Changes in the haematological and immune system
Blood volume includes both plasma volume and red cell mass. These are under different physiological control. Plasma volume increases by approximately 50% in pregnancy from 2600 mL prepregnancy to 3850 mL by 32-34 weeks' gestation where it plateaus (1, 2).
In multiparous women this increase can be higher (up to 60%). Plasma volume is directly correlated to the growth of the baby (2) with multiple pregnancies associated with significantly increased plasma volumes (1). Impaired fetal growth is associated with a poor increase in plasma volume (3).There is also a steady increase in the red cell mass in pregnancy. The circulating volume of red cells prior to pregnancy is approximately 1300 mL which increases by 20-30% in pregnancy (4). This change in mass is due to an increase in both red cell number and size. Women taking iron supplements and women with multiple pregnancies have a greater increase (5). Erythropoietin is increased in pregnancy by 50%, but less so with iron supplementation (25%) (6). This is thought to be stimulated by human placental lactogen (7).
Serum iron concentrations decrease in pregnancy despite the increase in absorption of iron from the gut. The increase in transferrin increases the iron-binding capacity. The increased renal clearance of folate towards the term pregnancy causes plasma folate concentrations to be halved.
The total white cell count increases during pregnancy due to an increase in neutrophil polymorphonuclear leucocytes which peaks at 30 weeks' gestation before plateauing. This increase in neutrophils is initiated at the time of the oestrogen peak in a normal menstrual cycle and then continues if conception occurs (8). A further fourfold increase in the number of polymorphs occurs during labour and immediately following delivery. Their phagocytic function increases during pregnancy. Eosinophil, basophil, and monocyte levels remain relatively constant during pregnancy until a significant reduction in eosinophils occurs at the time of labour and delivery.
The lymphocyte count does not alter significantly during pregnancy and there is no change in the number of circulating T and B cells (9). However, their function is depressed in pregnancy, potentially due to the increased concentration of glycoprotein coating as stimulated by the high levels of oestrogen in pregnancy which reduce the response to stimuli (10). Human chorionic gonadotropin and prolactin are also known to supress lymphocyte function, but there is no reduction in humoral immunity or immunoglobulins.In pregnancy, two types of fetal tissue are in direct contact with maternal tissues. Villous trophoblasts form a continuous syncytium that is b athed in maternal blo od and extravillous trophoblasts contact maternal endometrial/decidual tissues. Both appear to be immunologically inert. Villous trophoblasts do not express human leucocyte antigen (HLA) class I or II molecules. Extravillous trophoblasts do not express HLA-A or HLA-B but do express trophoblast-specific HLA- G, HLA-C, and HLA- E. The main type of decidual lymphocyte is the decidual natural killer cells. These differ from systemic natural killer cells as they express surface killer immunoglobulin-like receptors (KIRs) which bind to HLA-G and HLA-C on the trophoblast. KIRs are highly polymorphic and HLA-C is also polymorphic, therefore there is a potentially very variable receptor-ligand system. The impact of this is that one receptor ligand combination, KIR AA and HLA-C2, is associated with an increased possibility of miscarriage or pre-eclampsia (11).
Platelets can decrease in number throughout a normal pregnancy and the platelet volume increases from 28 weeks' gestation due to an increase in large and immature platelets. This suggests that there is destruction of platelets in pregnancy. The reactivity of platelets is increased in the second and third trimester and returns to normal 12 weeks after delivery.
There are dramatic changes to the coagulation system in pregnancy with a mild coagulopathy throughout normal pregnancy.
The end result of coagulation is formation of a fibrin clot from fibrinogen involving a complex interaction of clotting factors. There are changes in many clotting factors as summarized in Figure 8.1, which contribute to this coagulopathy. Factors VII, VIII, VIII:C, X,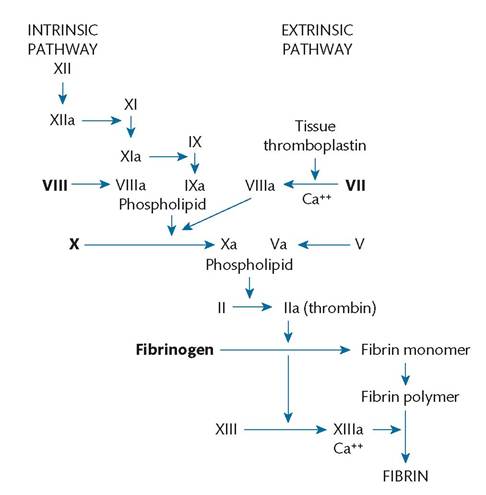
Figure 8.1 Alterations in the coagulation pathways associated with human pregnancy. Factors which increase during normal pregnancy are shown in colour.
Source data from Chamberlain G, Broughton Pipkin F (eds); Clinical Physiology in Obstetrics, 3rd edn. Oxford: Blackwell Science, 1998:71-1 10.
and IX are all increased in pregnancy and factors II and V remain constant. Factor XI and XIII both decrease in pregnancy by 60-70% and 50% respectively. Protein S, a cofactor of protein C which inactivates factors V and VIII, is reduced in the first two trimesters of pregnancy.
Plasma fibrinogen levels approximately double in pregnancy from 2.5-4 g/L to 6.0 g/L in late pregnancy. Concentrations of high-molecular-weight fibrin/fibrinogen complexes also increase in normal pregnancy. This increase in fibrinogen contributes to a rise in the erythrocyte sedimentation rate. An estimated 5-10% of all circulating fibrinogen is consumed at the time of placental separation. In contrast, plasma fibrinolytic activity is decreased in pregnancy and labour but quickly returns to non-pregnant values after delivery suggesting that mediators are derived from the placenta (12).
Clinical considerations
• The increase in plasma volume is greater than the increase in red cell mass, therefore the concentration of haematocrit, haemoglobin, and red cell count will reduce in pregnancy. This is termed physiological anaemia.
• Dramatic changes in the blood volume occur at delivery. Average blood loss can be tolerated without a significant decrease in haemoglobin concentrations. In the non-pregnant state, acute blood loss is associated with a subsequent increase in plasma volume causing a decrease in haematocrit over the following days.
In pregnancy, there is gradual decrease in plasma volume due to diuresis following delivery and therefore haematocrit gradually increases.• The activation of the clotting system during labour increases the risk of disseminated intravascular coagulation, which may be triggered by other stimulus, such as amniotic fluid embolus. In this • Adolescents are at particular risk of iron deficiency in pregnancy. Even mild anaemia is associated with decreased birthweight therefore appropriate supplementation is key.
• Neutrophilia during labour and immediate puerperium should not be assumed to be due to infection as this is a normal physiological response.
• The increased coagulability increases the risk of thrombotic disease therefore all women should be assessed for their risk of venous thromboembolism and appropriate precautions taken if their risk is increased.