Blood supply to the pelvis
The main blood supply to the pelvis comes from the aorta via the two common iliac arteries and the ovarian artery. There is a further supply to the rectum via the inferior mesenteric artery (a branch of the aorta).
The ovarian arteries emerge from the aorta b elow the renal arteries and descend into the pelvis entering the infundibulopelvic ligament. Branches are given off to the Fallopian tubes and anastomoses occur with the uterine blood supply originating from the internal iliac artery. Venous drainage from the ovary is also via a network of vessels, but predominantly through the ovarian vein that drains into the inferior vena cava on the right and renal vein on the left.
The common iliac arteries divide at the level of the pelvic brim into the external and internal iliac arteries (Figure 3.5). The external iliac artery passes down the brim of the pelvis above the external iliac vein and becomes the femoral artery once it passes under the inguinal ligament. Before this, it gives off two branches: the deep circumflex iliac artery that travels along the pelvic brim and the inferior epigastric artery that passes upwards on the anterior abdominal wall and anastomoses with the superior epigastric artery (Box 3.4). The first two branches supply the skin and muscles of the anterior abdominal wall and the femoral artery supplies the leg.
The internal iliac artery is classically described as having an anterior and posterior division (Figure 3.5 and Box 3.4). The posterior division gives off three branches classically described in a mnemonic
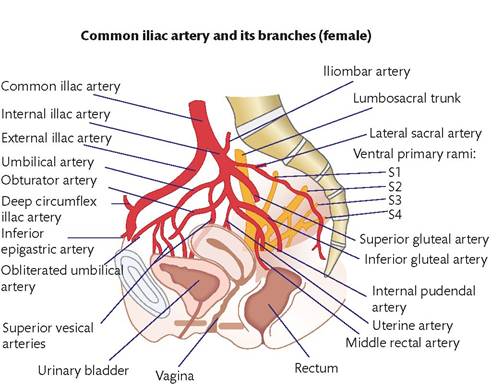
Figure 3.5 Blood supply to the pelvis.
as PILS (Posterior division, Iliolumbar, Lateral sacral, and Superior gluteal) (Box 3.4). The iliolumbar artery has an iliac and lumbar branches and the lateral sacral often has a superior and inferior branch.
There are multiple anastomoses between these vessels that supply the posterior compartment of the pelvis and gluteal muscles (Figure 3.5 and Box 3.4). The anterior division gives off a number of branches that supply the uterus, vagina, bladder, and perineum (Box 3.4). The uterine artery passes over the ureter before dividing and providing a superior and inferior branch. This is classically described as ‘water under the bridge' as the ureter passes under the uterine artery.Blood vessels in the pelvis all have numerous anastomoses. The venous drainage often corresponds to the arterial supply but a large venous plexus of anastomoses exists in the pelvis, from which blood drains into named vessels.
Clinical considerations
The most important clinical considerations with relation to blood vessels in the pelvis involve surgical ligation and avoidance of non- intentional damage. Knowledge of the arterial supply and venous drainage allows a surgeon to resect structures (such as the uterus) without haemorrhage. The multiple anastomoses and venous plexuses mean that surgical haemorrhage can be quite profuse and numerous surgical techniques can be used to control unintentional bleeding. Ligating the internal iliac arteries often controls profuse bleeding from the uterus during a caesarean section. This is normally done at a level below the posterior division (see Chapter 29).
Individual arterial branches can be identified radiologically and embolized. This can be done to control haemorrhage or to devascularize a structure such as in uterine artery embolization for the management of fibroids (see Chapter 49).