Pelvic floor, rectum, and anus
Pelvic floor
The pelvic floor comprises three muscle layers: the superficial perineal layer, which is innervated by the pudendal nerve; the urogenital diaphragm layer, which is also innervated by the pudendal nerve; and the pelvic diaphragm, which is innervated by the nerve roots S3-S5 (Box 3.3).
The position of these muscles is illustrated in Figure 3.4.Rectum
The rectum begins at the rectosigmoid junction at the level of the third vertebra. The calibre is similar to that of the sigmoid colon but near its termination it becomes dilated forming the rectal ampulla. It terminates at the dentate line to become the anus. The rectum is
Box 3.3 The pelvic floor muscle layers
Superficial perineal layer
• Bulbospongiosus (formerly bulbocavernosus)
• Ischiocavernosus
• Superficial transverse perineal
• External anal sphincter
Deep urogenital diaphragm layer
• Compressor urethra
• Urethrovaginal sphincter
• Deep transverse perineal
Pelvic diaphragm
• Levator ani: pubococcygeus (pubovaginalis), puborectalis, and iliococcygeus
• Coccygeus/ischiococcygeus
• Piriformis
• Obturator internus covered in its superior part by peritoneum. It lies posterior to the vagina, cervix, and corpus, forming a space called the pouch of Douglas. The pouch of Douglas is bordered by the rectum posteriorly, the vagina and cervix anteriorly, and the uterosacral ligaments on the lateral side. Distal to the fold of peritoneum in the pouch of Douglas, the rectum lies in close proximity to the vagina divided by a rectovaginal fascial plane. This plane corresponds to that named Denonvilliers' fascia in the male and sometimes this term is used to describe the rectovaginal fascia in women.
The superior rectal artery provides the chief blood supply to the rectum and is a continuation of the inferior mesenteric artery, which is a branch of the aorta.
Venous drainage is via the superior rectal vein that drains into the inferior mesenteric vein and the middle rectal vein that drains into the internal iliac vein. Lymphatic drainage is to the internal and external iliac nodes, as well as para-aortic nodes via the inferior mesenteric chain. The nerve supply to the rectum is via the rectal plexus that derives from the posterior part of the inferior hypogastric plexus. This provides sympathetic fibres to the vascular smooth muscle of the rectum and parasympathetic fibres to the smooth muscle of the rectum.Anus
The anal canal is the terminal part of the large intestine and extends from the rectum to the anal opening. The upper two-thirds of the anal canal are lined by columnar mucosa and contain longitudinal folds. The lower third is lined by squamous epithelium. Within this area is Hilton's white line, which marks the junction between keratinized stratified squamous epithelium and unkeratinized stratified squamous epithelium. The lower third is surrounded by folds, called anal valves. These valves converge at a line called the pectinate (dentate) line, which represents the embryological transition between the hindgut and the ectoderm, below which the mucosa becomes skin. This is subtly different to the ‘anal verge' which is the term used to define the transition between the epithelium of the anal canal and the perianal skin.
The upper two-thirds of the anus receives its arterial supply from the superior rectal artery, a branch of the inferior mesenteric artery, and the inferior third receives its supply from the inferior rectal artery, a branch of the internal pudendal artery which is a branch of the anterior division of the internal iliac artery (Box 3.4). Lymphatic drainage is via the internal and para-aortic chain of nodes above the pectinate line and to the superficial inguinal nodes below this. The upper two-thirds of the rectum are supplied by branches from the inferior hypogastric plexus.
In the lower third, the nerve supply is somatic, receiving its supply from the inferior rectal nerves, which are branches of the pudendal nerve. These are somatic and sensitive to temperature, touch, and pain.The anus is surrounded by the internal and external anal sphincters, which are two muscle rings that control defecation. The internal sphincter is about 3-4 cm in length and surrounds the anus. It is entirely involuntary and in a state of continuous contraction. Its nervous supply is from sympathetic fibres from the superior rectal and hypogastric plexuses which stimulate contraction. Inhibition of contraction of the internal sphincter is by parasympathetic fibres. The external anal sphincter is about 8- 10 cm long, elliptical in shape, and caudally lies close to the skin around the anus. It has a superficial and deep layer. The deep layer forms a complete circular sphincter
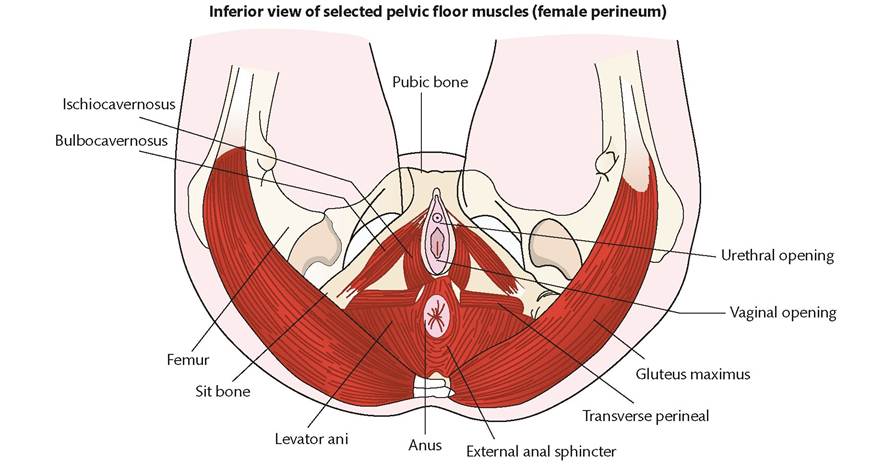
Figure 3.4 Anus and sphincter.
around the anus and lies next to the internal anal sphincter. Some fibres are shared with other muscles of the perineum. The superficial layer shares fibres with the transverse perineal, levator ani, and bulbospongiosus (formerly bulbocavernosus) muscles (Figure 3.4). Like the internal sphincter, the external sphincter is passively in a state of tonic contraction. It can be contracted further under the influence of the will, so as to further occlude the anus in expiratory efforts.
Clinical considerations
During radical hysterectomy, nerves from the hypogastric plexus are often divided. This can often leave the patient with permanent changes in bowel function. More recent techniques for performing radical hysterectomy are designed to try and preserve these nerve fibres by identifying them in a space deep to the uterosacral ligaments
Box 3.4 Arteries of the pelvis
External iliac artery
• Deep circumflex iliac artery
• Inferior epigastric artery
• Femoral artery
Internal iliac artery
Anterior division
• Inferior gluteal artery
• Middle rectal artery
• Obturator artery
• Inferior vesical artery
• Internal pudendal artery
• Uterine artery
• Umbilical artery
Posterior division
• Iliolumbar artery
• Lateral sacral artery
• Superior gluteal artery called Kobayashi’s space. Similar techniques have been employed to prevent damaging these nerves during sacrocolpopexy and other urogynaecological procedures.
Injury to the anal sphincters can occur during childbirth. Injury to the muscles of the sphincter are termed third-degree tears and those that enter the anus or rectum fourth-degree tears. These are described in more detail in Chapter 59.
More on the topic Pelvic floor, rectum, and anus:
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020
- Faecal incontinence
- Anorectal physiology and function
- Anatomy of the Female Pelvis
- Episiotomy
- Chapter 12 Reproduction