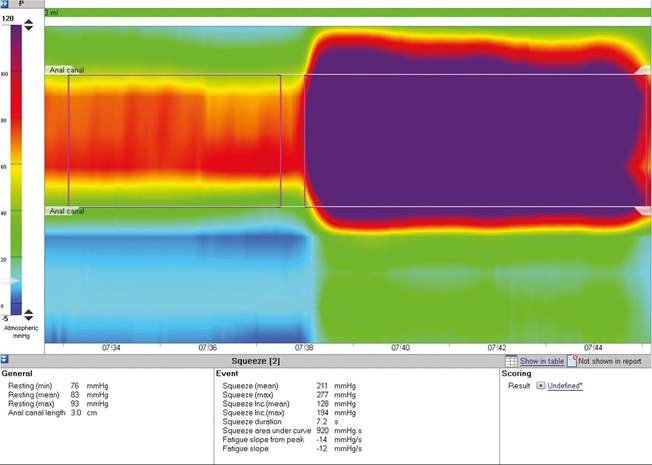
Figure 58.2 High -resolution anorectal manometry.
probe can distort the anal canal. Normal anal sphincter morphology and anal sphincter measurements can also be obtained using transvaginal and transperineal scanning (5).
Proctography
The dynamics of defecation can be assessed radiologically by evacuation proctography or magnetic resonance (MR) proctography (Figure 58.4).
These tests assess evacuation after paste or gel has been placed in the rectum to simulate a full rectum. Physiological filling of the rectum would normally occur at or around the time of colonic mass movements and these are not recreated in this laboratory setting. However, at present, these are the best tests available to look for an anatomical abnormality within the pelvic organs on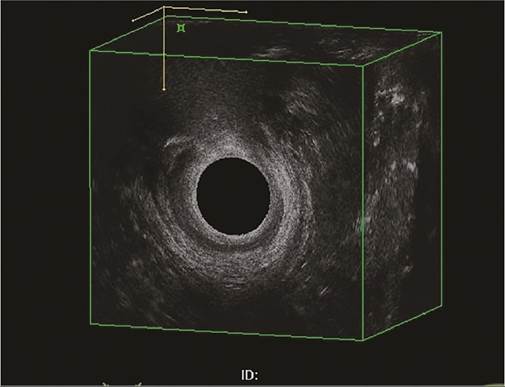
Figure 58.3 Three-dimensional anal ultrasonography showing a defect in the external sphincter.
straining. Fluoroscopic proctograms use rectal contrast and contrast may also be placed in the vagina, bladder, and small bowel, helping with better visualization of abnormalities such as an enterocele and rectocele. The patients are then fluoroscopically screened as they sit on the toilet and attempt to evacuate their rectum. MR defecography avoids radiation exposure and is better at visualizing bony landmarks. However, the patient is required to lie in the supine position and expel the gel onto a pad and this sometimes inhibits their normal defecatory push. This test visualizes the uterus, vagina, and anterior compartment as well as the rectum and any potential enterocele. A recent study suggested that MR proctograms may under-report pelvic floor abnormalities especially where there has been poor rectal evacuation (6).
Colon transit studies
The simplest way of studying a colon transit is ingesting a capsule of markers and taking a plain abdominal X-ray after 72 and then 120 hours. The distribution of the markers in the colon provides a crude measure of colonic transit. A normal study should show at least 80-90% of markers are eliminated by 120 hours in the majority of people. The markers have completely disappeared by this day. It is possible to use scintigraphic techniques to study both segmental colonic transit and small bowel transit and to give an idea of the flow of markers through the bowel. Some centres use three different-shaped markers on three different days and take further X-rays during the week.
More on the topic Anorectal physiology and function:
- Anorectal physiology and function
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020
- Pelvic floor, rectum, and anus
- Constipation and obstructive defecation
- Faecal incontinence
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Index