Changes in the cardiovascular system
The increase in plasma volume in pregnancy dramatically increases the cardiovascular preload. The most important changes in the cardiovascular system are the decrease in peripheral vascular resistance (affecting afterload) and the increase in cardiac output.
These changes are a proactive process, initiated in anticipation of increased physiological demand. Indeed, some are initiated during each ovulatory menstrual cycle and then amplified by stimuli from the growing uterus and fetoplacental unit in the first 8 weeks of pregnancy (13).Haemodynamic stimuli in pregnancy
The stimuli for the dramatic cardiovascular changes in early pregnancy are due to a number of vasoactive substances. The three major oestrogens in pregnancy—oestrone, oestriol, and oestradiol—all increase until term although different patterns of change are demonstrated. Oestrone and oestradiol show a gradual increase from conception throughout early pregnancy whereas oestriol levels remain undetectable until the ninth week of pregnancy. By term, oestrone and oestriol levels are increased by about 100-fold and oestradiol by 1000-fold (13). Extensive studies of the effect of exogenous oestrogen on the cardiovascular system conclude that oestrogen increases the stroke volume and reduces vascular resistance, thus increasing cardiac output (14). The pathways of action are complex including increased synthesis of nitric oxide, stimulating production of prostaglandins (15) as well as exerting structural effects by altering production of collagen in the vasculature (16). In contrast, the serum level of progesterone remains unchanged until after the tenth week of pregnancy. At this point it gradually increases until at term it is increased threefold. Progesterone is thought to exert a vasodilatory effect. Exogenous progesterone has been reported to reduce blood pressure in non-pregnant hypertensive people (17) and increase venous distensibility (18).
The renin-angiotensin system (RAS) also exerts significant effects on maternal cardiovascular function during pregnancy. During each ovulatory menstrual cycle there is a peak in both the precursors and the hormones of this system following ovulation. If conception occurs, this peak does not return to basal levels. During pregnancy, the peripheral concentration of active renin, angiotensinogen, and angiotensin II increases until the 30th week of gestation. The RAS regulates aldosterone release therefore aldosterone concentration is
also raised in pregnancy. This counters the natriuretic effect of progesterone at the distal tubule and results in sodium retention and plasma volume expansion. Angiotensin II is primarily a vasoconstrictor. Despite its elevated levels in pregnancy, the blood pressure remains reduced in pregnancy due to reduced sensitivity to its vasopressor effects (19, 20). The only component of this system reported to be reduced in pregnancy is angiotensin-converting enzyme (21).
Cardiac output, stroke volume, and heart rate
In nulliparous women, the cardiac output is increased by approximately 35-40%, and by around 50% in multiparous women. This can rise by a further 33% during labour. The cardiac output remains high for 24 hours after delivery and then gradually declines over 2 weeks to prepregnancy levels (22, 23). The majority of the increase in cardiac output occurs in the first trimester. By 8 weeks' gestation, the cardiac output has increased by 13% compared to at 5 weeks' gestation; this is further increased in the second and third trimesters due to increases in stroke volume and heart rate. Nearly 90% of the increase in cardiac output in the first 5 weeks of pregnancy can be attributed to the increase in heart rate. The heart rate then continues to rise more slowly until 32 weeks' gestation. The average increase is 10-15 beats per minute although there is wide individual variation. The increase in stroke volume occurs slightly later, starting gradually by the fifth week of pregnancy and plateauing in the second trimester (23, 24).
Total peripheral resistance decreases significantly by just 6 weeks' gestation. This decrease continues until approximately 20 weeks' gestation when a 40% reduction in peripheral vascular resistance is observed. This decreased total peripheral resistance is due to the changes in hormonal vasodilator and vasoconstrictor functions, rather than sympathetic tone, in addition to circulating prostaglandins and locally synthesized nitric oxide. The reduction in afterload causes an initial decrease in both the systolic and diastolic blood pressures in the first half of pregnancy with the diastolic blood pressure decrease exceeding the systolic. The most dramatic reduction in blood pressure (by 80-90%) occurs before 8 weeks of pregnancy where the mean arterial pressure is approximately 10 mmHg lower than during prepregnancy (23). Following this, the mean arterial pressure continues to decrease steadily, reaching a nadir at approximately 24 weeks (23). The reduction in blood pressure, in addition to increased levels of oestrogen and progesterone, trigger the renin- angiotensin-aldosterone system causing retention of sodium, an increase in total body water, and an increase in the plasma volume by about 50%. Thus in the latter half of pregnancy, the blood pressure then steadily increases in parallel with the increasing plasma volume and peripheral sympathetic activity. These changes are demonstrated in Figure 8.2 and Table 8.1.
Systemic vascular resistance is calculated by the ratio of mean arterial pressure and cardiac output. As with blood pressure it decreases in the first weeks of pregnancy, reaching a nadir in mid pregnancy and gradually increasing towards term. Blood flow increases in the low impedance uteroplacental circulation. Renal blood flow also gradually increases during pregnancy until the third trimester when it is 60-80% higher than prepregnancy levels. These are a result of renal vasodilatation resulting in lower glomerular filtration rates (GFRs).
The pulmonary resistance decreases in early pregnancy and remains fairly static throughout pregnancy. This is due to the capacity of the pulmonary circulation to absorb high rates of flow without an increase in pressure.The physiological changes in preload and afterload are accompanied by remodelling of the atria and ventricles. The left ventricular end-diastolic diameter is increased between the 10th and 20th weeks of pregnancy and then plateaus at approximately 5% greater than the prepregnancy value (27, 28). This higher left ventricular end- diastolic
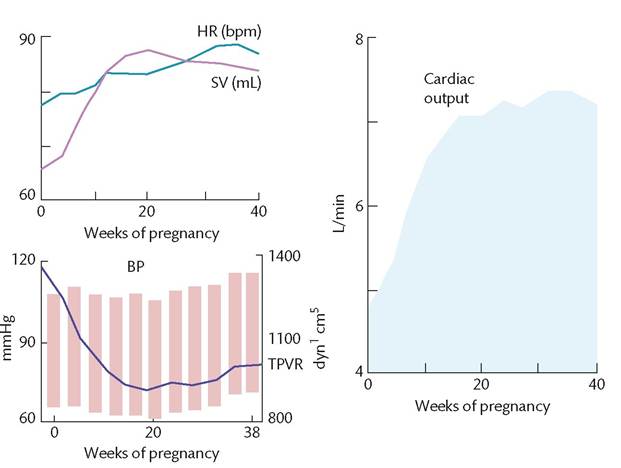
Figure 8.2 Major haemodynamic changes associated with normal human pregnancy. The marked augmentation of cardiac output results from asynchronous increases in both heart rate (HR) and stroke volume (SV). Despite the increase in cardiac output, blood pressure (BP) decreases for most of pregnancy. This implies a very substantial reduction in total peripheral vascular resistance (TPVR).
Table 8.1 Percentage changes in key cardiovascular variables in pregnancy
| First trimester (%) | Second trimester (%) | Third trimester (%) | |
| Heart rate (beats per minute) | +11 | +13 | +16 |
| Stroke volume (mL) | +31 | +29 | +27 |
| Cardiac output (L/min) | +45 | +47 | +48 |
| Systolic blood pressure (mmHg) | -1 | +1 | +6 |
| Diastolic blood pressure (mmHg) | -6 | -3 | +7 |
| Mean pulmonary artery pressure (mmHg) | +6 | +5 | +5 |
| Total peripheral resistance (resistance units) | -27 | -27 | -29 |
Mean pulmonary artery pressure data are derived from studies in which preconception values were determined.
The mean values shown are those at the end of each trimester and are thus not necessarily the maxima.Source data from Robson SC, Hunter S, Boys RJ, Dunlop W. Serial study of factors influencing changes in cardiac output during human pregnancy. American Journal of Physiology - Heart and Circulatory Physiology. 1 989;256(4):H1060-65.
diameter is associated with a rise in preload. In addition, the left ventricular end-systolic diameter is reduced in the first trimester compared to prepregnancy in accordance with the increased heart rate and contractility. There are also changes in the right ventricle, right atrium, and left atrium as described in Table 8.2.
Clinical considerations
• In pregnancy, the heart is pushed upwards by the elevation of the diaphragm and rotated forwards. The volume of the heart is increased by about 12% in pregnancy (28). Small pericardial effusions are frequently found which resolve after delivery.
• The apex beat is moved upwards and laterally under the fourth rib. The first heart sound becomes louder and there is an exaggerated splitting of this sound as the mitral valve closes earlier.
• Most women remain in sinus rhythm throughout pregnancy although premature atrial and ventricular complexes are more frequent. Increases in the atrial size may contribute to atrial arrhythmias during pregnancy. Those with pre- existing arrhythmias are at higher risk of adverse cardiac events during pregnancy.
• The most common changes observed on electrocardiography are increased heart rate, increased QT interval, and deviation to the left electrical axis due to the changed position of the heart. In many women the T wave becomes flattened or inverted in lead III (30, 31) and one-third of women show ST segment changes after exercise at the end of pregnancy (32, 33).
• In pregnancy, a special effort must be made to obtain accurate blood pressure measurements. Blood pressure is lowest when the woman is lying supine on her left side and is significantly different to when recorded sitting.
Sequential measurements should be made in the same positon for comparable results.• In addition, the difference between Korotkoff sounds IV (muffling of sound) and V (disappearance of sound) is increased in pregnancy. It is the current consensus that Korotkoff sound V is the most reliable in pregnancy.
• Many automatic devices are inaccurate in pre-eclampsia. Care should also be taken to ensure that blood pressure devices are validated in accordance with an established protocol.
• The vena cava is compressed by the uterus. This can result in a profound drop in blood pressure when the mother lies on her back. This is known as supine hypotension syndrome. Venous return from the lower limbs is restricted causing a drop in the stroke volume.
• The increased demand of pregnancy on the cardiovascular system may be detrimental to those with limited cardiac reserve. Despite the increased blood volume and the atrial and ventricular distension, cardiac filling pressures are not increased in women at term compared to postpartum because in pregnancy the normal heart compensates for these changes. Women with valve disease such as mitral stenosis or with dilated cardiomyopathy may not be able to compensate for the increased preload and are at risk of developing heart failure. In contrast, the increased preload and ventricular dimensions may improve the cardiovascular haemodynamics for women with hypertrophic cardiomyopathy. The increased cardiac work of pregnancy requires increased myocardial oxygen consumption. Therefore, women with coronary disease are at increased risk of ischaemia.
• Blood flow to the peripheries increases, resulting in warm hands and feet. Nasal congestion occurs due to increased blood flow to the nasal mucosa.