Basic principles of newborn care
Healthy babies need only simple measures to promote the natural process of transition from fetal to postnatal life. Following birth, all babies should undergo a rapid assessment of their well-being and need for resuscitation.
Other basic principles encompass thermoregulation, cleanliness, breastfeeding, and ability to recognize the sick and at-risk newborn baby.Cord clamping
The optimal timing of cord clamping (early vs late) continues to fuel considerable debate. Precise definitions of what constitutes early and delayed cord clamping are also uncertain in both routine clinical practice and in the literature. Recent systematic review data indicate no differences in maternal outcomes (maternal death, maternal morbidity, or postpartum haemorrhage). Potential benefits for term-born infants include increased haemoglobin in the first 2448 hours (mean difference 1.49 g/dL; 95% CI 1.21-1.78 g/dL) and a lower incidence of iron deficiency anaemia (RR 2.65 for the delayed cord clamping groups). No significant differences have been identified between the groups with respect to neonatal mortality (RR 0.37; 95% CI 0.04-3.41) or neonatal unit admission. There is, however, an increased requirement for phototherapy in the late cord clamping groups (RR 1.62; 95% CI 1.41-1.96) (41). This latter consequence is of particular relevance in settings where the incidence of neonatal jaundice is high, and phototherapy may not be readily available. In preterm infants, systematic review data indicate a reduction in anaemia (RR 0.61; 95% CI 0.46-0.81), periventricular haemorrhage (RR 0.59; 95% CI 0.41-0.85) and necrotizing enterocolitis (RR 0.62; 95% CI 0.43-0.90) (42). Other short-term benefits include improved urine output, reduction in hypotension, and improved cardiac function (43). There are limited data on the long-term effects of differing cord clamping regimens but follow- up data from a Swedish randomized controlled trial show delayed cord clamping to be beneficial to fine motor and social skills at 4 years of age (44).
Given the available evidence, and to date, the absence of harm, it is reasonable to wait for least a minute before clamping the cord if the baby appears vigorous after delivery. For babies that are in need of newborn resuscitation, the results of considerable ongoing research effort will provide greater insight into the possible benefits of resuscitation prior to cord clamping.Birth into a clean environment
Newborn infection is one of a triad of problems (with birth asphyxia and prematurity) that are the principal contributors to global neonatal mortality (45). Newborn infection has a high case fatality rate and is thought to account for approximately one-third of neonatal deaths (46). Neonatal sepsis usually presents with non-specific clinical signs (Table 37.4) (47) and can
| Potential indicators of neonatal sepsis | Comments |
| Altered behaviour/reduced responsiveness | Healthy term newborn babies should wake for feeds |
| Feeding difficulties | Lack of interest in breast- or bottle-feeding especially when combined with other signs listed may be a cause for concern |
| Abnormal heart rate | Tachycardia: heart rate >160 beats per minute Bradycardia: heart rate >60 beats per minute (this may be normal in a sleeping term baby) |
| Signs of respiratory distress | Tachypnoea, grunting, intercostal recession, subcostal recession, nasal flaring, head bobbing, cyanosis |
| Seizures | This should prompt investigations and treatment for neonatal central nervous system infection |
| Temperature instability | Hypothermia: 38°C |
| Signs of shock | Capillary refill time >3 seconds, poor urine output, metabolic acidosis |
| Glucose instability | Healthy term infants have a physiological drop in blood glucose following birth and should not have routine measurement of their blood glucose. However, if a newborn is noted to be hypoglycaemic, this may be a sign of sepsis |
| Jaundice within 24 hours of birth | Jaundice within the first 24 hours of life should always be considered pathological |
| Evidence of local infection (e.g. skin/eye) | Purulent conjunctivitis/eyelid swelling in the first 24 hours should prompt consideration of a diagnosis of Neisseria gonorrhoeae conjunctivitis |
Source data from National Institute of Health and Care Excellence (NICE). Neonatal Infection (Early Onset): Antibiotics for Prevention and Treatment. Clinical guideline [CG149]. https://www.nice.org.uk/guidance/CG149 (accessed 15 July 2016).

be difficult to treat, especially in low-resource settings where antimicrobials may not be readily available and where antimicrobial resistance is a growing and serious problem. Careful attention should be paid to simple and inexpensive preventive measures, chief among which are scrupulous hand and umbilical cord hygiene. Practitioners should wash their hands or use alcohol hand gels, and utilize the World Health Organization (WHO) ‘My five moments of hand hygiene' tool (48). The umbilical cord should be cut with a sterile instrument and then either clamped with a clean device or tied with clean material and allowed to dry and separate naturally by exposure to air. The cord should be kept clean with sterile water until separation occurs. In parts of the world with high rates of newborn infection, current WHO guidance is to recommend ‘dry' cord care, though use of topical antiseptics (e.g. chlorhexidine) may also be considered (49). Recent systematic review evidence supports the practice of ‘dry' cord care in the hospital setting but also suggests topical antiseptic application of 4% chlorhexidine may be of benefit in home births in low-resource settings (50, 51).
Implementation of these simple but highly effective practices requires strong leadership, regular audit of compliance by all healthcare professionals, and access to clean water, soap, and towels.Resuscitation
All healthcare professional attending a birth should have basic training in newborn resuscitation. This advice extends to obstetric, midwifery, and anaesthetic staff as the need for newborn resuscitation is often unpredictable. Attendance at a recognized neonatal resuscitation training course along with regular multidisciplinary ‘skill drills' to ensure ongoing competence is recommended best practice.
Resuscitation equipment should be checked at regular intervals. At birth, the baby should be assessed in accordance with country specific and local guidelines, an example of which is provided in Figure 37.1 (52). The use of 100% oxygen in neonatal resuscitation of term babies was long considered best practice until research showing this resulted in a 30% increase in neonatal mortality in comparison with resuscitation with air (53). These clinical trials changed neonatal resuscitation guidelines around the world. Room air is now considered the optimal starting gas for the resuscitation of the term baby. Where required, oxygen use should be carefully titrated and ideally utilized with parallel monitoring of oxygen saturation levels to detect both hyperoxia and hypoxia. Though initially considered controversial, this has been accepted into standard practice.
Meconium-stained liquor
The aspiration of meconium into the lungs takes place before delivery and is usually associated with advanced gestational age. The passage of meconium in the preterm infant has historically been associated with maternal and/or congenital infection with Listeria monocytogenes but this is not borne out by retrospective case-control studies (54). There are good quality randomized clinical trial data demonstrating no evidence of benefit to the newborn from oropharyngeal suction of the airway prior to delivery of the shoulders (55) and routine intubation of the vigorous infant born through meconium (56), hence these practices are no longer recommended.
If a baby born through meconium is not breathing and/or has a low heart rate, then inspection of the oropharynx under direct vision using a laryngoscope, with suctioning of any particulate matter obstructing the airway is recommended, following which resuscitation should proceed along usual lines as outlined in Figure 37.1. It is recommended that either a large-bore suction catheter or a meconium aspirator device is used if the newborn airway is thought obstructed with potentially thick particulate matter such as meconium, blood, amniotic fluid, or vernix. The newborn should then be observed (usually for 12-24 hours) according to a locally agreed policy to monitor for clinical signs of meconium aspiration syndrome, which usually presents with respiratory distress.Thermoregulation
Newborn babies are born with wet skin and have a high surface area- to-weight ratio. They are susceptible to heat loss through the well- described mechanisms of evaporation, conduction, convection, and radiation and so can become hypothermic quickly if attention is not paid to thermoregulation. Every gram of water lost through evaporation results in 0.6 kcal of heat loss (57). Evaporative heat loss is magnified in preterm infants by virtue of their skin immaturity through transepidermal water loss and so these infants require even more attention to their early thermal environment. Hypothermia is associated with increased morbidity and mortality and so measures to actively prevent this are key components of good perinatal care (58). Thermoregulation requirements should be considered by obstetric
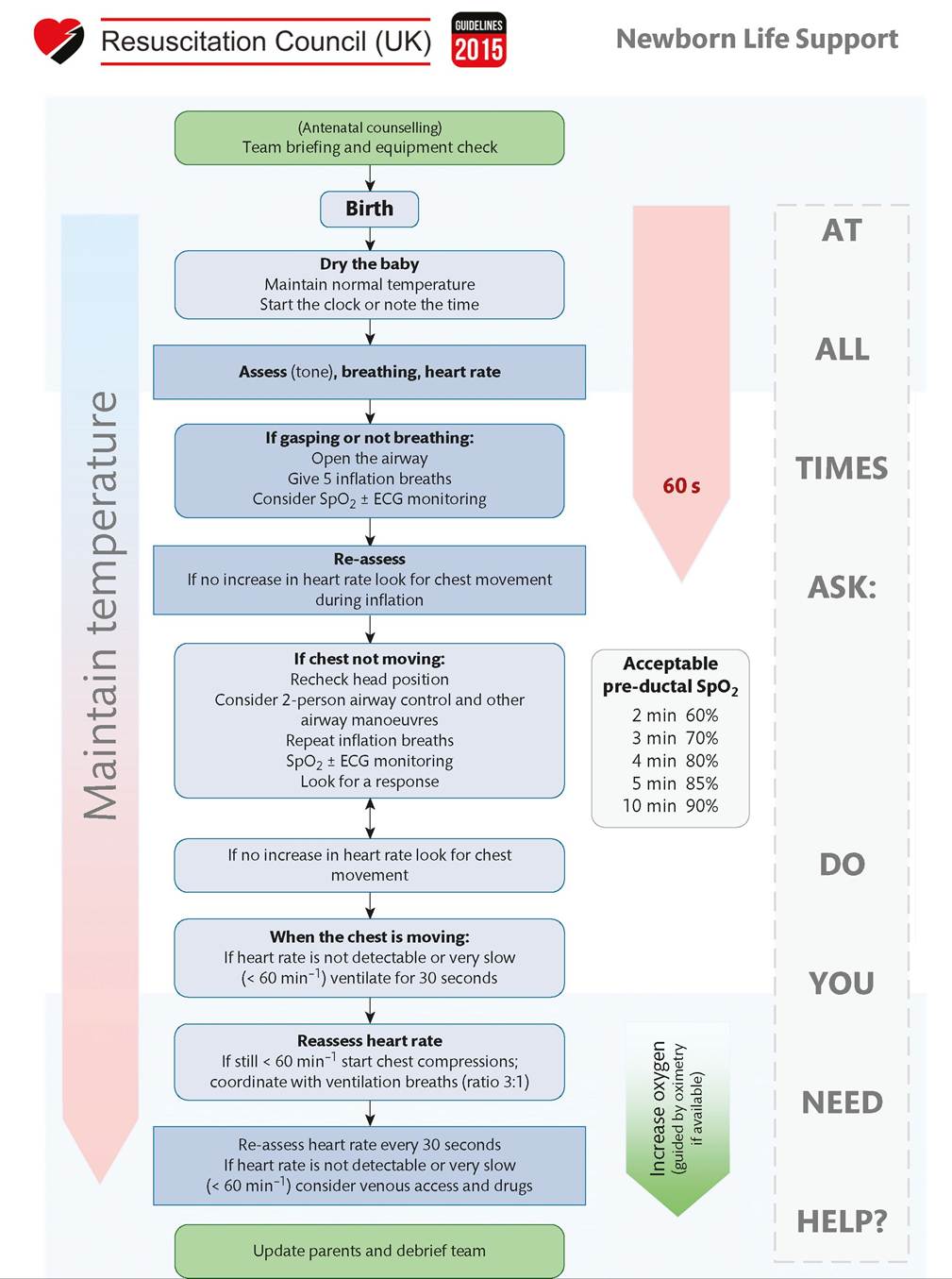
Figure 37.1 UK Resuscitation Council Newborn Life Support Guidance. Reproduced with the kind permission of the Resuscitation Council (UK) https://www.resus.org.uk/resuscitation-guidelines/.
teams prior to delivery in the same way as the need for neonatal team attendance at high-risk deliveries.
The delivery environment (including theatre) should be warm (26°C is recommended), with windows closed and draughts prevented (59). Following birth, a healthy baby should be dried, placed prone on the bare chest of the mother for direct skin-to-skin contact (60) and covered with a warm towel. A hat should be placed on the baby's head as the head is a major source of heat loss in newborn infants. Assessment of wellbeing by the birth attendant can take place during skin-to-skin contact. If resuscitation is anticipated or required, the first step should be to dry the baby with a warm towel. Once dried, the baby should be wrapped in a fresh warm towel and a hat placed on the head. Preterm infants may also benefit from early skin-t o-skin contact especially in low-income settings (61). Systematic review evidence supports the practice of delivery of preterm infants into a plastic bag without drying as a strategy to reduce hypothermia (21-46% reduction in hypothermia defined as a temperature distress is important to recognize as it can be a sign of several different newborn pathologies including systemic infection, pneumonia, surfactant deficiency lung disease (respiratory distress syndrome), meconium aspiration syndrome, pulmonary air leak, congenital diaphragmatic hernia, and congenital heart disease. Signs of respiratory distress include tachypnoea (defined as a respiratory rate of >60 breaths per minute), intercostal recession, subcostal recession, grunting, nasal flaring, and head bobbing. Babies that display any of these clinical signs need an urgent medical assessment including measurement of oxygen saturation and continued regular observation of heart rate, respiratory status, and temperature. Treatment with intravenous antibiotics is usually indicated pending identification of the underlying cause.Jaundice
Approximately 50-80% of healthy newborn infants will develop visible jaundice. In the majority of infants, jaundice is physiological, occurring due to an increased red cell mass, increased red cell turnover, and hepatic immaturity. Physiological jaundice tends to appear at around 2-3 days, peaks by 5 days, and resolves by 7-10 days of life. Jaundice should be considered pathological until proven otherwise if it is apparent early (within 24 hours of birth), is severe, rises rapidly (>18 μmol∕L∕hour), or is prolonged (beyond 14 days in term infants and beyond 21 days in preterm infants). Serum or plasma bilirubin levels should be measured or checked using a non-invasive transcutaneous bilirubinometer (not recommended in the first 24 hours, in preterm infants 20 mmol/L or >20-25% of total serum bilirubin value), pale stools, and dark urine; there may also be evidence of liver dysfunction (e.g. elevated alkaline phosphatase and/or alanine transaminase). The possibility of obstructive jaundice requires immediate assessment and investigation with referral to a specialist paediatric
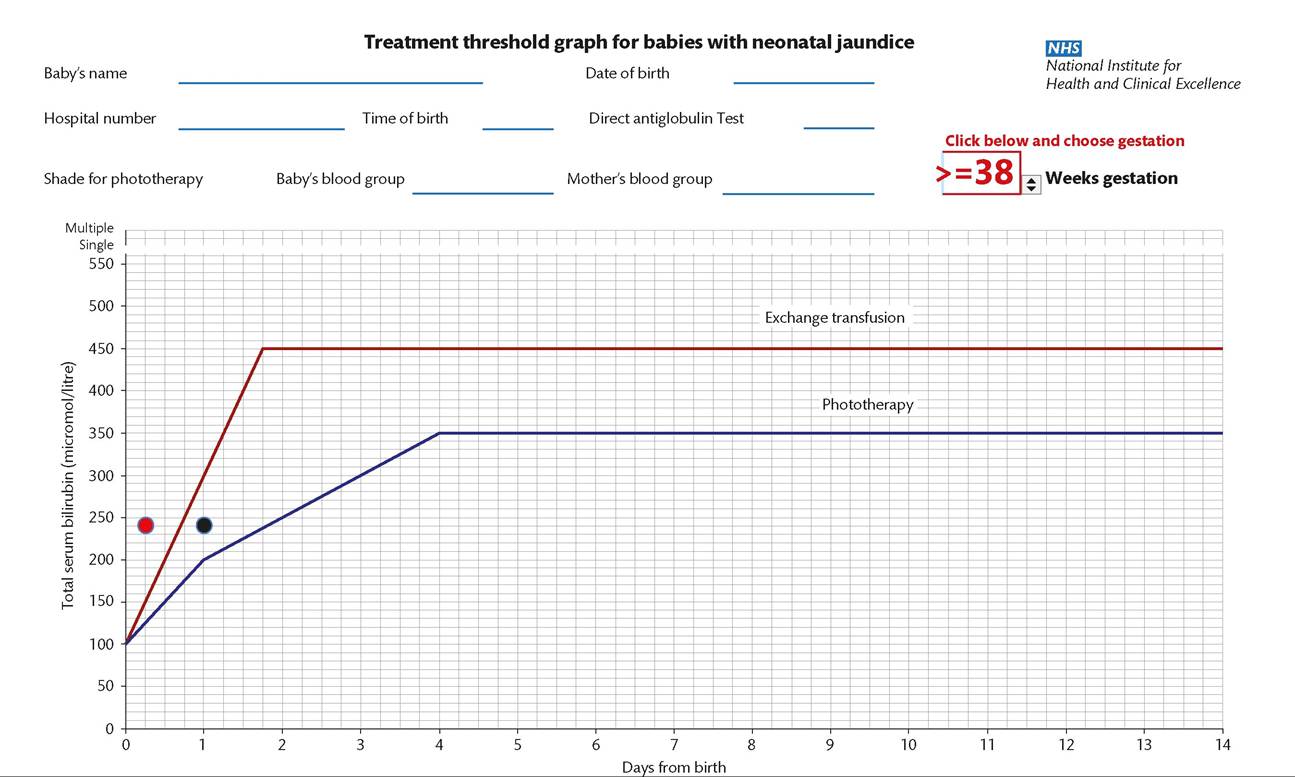
Figure 37.2 Treatment threshold graph for babies with neonatal jaundice. The blue line indicates the total serum bilirubin level at which phototherapy is indicated. The red line indicates the total serum bilirubin at which a double-volume exchange transfusion might be considered. Forexample, a 38 weeks'gestation newborn Infantwith a total serum bilirubin of 240 μmol∕Lat 24 hours of age (indicated by the black circle on the graph above) would require Ireatmentwith phototherapy. A similar total serum bilirubin value at 6 hours of age (indicated by the red circle) may require an urgent double-volume exchange transfusion.
Source data from National Institute for Health and Care Excellence (NICE). Neonatal Jaundice. Clinical guideline [CG9s:]. London: NICE: 2010. https://www.nice.org.ulCguidanceZcgOt:.
SECTION 4 Neonatal Careand Neonatal Problems
liver unit if confirmed (69). There are several potential underlying diagnoses including neonatal sepsis, metabolic conditions, neonatal hepatitis, choledochal cysts, and biliary atresia. Biliary atresia occurs in two forms, syndromic (10-20% of cases) and acquired (80-90% of cases). Though variable in severity, the condition classically presents with conjugated jaundice, pale stools, dark urine, failure to thrive, and hepatomegaly (70). Immediate referral to a specialist liver unit is warranted if biliary atresia is suspected as early surgical treatment (As a general principle, it is recommended that initial antimicrobial therapy be broad spectrum but should be narrow spectrum once the pathogen has been identified. Strict antibiotic discipline is an important means of reducing antimicrobial resistance; this includes facility-based guidelines to ensure that use is consistent and limited to a small range of antibiotics, reserving the use of other antibiotics to specific situations under senior supervision, and stopping antibiotics promptly (usually at 36-48 hours) after initiation for suspected sepsis if the baby is well, and blood cultures are negative. The need for a lumbar puncture to obtain cerebrospinal fluid to diagnose neonatal meningitis should be based upon clinical evaluation first and foremost. The practice of performing routine lumbar punctures in newborns as part of a sepsis workup is not recommended (74).
Poor feeding
The assessment of a baby with poor feeding requires knowledge and experience. Poor feeding can be a sign of an unwell newborn even though specificity is low. Several tools exist to provide mothers and healthcare professionals with indications that infant feeding is progressing well. As a general rule, healthy term babies will take more than eight feeds in a 24- hour period, suckle for between 5-40 minutes, be calm during feeding and contented afterwards, and will have one or two wet nappies and pass meconium within the first 24 hours (75). A common misconception is that the healthy full-term baby who appears to want to suckle frequently in the first 2-3 days before maternal lactation is established is ‘hungry’ and ‘not getting enough’. Healthy term babies require only such colostrum as is available, and will initially suckle at varying frequencies. After a mother’s milk has ‘come in’, a more regular pattern is usually established over the subsequent days. It is important that all healthcare professionals contributing to the care of mothers and babies understand normal postnatal lactation physiology and infant behaviour and are able to provide consistent advice and reassurance if appropriate. Failure to do so may undermine the confidence of a first-time mother and lead her to opt for formula feeding. Every effort should be made to actively promote breastfeeding and this is an important performance metric for perinatal teams.
In the case of a baby who is believed to be feeding poorly, a careful history from the mother and the midwifery or birth attendant staff, observing a feed, and examination of the baby are all essential. A sick baby will not feed well, and feeding may also reflect problems such as an unrecognized cleft palate, genetic syndromes (e.g. unrecognized aneuploidies), infection, and other acute conditions.
Healthy term babies will normally lose 1-2% of their birth weight in the first few postnatal days and regain this by around 7-10 days. Weight loss of greater that 10-15% may be indicative of poor feeding and result in hypernatraemic dehydration. Observation of changing stool colour can also be used as a way of assessing adequacy of feeding. Regular stooling and more than three wet nappies within a 24-hour period are reassuring signs. A healthy, well-fed term baby will pass meconium within the first 24-48 postnatal hours. After this, the stool of a breastfed baby will change to becoming ‘transitional’ in nature, and then to the characteristic fragrant, soft yellow, seedy appearance.
Bilious vomiting
Bilious vomiting in both term and preterm infants is of concern to the neonatologist as this may indicate a number of underlying medical and surgical pathologies resulting in functional (ileus) or anatomical obstruction (Table 37.5). Any baby with bilious vomiting should undergo an urgent medical review to establish the history (antenatal scans and presence of polyhydramnios, family history, passage of meconium, feeding history) and assess well-being. Clinical examination should focus upon whether the abdomen is distended, the anus is patent, and signs of systemic illness. General principles of management include placing the infant nil by mouth, passage of a large- bore nasogastric tube on free drainage, and admission to the neonatal unit. Nasogastric losses in excess of 20 mL/kg/ day should be replaced millilitre for millilitre from a 500 mL bag of
Table 37.5 Potential causes of bilious vomiting in newborn infants
| Potential causes of bilious vomiting | Comments |
| Neonatal infection | Associated with a functional gut ileus. Review history for risk factors Serial review of newborn for evolving clinical signs of infection |
| High gastrointestinal obstruction (duodenal atresia, jejunal atresia, ileal atresia) | Treat newborn with nil by mouth, large-bore nasogastric tube on free drainage, and intravenous antibiotics. Obtain abdominal X-ray. Review antenatal history for known associations (polyhydramnios, requires paediatric surgical referral) |
| Malrotation and midgut volvulus | Treat newborn with nil by mouth, large-bore nasogastric tube on free drainage, and intravenous antibiotics. Obtain abdominal X ray. Monitor acid-base balance Requires urgent paediatric surgical referral (time critical because of potential for extensive bowel necrosis) |
| Necrotizing enterocolitis (consider especially in preterm infants) | More likely in preterm infants. Term infants with necrotizing enterocolitis should raise the suspicion of congenital heart disease (76) Treat newborn with nil by mouth, large-bore nasogastric tube on free drainage and intravenous antibiotics. Obtain abdominal X-ray Monitor cardiorespiratory status and acid-base balance If worsening clinical status and/or non-response to medical therapy, requires urgent paediatric surgical referral (time critical because of potential for extensive bowel necrosis) |
| Meconium ileus | Associated with delayed passage of meconium May be a presentation of cystic fibrosis Treat newborn with nil by mouth, large- bore nasogastric tube on free drainage, and intravenous antibiotics. Obtain abdominal X ray Requires paediatric surgical referral |
Source data from National Institute of Clinical Excellence Guideline CG149 https:// www.nice.org.uk/guidance/CG149 (accessed 15/07/2016)
Box 37.2 Potential causes of neonatal encephalopathy
• Hypoxic ischaemic encephalopathy (perinatal asphyxia encephalopathy)
• Perinatal stroke
• Perinatal/congenital central nervous system infection (e.g. herpes encephalitis)
• Structural/developmental brain anomalies (e.g. cortical dysplasia)
• Neurometabolic conditions (e.g. Zellweger syndrome, neonatal adrenoleucodystrophy, and non-ketotic hyperglycinaemia)
• Genetic syndromes (e.g. Walker-Warburg syndrome)
• Mitochondrial disorders
• Neuromuscular disorder (e.g. congenital myotonic dystrophy and nemaline rod myopathy)
• Antenatal maternal trauma
presentation of these different causes may share features in common such as fetal distress (e.g. abnormal cardiotocography (CTG) trace, meconium-stained liquor, abnormal cord pH) and need for resuscitation at birth, emphasizing the importance of obtaining a careful history (Table 37.6), examining the newborn and placenta, and carrying out other investigations to help establish the cause. The term hypoxic-ischaemic encephalopathy or birth asphyxia should be reserved for specific cases of neonatal encephalopathy where there is good evidence that the infant has sustained an asphyxial insult likely to have led to impaired cerebral perfusion.
Infants with neonatal encephalopathy may require a multitude of investigations including tests to exclude central nervous system infection, and identify possible underlying genetic, metabolic, structural, or developmental brain anomalies. The placenta and membranes should be sent for histopathological and microbiological analysis. It is important for parents and healthcare professionals that all cases of neonatal encephalopathy have careful documentation of the history, investigations including venous and arterial cord blood gases,
0.9% saline containing 10 mmol of potassium chloride. Imaging (abdominal radiography) and relevant blood tests are first-line investigations followed by gastrointestinal contrast series in discussion with the neonatal surgical team.
Neonatal encephalopathy
This is a clinical syndrome manifest in the early postnatal period comprising disturbed neurological function in term/near-term newborn babies. The features are altered consciousness, and abnormalities of tone; there may be seizures, and apnoeic episodes (77). The initial description of neonatal encephalopathy by Sarnat classified babies into three stages (Sarnat 1, 2, or 3). Sarnat stage 1 is characterized by a duration of less than 24 hours, hyperalertness, uninhibited Moro reflex, and a normal electroencephalogram. Sarnat stage 2 infants are obtunded, hypotonic, with distal limb flexion and clinical seizures. Sarnat stage 3 infants are stuperose, flaccid with absent Moro and suck reflexes, and an abnormal electroencephalogram. Stage 1 generally has a good prognosis with normal development; approximately 25% of stage 2 Sarnat cases develop later neurological problems; stage 3 infants have a very high rates death and cerebral palsy (78). There are many possible causes of neonatal encephalopathy (Box 37.2). The
Table 37.6 Neonatal encephalopathy: important information for the neonatologist
| Neonatal encephalopathy | Comments |
| Antenatal serology | May indicate congenital infection |
| Maternal medical history, e.g. thrombophilia and medications during pregnancy | Maternal thrombophilia can be associated with neonatal stroke |
| First-trimester screening results | May indicate aneuploidy |
| Antenatal scan or liquor volume abnormalities | Polyhydramnios may indicate neurological/neuromuscular problem in newborn |
| Decreased fetal movements/ abnormal fetal movements | May indicate antenatal origin/may indicate fetal seizure activity |
| Antenatal maternal trauma | May suggest a sentinel causative event |
| CTG trace | Provides evidence of fetal distress |
| Cord blood gas result | Provides evidence of fetal distress |
| Consanguinity | May be indicative of a rare autosomal recessive disorder in newborn |
| Family history | May suggest inherited condition |
| Delivery | Mode of delivery, shoulder dystocia, instrumentation, prolonged second stage |
and sequential clinical findings on daily newborn examination. The baby must receive long-term neuro developmental surveillance. Multidisciplinary discussion of cases of neonatal encephalopathy can help identify the cause, and promote shared learning.
Therapeutic hypothermia is now a standard of care in most high- income countries for babies older than 36 weeks' gestation who have evidence of moderate to severe perinatal hypoxic-ischaemic encephalopathy. This involves either whole body or head cooling within 6 hours of birth to 33-34°C for 72 hours. The intervention reduces cerebral palsy by approximately 33% at 18 months of age (79). Reassuringly, follow-up data into middle childhood demonstrate persistence of a beneficial effect with respect to higher IQ, reduced cerebral palsy, and less requirement for special educational resources (80). As is common with any emerging evidence-based intervention, many uncertainties remain; examples include whether benefit extends to preterm infants, other causes of neonatal encephalopathy (e.g. perinatal stroke), lesser degrees of compromise, and hypoxic- ischaemic encephalopathy in the presence of sepsis as is particularly common in many low- to middle-income countries (81).
More on the topic Basic principles of newborn care:
- Introduction
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Anticipating problems
- Table of Contents
- Prepregnancy counselling