Basic principles of radiotherapy
External beam radiation
Therapeutic applications for radiation therapy followed quickly from the discovery of X-rays by Roentgen in 1895 (1). The first radiation treatment is credited to Grubbe, who reported the external beam treatment of breast cancer in 1896 (2).
Application to gynaecological cancers was almost immediate (3).However, the limited penetrating ability of the low-energy radiation of early X-ray tubes and isotopes was a major limitation. Therefore, treating targets deep within the pelvis required simultaneously delivering a high dose to the skin, often with substantial toxicity. These features limited the application of external beam radiation therapy, where the beam originates outside of the patient. Consequently, brachytherapy and near-contact external beam therapy (4) were preferred for gynaecological cancer until the advent of cobalt-60.
Isotopes versus linear accelerators
Radiative cobalt- 60 releases 1.17 and 1.33 mega- electron volt gamma rays and was the first source of a penetrating beam of megavoltage photons with a high dose rate, long half-life, and reasonable cost. This led to cobalt-60 machines becoming the most widely utilized treatment machine from the 1950s to 1970s (5). Radar research during World War II dramatically improved microwave technology. Linear accelerator-based machines (linacs) applied these advances to use microwaves to accelerate electrons onto a tungsten target and emit a fraction of their kinetic energy as mega-electron volt energy X-rays. The emitted X-rays are collimated into a beam and directed towards the patient. Advantages of linacs over cobalt-60 include higher dose rates, sharper beam edges, higher energies, and simplified radiation protection.
Typical modern linac configurations include 6-18 MV X- rays, a multileaf collimator that can dynamically shape the beam aperture with a 5 mm resolution, mechanical accuracy of about 1 mm, and integrated volumetric imaging devices.
These features allow delivery techniques, such as intensity-modulated radiation therapy (IMRT), where differential beam intensities are created, and image-guided radiation therapy (IGRT) to image the patient and adjust the targeting immediately prior to radiation delivery.Simulation
The simulation stage of radiation treatment planning acquired its name from the historical use of machines called ‘simulators' that reproduced the linac geometry. This allowed simple treatment geometries to be simulated and two-dimensional (2D) radiographs of the patient in the planned position could be acquired (7). Today's ‘computed tomography (CT) simulator' is a diagnostic CT scanner used to acquire images of the patient in the treatment position. These images are transferred to a treatment planning computer system to create a treatment plan. Tumours and relevant anatomy in gynaecological cancers may be better visualized on magnetic resonance imaging (MRI) or positron emission tomography (PET) (8, 9) and these images can be ‘fused' in the treatment planning system and used for visualization during planning.
Treatment planning: two- versus three-dimensional
Classical (also known as 2D or conventional) and modern 3D treatment planning share the concepts of using imaging to define target volumes, setting beam parameters to irradiate targets and avoid healthy tissue, and making accurate dose calculations; however, different technologies are used.
Target definition in classical treatment planning used radiographs to define a rectangular target area. Current planning involves careful ‘contouring' of images, where the radiation oncologist draws the tumour volumes and normal tissues to be avoided on the images acquired during simulation. At the end of this process, a 3D model of the patient anatomy has been constructed.
Contouring is crucially important for the quality of the treatment plan, since it will influence all future planning steps. In recognition of the importance of this step, guidelines have been created to promote accurate and consistent contours between different institutions
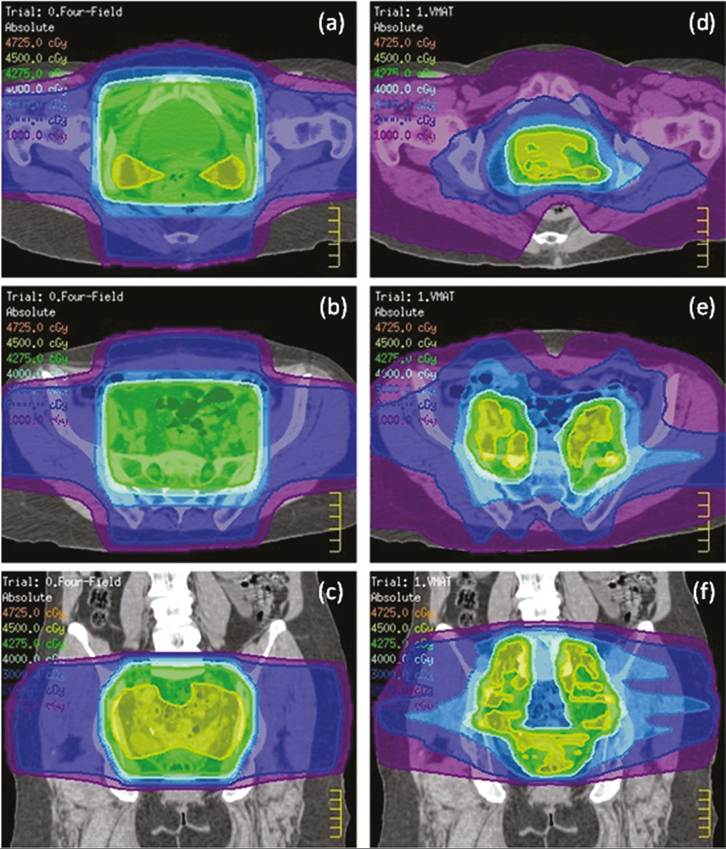
Figure 68.1 Axial CT image and dose (colourwash) illustrating a typical conventional four-field box and intensity-modulated radiation therapy treatment at the level of vagina (a, d), pelvic lymph nodes (b, e), and coronal view (c, f).
and radiation oncologists, with several dedicated solely to gynaecological cancers (10-13).
The contoured model of the patient is used to design a personalized treatment plan. The goal is always to plan a high, therapeutic target dose while minimizing normal tissue toxicity. However, modern techniques differ substantially from conventional 2D approaches.
Two classic techniques for gynaecological cancers are the ‘parallel-o pposed pair' and ‘four-field box' (Figure 68.1). The parallel-o pposed pair technique uses two beams, one entering from the anterior and one posterior. The resulting dose distribution is a relatively uniform column of dose from the anterior to posterior of the patient. The four-field box technique uses four beams, with one entering though each of the anterior, left, posterior, and right directions. The resulting dose features a uniform box-shaped high-dose region at the intersection of the beams, and is frequently used to irradiate a primary tumour and pelvic lymph nodes. These classic techniques are still used, albeit with modern planning tools. However, they have limited ability to shape the dose distribution, and a consequence of a column or box-shaped high-dose volume is that the rectum, bladder, sigmoid, and small bowel are also treated to the prescription dose.
IMRT is a revolutionary technology that uses varying intensity patterns created by dynamic multileaf collimator motion (14-17). The planner will specify objectives (e.g. a minimum dose for the target, maximum doses for normal tissue), and an optimization algorithm determines the intensity patterns that most closely achieve the objectives. The result is high-dose regions that very closely conform to even irregularly shaped target volumes while minimizing the dose to healthy tissues.
A planning study of the use of IMRT in gynaecological cancer indicated it could substantially reduce the dose to small bowel, rectum, and bladder in postoperative cervix and endometrial cancers (18).
A clinical study followed, demonstrating favourable acute (19) and chronic toxicity (20). A phase 2 Radiation Therapy Oncology Group study (RTOG 0418) demonstrated that multi-institutional studies are feasible and the single-institution experiences of toxicity reduction could be replicated (21, 22). A randomized trial (RTOG 1203, NCT01672892) of conventional treatment versus IMRT in this population has confirmed these results.IMRT has also been applied to locally advanced vulval carcinoma to avoid the high skin, gastrointestinal, and haematological toxicities associated with conventional 2D approaches. A comparison of conventional and IMRT plans demonstrated sparing of small bowel, rectum, and bladder, good disease control, and low rates of toxicity (23).
Image-guided radiotherapy
IGRT refers to real-time daily acquisition of patient images in the treatment position and adjustment prior to delivering radiation. Cone-beam computed tomography, the most common volumetric IGRT technology (24), integrates a modified CT scanner into the treatment machine. The acquired image is compared with the reference CT image acquired during the simulation, and the adjustment required to match the two images is calculated and performed remotely using a robotic treatment couch. This approach can position an easily identifiable target with an error of less than 2 mm. However, integration with the linac introduces some compromises, as cone-beam CT images have poor contrast compared with diagnostic CT images. In addition to ensuring the patient is correctly targeted, daily imaging demonstrates substantial variations in the positions of the uterus, cervix, vagina, bladder, rectum, and small bowel from day to day during a typical treatment (25-28). This has generated interest in adaptive radiation therapy. Adaptive radiation therapy uses imaging from the first few treatments to personalize and adapt treatment. In gynaecological cancers, adaptive radiation therapy may be useful when variations in uterus position and tumour regression exist.
CT and MRI have demonstrated that cervical tumour volumes shrink dramatically over 5 weeks of treatment (29), and adapting to these changes spares the bowel, rectum, and bladder (30).Another novel approach uses MRI with deformable image registration to map and accumulate the dose to mobile and deforming organs during treatment (31, 32). This accumulated dose can be used to trigger one or more replanning events to ensure targets are appropriately treated (33).
Future directions
X-ray-producing linacs are by far the most common treatment machine today; however, there is interest in other radiation types. Protons beams feature a peak dose at depth, then stop completely. Proton planning has shown this could be exploited to better spare bone marrow, bowel, and kidneys compared to IMRT (34, 35).
Carbon ion beam facilities are rare and extremely expensive; however, they produce complex DNA damage that should counteract the adverse effect of hypoxia within the cervical cancers, which is prognostic of a poor response (36, 37). A report of locally advanced cervical cancer patients treated with carbon ions was unable to demonstrate differences in disease-specific survival for oxic or hypoxic tumours, supporting this hypothesis (38).
Brachytherapy
Isotopes
Brachytherapy for gynaecological cancers has its origins very close to the isolation of radium-2 2 6 ( 226Ra) by Marie Curie. Within a decade of the isolation of 226Ra, treatment techniques for many cancers had been developed (39), including gynaecological cancers.
Radium was very useful for initial therapies using radiation; however, it suffers from several physical characteristics, which make it non-ideal as a radionuclide for brachytherapy. Its mean and maximum energies are large, which makes the dose deposition area larger than ideal, where the overarching goal of the therapy is to keep the radiation dose deposition as close as possible to the targeted lesion. In addition, the production of radon gas as the first product of its radioactive decay is problematic since this can lead to problems in containing the radioactive material, and is thus a radiation safety hazard.
Finally, the long half-life of 1622 years is also undesirable in that once the radionuclide is isolated, it must be managed and safely stored for a significant time. The advent of high-energy accelerators and nuclear reactors between the 1930s and 1950s allowed the production of non-naturally occurring radionuclides, many of which have more favourable properties than 226Ra for therapeutic purposes. With these new radionuclides, radium was gradually phased out of clinical use by the end of the 1980s.Initially, cesium-137 (137Cs) was used to replace 226Ra in gynaecological brachytherapy. This radionuclide has a mean photon energy of 660 keV and a half-life of 30.2 years. Although this is an improvement from 226Ra, this radionuclide suffers from a poor specific activity (the number of disintegrations per mass), thus the source size for i37Cs needs to be quite large in order to produce a dose rate suitable for clinical procedures. Today, most gynaecological brachytherapy is done using iridium-192 (^Ir), which has a mean photon energy of 380 keV, a very high specific activity, and a half-life of 74.2 days, making it a very good radionuclide for brachytherapy. In particular, radiation protection issues are minimized with a half-life that is short enough to simplify disposal of the radionuclide, but long enough so that it can be used over a reasonable period of time in the clinic.
Applicators
Due to the rapid fall-off of dose of the brachytherapy sources, very consistent and reproducible brachytherapy source positions are required in order to reproduce the desired therapeutic effect of brachytherapy. In addition, to better control the overall dose delivered (which depends on the dwell time of the radionuclide sources), it is desirable to use a device which is first placed without sources being loaded, in order to determine the localization of the source positions, allowing the sources to subsequently be quickly inserted and removed when treatment is finished.
In the early days of brachytherapy, inconsistent positioning of sources and other dosimetric problems led to an inconsistently delivered dose, which had a negative effect on the perception of the treatment technique. In order to address this, and to provide tools for clinicians to be able to achieve a more uniform level of implant, certain brachytherapy insertion ‘systems' were developed. These ‘systems' provided rules for source positioning and significantly improved the consistency of the clinical outcomes. In gynaecology, the
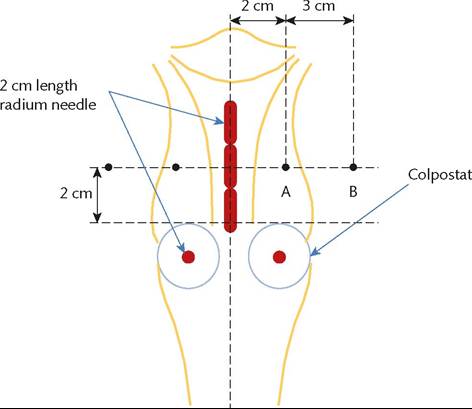
Figure 68.2 Illustration of the Manchester system. Radium needles
2 cm in length were inserted in the uterus (up to three) and in the vaginal fornixes. Dose was prescribed at point A, which is 2 cm lateral to the intrauterine needles and 2 cm superior to the surface of the colpostats, which are assumed to be flush with the vaginal mucosa. Point B, which is 3 cm lateral to point A, represents lateral dose fall off and dose to obturator lymph nodes.
‘Stockholm’ and ‘Paris' systems prescribed a manner for inserting tubes of 226Ra into the uterus and vagina, both spatially and temporally (dose rate and number of insertions), in order to provide a dose coverage that could be tailored to the clinical presentation of the disease. The space distribution of the Paris system combined with the temporal placement of sources was combined into what became known as the ‘Manchester’ system. Initially, this system used flexible tubing to place intrauterine sources and sources adjacent to the cervix. This involved inserting 2 cm long 226Ra sources (1.5 cm active length), either 1, 2, or 3 into the uterus (called the uterine tandem) and two separate 2 cm long source perpendicular to the intrauterine sources, in cylindrical applicators called colpostats inserted in the vaginal fornices. Finally, to allow consistent reporting of dose to the disease treated, specific dose calculation points were described, known as points A and B. Point A is specified as 2 cm lateral to the central intrauterine tandem and 2 cm superior to the mucous membrane of lateral vaginal fornix. This point is meant to represent the coverage dose to the cervix. Point B is taken as 3 cm lateral to point A, and represents the lateral dose drop off, and as well was considered to be representative of dose to the obturator nodes (Figure 68.2). Finally, the Manchester system also specified how to calculate the dose received at specific points in order to represent the dose to the bladder and rectum, which are the normal healthy tissues to which doses are to be minimized.
The Henschke applicators were developed in the 1960s and 1970s, and were specifically designed to give a dose distribution consistent with the Manchester system, but to be used specifically with 137Cs. The design consists of a central intrauterine tandem and two colpostats/ovoids. The separation of the colpostats could be adjusted to provide adequate lateral dose coverage. Finally, tungsten shielding was available for both the bladder and rectum as well as for the ovoids to reduce normal tissue dose if required.
The Fletcher-Suit (and later Delclos) applicators were similar to the Henschke applicator, in that it used a central tandem and two ovoid-type applicators and mimics the Manchester system. The ovoid design, however, was adjusted specifically to allow for remote afterloading, as opposed to manual loading of sources. With automated source placement, care was taken in the Fletcher-Suit- Delclos design to minimize friction in source movement, which can lead to stuck sources, and are a major risk of afterloader techniques.
Another commonly used applicator is the tandem and vaginal ring, which also allows the use of interstitial catheters inserted through the ring into parametrial tumour extension. Although requiring image-guided techniques (see ‘Image guidance’), this optimizes the dose to the residual tumour while also reducing the dose to the bladder and rectum (40).
Remote afterloading
The practice of brachytherapy necessarily involves placement of radioactive sources in patients in order to provide a therapeutic benefit. The radiation action on cancer cells also affects normal healthy tissues, including those of the clinical staff. By using suitable shielding, and by keeping the distance to the sources large (using forceps) and exposure times low, doses to the attending physician, therapists, and nurses can be kept quite low for an individual treatment. However, the cumulative exposure of the staff over multiple patient treatments can lead to a large lifetime radiation dose. For this reason, technology was developed through the 1970s in order to automate the placement of radioactive source without the need for manual placement. This work was led by the Nucletron Corporation, who developed the Selectron remote afterloader (RAL), which was marketed in the early 1980s.
The Selectron RAL was specifically designed for cervical brachytherapy, and implemented a Manchester type of source loading using i37Cs. The unit utilized a source selector, which could choose between an active source and a non-radioactive spacer. By adjusting the sequence of active source and non-active spacer, the Selectron could generate a variable pattern of radioactivity, and hence dose distribution. The unit utilized air pressure to push sources from the inner source ‘safe’ out to the Fletcher-type applicator, and suction to retrieve the sources when the treatment is completed. The unit was limited by the large 137Cs source size (2.5 mm spheres), resulting in a large applicator which was only useful for gynaecological brachytherapy, limiting its use and thus marketability as a generalized brachytherapy device. With the higher specific activity of iThr, modern brachytherapy RALs now have much smaller sources (<1 mm diameter) utilizing a single source (as opposed to a bank of sources), which is welded to a stainless steel cable. The source can then be ‘stepped’ through the target treatment volume to generate the desired dose distribution. With smaller source dimensions, generalized brachytherapy techniques are now available for a wide array of disease sites, not just gynaecological cancers.
Current RALs have other advantages as the degree of dose modulation is considerably higher than for caesium, due to the small size, but also the lower photon energy of the iridium spectra. Finally, the very high specific activity of iridium allows for considerably higher dose rates permitting treatment delivery in times in the order of minutes, as opposed to days. This also introduces new problems since the biological effect of radiation is dose-rate dependent.
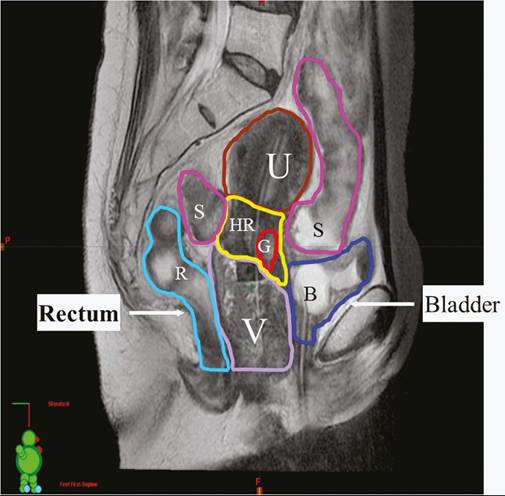
Figure 68.3 Sagittal MRI with intrauterine applicator and Foley catheter in bladder, illustrating high-risk (HR) clinical target volume, gross tumour volume (G), uterus (U), sigmoid (S), and vagina (V) with packing.
Image guidance
The correct placement of the brachytherapy applicator relative to the targeted disease area is critical to the success of the treatment. A poorly placed applicator is problematic because not only will the tumour receive less dose than required, but the normal healthy tissues will receive an unnecessary dose. Imaging is an important component of the brachytherapy applicator placement procedure, which verifies correct placement of the device. Originally, 2D planar X-ray imaging was used to define the applicator placement in relation to the target area, which could be defined using radio-opaque clips inserted into the cervix; and contrast used to define the bladder and rectal dose points.
Currently, 3D CT imaging is the method of choice for defining applicator positions. However, recent evidence (41) has shown that magnetic resonance-based imaging is the current standard for the definition of tumour volumes, including areas of suspected clinical extension. Also, the modern method of reporting doses to both the target and normal tissues is to report the integrated dose to a volume of tissue, as opposed to point doses. Thus, MRI is the imaging modality of choice, where T2-weighted imaging has been shown to be useful in defining target volumes as well as the normal tissues, namely the bladder, rectum, sigmoid, and small bowel (Figure 68.3). In addition, involved lymph nodes can be readily identified with MRI, thus allowing an accurate determination of their doses from brachytherapy.
Physics/biology
Radiation dosimetry
Modern linacs deliver a specified amount of X-ray energy with high accuracy and precision. Absorbed dose is defined as the energy absorbed per unit mass, and has the International System of Units (SI) unit of gray (Gy), which is equal to 1 J/kg. For radiation doses to be meaningful, and to facilitate comparison between different machines and different institutions, all machines must be calibrated to ensure they deliver the same absorbed dose under a specific reference condition. This is achieved by the calibration of an internal ionization monitor that measures ‘monitor units’. A common calibration is to adjust the output of the machine such that 1 cGy is delivered per monitor unit at a depth of 1.5 cm in water for a 6 MV X-ray beam with 10 ? 10 cm field size. Methods to perform this calibration are described in protocols developed by the American Association of Physicists in Medicine (42) and the International Atomic Energy Association (43). These protocols require the use of dosimeters calibrated at a national or accredited dosimetry standards laboratory, ensuring that the dose is delivered and reported consistently around the world.
The performance of linacs is maintained by routine quality assurance activities. Guidance documents from the American Association of Physicists in Medicine, for example, describe a detailed list of radiation safety features, dosimetry parameters, mechanical function, and imaging tests that are variously performed on a daily, weekly, monthly, and annual basis. A well-maintained modern machine can typically be expected to deliver the intended dose with an accuracy of 2%, and have a total mechanical accuracy of about 1 mm.
Radiation protection
While the irradiation of the patient is intentional, specific, and intended to be beneficial, any dose to others is undesirable and should be maintained as low as reasonably achievable. Limits on the permitted dose to the public and staff in a radiotherapy facility are specified nationally; however, most countries apply limits based on recommendations of the International Commission on Radiation Protection (44). Radiation protection conventionally uses the SI unit of sievert (Sv), which is the dose multiplied by a radiation effectiveness factor and an organ weighting factor. Grays, the unit of absorbed dose, and sieverts are numerically equivalent for whole-body exposure to X-rays (where the weighting factors are both equal to 1.0). In this formalism, occupational exposure is limited to 20 mSv/year (using a 5-year average) and 1 mSv/year for the public.
These limits are achieved through well-educated qualified staff and stringent facility design. The walls, door, ceiling, and floors of the room containing a linac are constructed considering the materials to be used, occupancy of adjacent spaces by staff or the public, and machine features such as maximum energy and anticipated workload. The shielding required can be substantial, and a common treatment room design that satisfies International Commission on Radiation Protection requirements uses walls constructed of 2.5 m of solid concrete.