Chapter 41 Menopause
This chapter deals primarily with APGO Educational Topic Area:
TOPIC 42 MENOPAUSE
Students should be able to define and describe the physiologic changes associated with menopause.
They should outline a basic approach to evaluation and management of the perimenopausal or menopausal patient. They should identify risk factors, common presenting signs and symptoms, and physical exam findings. They should be able to counsel women about the menopausal transition including long-term changes.Clinical Case
A 54-year-old woman comes to see you because she has been having trouble sleeping. She reports that her youngest child recently left for college, and she has just felt “off ” recently. She has been irritable with her husband and feels somewhat tired. Her husband complains that her thrashing about at night keeps him awake. Also her menstrual cycle has been irregular with her last bleeding occurring 4 months ago.
Menopause is the permanent cessation of menses after significant decrease of ovarian estrogen production. This is evidenced by 12 consecutive months with no menstrual bleeding. Perimenopause is the period before menopause, that is, the transition from the reproductive to the nonreproductive years during which ovarian estrogen production may fluctuate unpredictably. The time period during which the changes of menopause occur is called the climacteric. An increasing proportion of American women are included in these groups, because the female life expectancy has lengthened, and the number of women in this age group is expanding (Fig. 41.1).
 MENSTRUATION AND MENOPAUSE
MENSTRUATION AND MENOPAUSE
Although male gametes are renewed on a daily basis, female gametes are of a fixed number that progressively diminish throughout a woman’s reproductive life. At the time of birth, the female infant has approximately 1 to 2 million oocytes; by puberty, she has approximately 400,000 oocytes remaining.
By ages 30 to 35 years, the number of oocytes would have decreased to approximately 100,000. For the remaining reproductive years, the process of oocyte maturation and ovulation becomes increasingly inefficient, with the continued loss of functional oocytes.A woman ovulates approximately 400 oocytes during her reproductive years. The process of oocyte selection is complex, and new information is making the process clearer. During the reproductive cycle, a cohort of oocytes is stimulated to begin maturation, but only one or two dominant follicles complete the process and are eventually ovulated.
Follicular maturation is induced and stimulated by the pituitary release of the follicle-stimulating hormone (FSH) and luteinizing hormone (LH). FSH binds to its receptors in the follicular membrane of the oocyte and stimulates follicular maturation, providing estradiol (E2), which is the major estrogen of the reproductive years. LH stimulates the theca luteal cells surrounding the oocyte to produce androgens as well as estrogens and serves as the triggering mechanism to induce ovulation. With advancing reproductive age, the remaining oocytes become increasingly resistant to FSH. Thus, plasma concentrations of FSH begin to increase several years in advance of actual menopause, when the FSH is generally found to be >30 mIU/mL (Table 41.1).
Menopause marks the end of a woman’s natural reproductive life. The average age for menopause in the United States is between ages 50 and 52 years (median 51.5), with 95% of women experiencing this event between ages 44 and 55 years. The age of menopause is not influenced by the age of menarche, number of ovulations or pregnancies, lactation, or the use of oral contraceptives. Race, socioeconomic status, education, and height also have no effect on the age of menopause. Genetics and lifestyle, however, can affect the age of menopause. Undernourished women and smokers, for example, tend to have an earlier menopause, although the effect is slight.
Approximately 1% of women undergo menopause before the age of 40 years, which is generally referred to as premature ovarian failure (POF). Women spend roughly one third of their lifespan in menopause.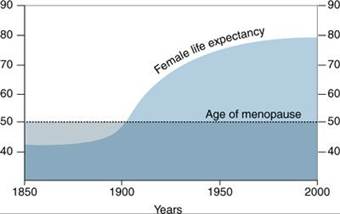
FIGURE 41.1. Age of menopause and female life expectancy.
Contrary to popular belief, the ovaries of postmenopausal women are not quiescent. Under the stimulation of LH, theca cell islands in the ovarian stroma produce hormones, primarily the androgens testosterone and androstenedione. Testosterone appears to be the major product of the postmenopausal ovary. Testosterone concentrations decline after menopause, but remain two times higher in menopausal women with intact ovaries than in those whose ovaries have been removed. Estrone (E1) is the predominant endogenous estrogen in postmenopausal women. It is termed extragonadal estrogen because the concentration is directly related to body weight. Androstenedione is converted to E1, proportionate to the amount of fatty tissue (Table 41.2). Because estrogen promotes endometrial proliferation, obese menopausal women have a higher risk of endometrial hyperplasia and carcinoma. Conversely, slender menopausal women are at a higher risk for menopausal symptoms.
 SYMPTOMS AND SIGNS OF MENOPAUSE
SYMPTOMS AND SIGNS OF MENOPAUSE
Menopause is a physiologic process that can be associated with symptoms that may affect a woman’s quality of life. Decreased estrogen production can result in multiple adverse systemic effects (Fig. 41.2). Many of these symptoms can be ameliorated with hormone therapy (HT). The need for HT should be individualized based on a woman’s specific risk factors.

Menstrual Cycle Alterations
Beginning at approximately the age of 40 years, the number of a woman’s ovarian follicles diminishes, and subtle changes occur in the frequency and length of menstrual cycles.
A woman may note shortening or lengthening of her cycles. The luteal phase of the cycle remains constant at 13 to 14 days, whereas the variation of cycle length is related to a change in the follicular phase. As a woman approaches menopause, the frequency of ovulation decreases from 13 to 14 times per year to 11 to 12 times per year. With advancing reproductive age, ovulation frequency may decrease to three to four times per year.With the change in reproductive cycle length and frequency, there are concomitant changes in the plasma concentration of FSH and LH. More FSH is required to stimulate follicular maturation. Beginning in the late thirties and early forties, the concentration of FSH begins to increase from normal cyclic ranges (6–10 IU/L) to perimenopausal levels (14–24 IU/L). During this period, women begin to experience sometimes unpleasant symptoms and signs of decreasing estrogen levels. Some women are not symptomatic yet have significant clinical effects such as early osteoporosis. Levels of FSH are 30 IU/L or more at menopause.
Hot Flushes and Vasomotor Instability
Coincident with the change in reproductive cycle length and frequency, the hot flush is usually the first physical manifestation of decreasing ovarian function and is a symptom of vasomotor instability.


FIGURE 41.2. Effects of menopause.
Hot flushes are recurrent, transient episodes of flushing, perspiration, and a sensation ranging from warmth to intense heat on the upper body and face, sometimes followed by chills. When they occur during sleep and are associated with perspiration, they are termed night sweats. Occasional hot flushes begin several years before actual menopause. Other conditions that can cause hot flushes include thyroid disease, epilepsy, infection, and use of certain drugs.
The hot flush is the most common symptom of decreased estrogen production and is considered one of the hallmark signs of perimenopause. However, its incidence varies widely. Some U.S. studies have found that about 75% of women experienced hot flushes during the transition from the perimenopause to postmenopause. Outside the United States, rates vary even more widely, from about 10% in Hong Kong to 62% in Australia. Reasons for these differences are unknown. In the United States, prevalence rates also differ among perimenopausal women of racial and ethnic groups, with African Americans most frequently reporting symptoms (45.6%), followed by Hispanics (35.4%), whites (31.2%), Chinese (20.5%), and Japanese (17.6%). More recent studies seem to indicate that differences in body mass index (BMI) would be a more reliable indicator of the incidence of hot flushes.
Hot flushes have a rapid onset and resolution. When a hot flush occurs, a woman experiences a sudden sensation of warmth. The skin of the face and the anterior chest wall become flushed for approximately 90 seconds. With resolution of the hot flush, a woman feels cold and breaks out into a “cold sweat.” The entire phenomenon lasts less than 3 minutes. The exact cause of hot flushes has not been determined, although it seems that declining estradiol-17β secretion by the ovarian follicles plays a significant role. As a woman approaches menopause, the frequency and intensity of hot flushes increase. Hot flushes may be disabling during the day and even more so at night when they are a significant cause of clinical sleep disturbance. When perimenopausal and postmenopausal women receive HT, hot flushes usually resolve in 3 to 6 weeks, though sometimes even more rapidly, depending on the dose administered. If a menopausal woman does not receive HT, hot flushes usually resolve spontaneously within 2 to 3 years, although some women experience them for 10 years or longer. Hot flushes are not simply an uncomfortable part of the normal perimenopause and menopause insofar as they are associated with significant adverse outcomes, such as hampered job productivity and sleep deprivation.
Sleep Disturbances
Declining E2 levels induce a change in a woman’s sleep cycle so that restful sleep becomes difficult and, for some, impossible. The latent phase of sleep (i.e., the time required to fall asleep) is lengthened with alterations in REM (rapid eye movement) patterns; the actual period of sleep is shortened. Therefore, perimenopausal and postmenopausal women complain of having difficulty falling asleep and of waking up soon after going to sleep. Sleep disturbances are one of the most common and disabling effects of menopause.
Women with marked sleep aberration are understandably often tense and irritable and have difficulty with concentration and interpersonal relationships. With HT, the sleep cycle is restored to the premenopausal state.
Vaginal Dryness and Genital Tract Atrophy
The vaginal epithelium, cervix, endocervix, endometrium, myometrium, and uroepithelium are estrogen-dependent tissues. With decreasing estrogen production, these tissues become atrophic, resulting in various symptoms. The vaginal epithelium becomes thin and cervical secretions diminish. Women experience vaginal dryness while attempting or having sexual intercourse, leading to diminished sexual enjoyment and dyspareunia. Atrophic vaginitis also may present with itching and burning. The thinned epithelium is also more susceptible to becoming irritated by common skin irritants or infected by local flora. This discomfort can be relieved with systemic HT or the topical use of estrogen.
The endometrium also becomes atrophic, sometimes resulting in postmenopausal spotting. The paravaginal tissues that support the bladder and rectum become atrophic. When this is combined with the effects of childbearing, it can result in loss of support for the bladder (cystocele or anterior vaginal prolapse) and rectum (rectocele or posterior vaginal prolapse). In addition, uterine prolapse is more common in the hypoestrogenic patient. Because of atrophy of the lining of the urinary tract, there may be symptoms of dysuria and urinary frequency, a condition called atrophic urethritis. HT can relieve the symptoms of urgency, frequency, and dysuria. Loss of support to the urethrovesical junction may result in stress urinary incontinence; in some cases, pelvic muscle (Kegel) exercises may relieve some of these symptoms.
Mood Changes and Memory Changes
Perimenopausal and postmenopausal women often complain of volatility of affect. Some women experience memory loss, depression, apathy, and “crying spells.” These may be related to menopause, to sleep disturbances, or both. The physician should provide counseling and emotional support as well as medical therapy, if indicated. Because there may be a comorbid sleep disorder, such as obstructive sleep apnea and restless legs syndrome (RLS), consultation with a sleep medicine expert for consideration of an overnight sleep study may be appropriate in some cases. Although sex steroid hormone receptors are present in the central nervous system (CNS), there is insufficient evidence about the role of estrogens in CNS function to implicate a direct affective mechanism.
Skin, Hair, and Nail Changes
Some women notice changes in their hair and nails with the hormonal changes of menopause. Estrogen influences skin thickness. With declining estrogen production, the skin tends to become thin, less elastic, and eventually more susceptible to abrasion and trauma. Estrogen stimulates the production of the sex hormone–binding globulin (SHBG), which binds androgens and estrogens. With declining estrogen production, less SHBG is available, thereby increasing the level of free testosterone. Increased testosterone levels may result in increased facial hair. Moreover, changes in estrogen production affect the rate of hair shedding. Hair from the scalp is normally lost and replaced in an asynchronous way. With changes in estrogen production, hair is shed and replaced in a synchronous way, resulting in the appearance of increased scalp hair loss at a given point in time. Disturbing as physiologic scalp hair loss may be, physicians should reassure patients that the process is self-limiting and requires no therapy. Nails become thin and brittle with estrogen deprivation but are restored to normal with estrogen therapy.
Osteoporosis
Bone demineralization is a natural consequence of aging. Diminishing bone density occurs in both men and women. However, the onset of bone demineralization occurs 15 to 20 years earlier in women than in men because of acceleration after ovarian function ceases. Bone demineralization not only occurs with natural menopause but also has been reported in association with decreased estrogen production in certain groups of young women (such as those with eating disorders or elite athletes with an exercise-associated lower BMI). Risk factors warranting earlier screening for osteoporosis are shown in Box 41.1.
Estrogen receptors (ERs) are present in osteoblasts, which suggests a permissive and perhaps even an essential role for estrogen in bone formation. Estrogen affects the development of cortical and trabecular bone, although the effect on the latter is more pronounced. Bone density diminishes at the rate of approximately 1% to 2% per year in postmenopausal women, compared with approximately 0.5% per year in perimenopausal women (Fig. 41.3). HT, especially when combined with appropriate calcium supplementation and weight-bearing exercise, can help slow bone loss in menopausal women. Weight-bearing activity such as walking for as little as 30 minutes a day increases the mineral content of older women.
Calcium is beneficial to prevent bone loss; women older than age 50 years should meet the Recommended Dietary Allowance of 1,200 mg. Calcium therapy combined with estrogen therapy is more effective than calcium alone. In addition, for those with limited sun exposure and those lacking other dietary sources, supplementation with vitamin D should be considered: 600 IU/day from ages 51 to 70 years and 800 IU/ day for ages greater than 70 years.
BOX 41.1 When to Screen for Bone Density Before Age 65 Years
Bone density should be screened in postmenopausal women younger than age 65 years if any of the following risk factors are noted:
• Medical history of a fragility fracture
• Body weight less than 127 lb
• Medical causes of bone loss (medications or diseases)
• Parental medical history of hip fracture
• Current smoker
• Alcoholism
• Rheumatoid arthritis
American College of Obstetricians and Gynecologists. Osteoporosis. Practice Bulletin 129. Washington, DC: American College of Obstetricians and Gynecologists; September, 2012.
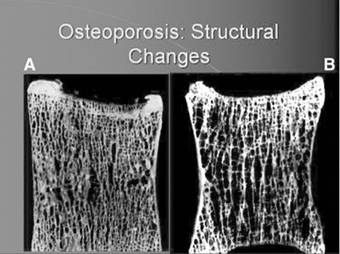
FIGURE 41.3. Structural bone changes with osteoporosis. (A) Normal bone. (B) Osteoporotic trabecular bone. (From Randolph JF, Lobo RA. Menopause. In: Precis: Reproductive Endocrinology. 3rd ed. Washington, DC: ACOG; 2007:185.)
Progressive, linear decrease in bone mineral mass is noted in women who do not receive HT in the first 5 to 10 years following menopause. When HT is initiated before or at the time of menopause, bone density loss is greatly reduced, although this benefit is lost 1–2 years after discontinuation. HT begun in a woman 5 or more years after menopause may still have a positive effect on bone density loss. However, osteoporosis is not the primary indication for HT. Several bisphosphonates, such as alendronate, ibandronate, and risedronate, can be used for the management of menopause-associated bone loss. These agents reduce bone resorption through the inhibition of osteoclastic activity (Table 41.3).
Selective estrogen receptor modulators (SERMs) provide another nonhormonal management option. Most estrogenic responses are mediated in the body by one of two receptors, either ERα or ERβ. SERMs are ER ligands, which act like estrogens in some tissues but block estrogen action in others. Examples include tamoxifen and raloxifene, which exhibit ER antagonist activity in the breast but agonist activity in the bone. As with the bisphosphonates, they also lack the capabilities of mitigating many of the other estrogen deprivation symptoms, such as hot flushes and sleeplessness, and may even exacerbate these symptoms.
Cardiovascular Lipid Changes
With perimenopause, changes occur in the cardiovascular lipid profile. Total cholesterol increases, high-density lipoprotein cholesterol decreases, and low-density lipoprotein cholesterol increases. HT may promote changes in the lipid profile that are favorable to the cardiovascular system. Retrospective case– control studies suggest that estrogens have a cardioprotective effect. However, data from the Women’s Health Initiative (WHI) suggest that no such protection exists in placebo-controlled clinical trials, although some have criticized these trials because of various methodological flaws, including the late age onset of treatment in a large group of the study subjects. Current trials are underway using transdermal estrogen and natural progesterone administered to women in their fifties to better understand whether earlier HT carries the same risk as shown in the WHI. At this time, HT should not be offered to patients with the primary goal of protection against heart disease.
PREMATURE OVARIAN FAILURE
The diagnosis of POF applies to the approximately 1% of women who experience menopause before the age of 40 years. The diagnosis should be suspected in a young woman with hot flushes and other symptoms of hypoestrogenism and secondary amenorrhea (e.g., a woman seeking treatment for infertility). The diagnosis is confirmed by laboratory findings of menopausal FSH levels (>30 mIU/mL). Interestingly, hot flushes are not as common as might be expected in this group of patients. The diagnosis has profound reproductive and emotional implications for most patients, especially if their desires for childbearing have not been fulfilled, as well as metabolic and constitutional implications. There are many causes of premature loss of oocytes and premature menopause; some of the more common causes are discussed below. Given its potential dramatic impact, POF demands a careful workup in order to identify the underlying cause and permit appropriate management.

Genetic Factors
Several factors influence a woman’s reproductive lifespan. Genetic information that determines the length of a woman’s reproductive life is carried on the distal long arm of the X chromosome. Partial deletion of the long arm of one X chromosome results in POF. Total loss of the long arm of the X chromosome, as seen in Turner syndrome, results in ovarian failure at birth or in early childhood. When suspected, these diagnoses can be established by careful mapping of the X chromosome. Additionally, screening for premutations for the fragile X syndrome should be performed because of its association with POF. These patients are at risk for having children with mental disabilities. Evaluation for any Y chromosome material should also be performed, because, if identified, oophorectomy should be performed because of the risk of cancer in these patients.
Autoimmune Disorders
Some women develop autoantibodies against thyroid, adrenal, and ovarian endocrine tissues. These autoantibodies may cause ovarian failure. These women may need HT for the indications described above; some will spontaneously resume ovarian function.
Smoking
Women who smoke tobacco can undergo ovarian failure some 3 to 5 years earlier than the expected time of menopause. It is established that women who smoke metabolize E2 primarily to 2-hydroxyestradiol. The 2-hydroxylated estrogens are termed catecholestrogens because of their structural similarity to catecholamines. The catecholestrogens act as antiestrogens and block estrogen action. The effects of smoking should be considered in smokers who are experiencing symptoms of estrogen deficiency and be part of routine menopausal counseling.
Alkylating Cancer Chemotherapy
Alkylating cancer chemotherapeutic agents affect the membrane of ovarian follicles and hasten follicular atresia. One of the consequences of cancer chemotherapy in reproductive age women is loss of ovarian function. Young women being treated for malignant neoplasms should be counseled of this possibility and advised that they may be candidates for follicular retrieval and cryopreservation as a means for attempting future pregnancy.
Hysterectomy
Surgical removal of the uterus (hysterectomy) in reproductive age women is associated with hormonal aspects of menopause some 3 to 5 years earlier than the expected age. The mechanism for this occurrence is unknown. It is likely to be associated with alteration of collateral ovarian blood flow resulting from the surgery.
MANAGEMENT OF MENOPAUSE
The changes of menopause result from declining 17-β estradiol production by the ovarian follicles. 17-β estradiol and its metabolic byproducts, E1 and estriol, are used in HT, the objective of which is to diminish the signs and symptoms of menopause.
Estrogen Therapy
Several different estrogen preparations are available through various routes of administration, including oral medications, transdermal preparations, and topical preparations. When administered orally, 17-β estradiol is oxidized in the enterohepatic circulation to E1. 17-β estradiol remains unaltered when it is administered transdermally, transbuccally, transvaginally, intravenously, or intramuscularly (IM). Unfortunately, IM E2 administration results in unpredictable fluctuations in plasma concentration. When E2 is administered across the vaginal epithelium, absorption is poorly controlled, but remains at very low levels when appropriately used. Pharmacologic plasma concentrations of E2 can result when excessive amounts are used. Transdermal administration of E2 results in steady, sustained estrogen blood levels and may be a preferable alternative to oral dosing for many patients.
Combined Estrogen and Progestin Therapy
The administration of continuous unopposed estrogens can result in endometrial hyperplasia and an increased risk of endometrial adenocarcinoma. Therefore, it is essential to administer a progestin in conjunction with estrogens in women who have not undergone hysterectomy. Progestins may include any variety of synthetics, such as medroxyprogesterone acetate and norethindrone or micronized progesterone. To achieve this protective effect, the progestin chosen may be given continuously in low doses or sequentially in higher doses. Sequential dosing is usually for 10 or 12 days of each calendar month. Progestins, particularly medroxyprogesterone acetate, may be associated with unacceptable side effects, such as affective symptoms and weight gain. If estrogen is administered alone because of unacceptable side effects of progestins, then it is imperative to counsel the patient about the need for yearly endometrial biopsy.
There are two principal regimens for HT. Continuous estrogen replacement with cyclic progestin administration results in excellent resolution of symptoms and cyclic withdrawal bleeding from the endometrium. One of the difficulties of this method of therapy is that many postmenopausal women do not want a return of menstrual bleeding. As a result, many physicians and patients choose to avoid the problem of cyclic withdrawal bleeding by the daily administration of both an estrogen and a low-dose progestin.
There are a variety of estrogen preparations available. Most perimenopausal and menopausal women respond to one of these preparations, all of which ameliorate acute menopause symptoms and relieve vaginal atrophy. The administration of progestins for 10 to 12 days of each month converts the proliferative endometrium into a secretory endometrium, brings about endometrial sloughing, and prevents endometrial hyperplasia or cellular atypia. Continuous oral progestin therapy or a levonorgestrel intrauterine device may be used to produce endometrial atrophy.
Numerous preparations combining estrogen and progestins are available in both oral and transdermal formulation. The most widely used contain a combination of conjugated equine estrogens and medroxyprogesterone acetate in one tablet. Newer preparations include a combination of micronized estradiol and norethynodrel acetate or ethinyl estradiol and norethindrone acetate. Transdermal preparations include a combination of micronized estradiol and norethindrone acetate. Low-dose oral contraceptives may also be used to relieve the vasomotor symptoms of menopause.
CAUTIONS IN HORMONE THERAPY
The results of the WHI in 2002 revealed epidemiologic findings that have modified the contemporary use of HT. This large, multicenter, randomized clinical trial (approximately 17,000 women) studied the effects of HT, dietary modification, and calcium and vitamin D supplementation as related to heart disease, fractures, breast cancer, and colorectal cancer. Although there are features of this study that are not applicable to many younger menopausal patients, the overall results suggested that when compared with placebo, a combination of conjugated equine estrogens and continuous low-dose medroxyprogesterone acetate resulted in an increased risk of heart attack, stroke, thromboembolic disease, and breast cancer, with a reduced risk of colorectal cancer and hip fractures. One arm of the study reviewed the same outcomes in women taking unopposed estrogen and found that these women had no increased risk of cardiac events and a trend toward decrease in breast cancer compared to women on combined therapy.
Some of the data contradicted prior large-scale observational studies, and, therefore, many physicians have changed their practice regarding HT to center more on the relief of short-term symptoms of estrogen deprivation, including hot flushes, sleeplessness, and vaginal atrophy. Although reappraisals of the study have focused on its flaws, current opinion suggests that initiation early in menopause is associated with a good risk/benefit ratio, with preference for the transdermal route. Nonetheless, the current recommendations from numerous organizations, including the American College of Obstetricians and Gynecologists, are that HT should only be used for the short-term relief of menopausal symptoms and should be individually tailored to a woman’s need for treatment (Box 41.2).
HT in women with prior history of breast and endometrial cancer is controversial. Currently, prospective studies are underway using low-dose HT in women with a prior history of limited-lesion, successfully treated breast cancer. Similar studies in women with prior treated limited-lesion endometrial cancer have been completed and show no increased risk of recurrence for estrogen users.
BOX 41.2 Contraindications to Hormone Therapy
• Undiagnosed abnormal genital bleeding
• Known or suspected estrogen-dependent neoplasia except in appropriately selected patients
• Active deep vein thrombosis, pulmonary embolism, or a history of these conditions
• Active or recent arterial thromboembolic disease (stroke and myocardial infarction)
• Liver dysfunction or liver disease
• Known or suspected pregnancy
• Hypersensitivity to hormone therapy preparations
ALTERNATIVES TO HORMONE THERAPY
Because of the controversy surrounding HT, many women are seeking alternative therapies. When counseling patients, physicians must take a holistic approach. Most women seek relief of the most common symptom of menopause—hot flushes—but as noted above, menopause affects women in different ways. As women age, their risk for heart disease begins to rise and, therefore, it is important to advocate heart-healthy lifestyle changes. Likewise, preventive counseling about osteoporosis, as previously discussed, should also be included. Alternative therapies for the short-term treatment of common symptoms of menopause include the following:
• Soy and isoflavones may be helpful in the short-term (≤2 years) treatment of vasomotor symptoms. Given the possibility that these compounds may interact with estrogen, these agents should not be considered free of potential harm in women with estrogen-dependent cancers.
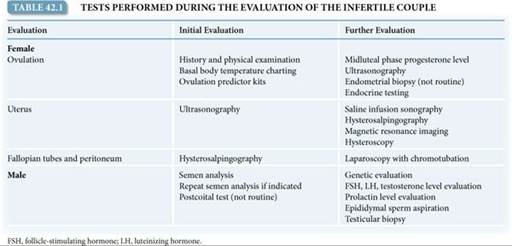
• St. John’s wort may be helpful in the short term (during the initial evaluation of infertility. It is important to recognize that more than one factor may be involved in a couple’s infertility; thus, comprehensive evaluation is often warranted (Table 42.1). As with any medical condition, a careful history and evaluation should reveal factors that may be involved in a couple’s infertility, such as medical disorders, medications, prior surgeries, pelvic infections or pelvic pain, sexual dysfunction, and environmental and lifestyle factors (e.g., diet, exercise, tobacco use, and drug use).
The timing of the initial evaluation depends primarily on the age of the female partner and a couple’s risk factors for infertility. Because there is a decline in fecundity with advancing maternal age, women over the age of 35 years may benefit from a preliminary evaluation after only 6 months of attempted conception. The initial assessment and treatment of infertility is commonly provided by an obstetrician–gynecologist. More specialized evaluation and treatment may be performed by a reproductive endocrinologist.
Ovulation
A history of regular, predictable menses strongly suggests ovulatory cycles. Furthermore, many women experience characteristic symptoms associated with ovulation and the production of progesterone: unilateral pelvic discomfort (mittelschmerz), fullness and tenderness of the breasts, decreased vaginal secretions, abdominal bloating, slight increase in body weight, and occasional episodes of depression. These changes rarely occur in anovulatory women. Therefore, a history of regular menses with associated cyclic changes may be considered presumptive evidence of ovulation.
Secretion of progesterone by the corpus luteum dominates the luteal phase of the menstrual cycle and persists if conception occurs. Progesterone acts on the endocervix to convert the thin, clear endocervical mucus into a sticky mucoid material. Progesterone also changes the brain’s thermoregulatory center set point, resulting in a basal body temperature rise of approximately 0.6°F. In the absence of pregnancy, involution of the corpus luteum is associated with an abrupt decrease in progesterone production, normalization of the basal body temperature, shedding of the endometrium, and the commencement of menstruation.

FIGURE 42.2. Steps in successful conception: ovulation, production of viable sperm and fertilization, development of the zygote, early embryonic development, and implantation of the embryo into the endometrium.
Ovulation Tests
Two tests provide indirect evidence of ovulation and can help predict the timing of ovulation. Basal body temperature measurement reveals a characteristic biphasic temperature curve during most ovulatory cycles (Fig. 42.3). Special thermometers are available for this use. Upon awakening in the morning, the patient must take her temperature immediately before any physical activity. The temperature drops at the time of menses and then rises 2 days after the peak of the luteinizing hormone (LH) surge, coinciding with a rise in peripheral levels of progesterone. Oocyte release occurs 1 day before the first temperature elevation, and the temperature remains elevated for up to 14 days. This test for ovulation is readily available, although it is cumbersome to use; it can retrospectively identify ovulation and the optimal time for intercourse, but it can be difficult to interpret. Urine LH kits are also used to prospectively assess the presence and timing of ovulation based on increased excretion of LH in the urine. Ovulation occurs approximately 24 hours after urinary evidence of the LH surge. However, due to the pulsatile nature of LH release, an LH surge can be missed if the test is performed only once daily.
Other diagnostic tests assess ovulation using serum progesterone levels and the endometrial response to progesterone. A midluteal phase serum progesterone level can be used to retrospectively assess ovulation. A value above 3 ng/mL implies ovulation; however, values between 6 and 25 ng/mL may occur in a normal ovulatory cycle. Due to the pulsatile nature of hormone secretion, a single low progesterone assessment should be repeated. Another diagnostic procedure is the luteal phase endometrial biopsy. The identification of secretory endometrium consistent with the day of the menstrual cycle confirms the presence of progesterone; hence, ovulation is implied. However, this procedure is invasive, and histologic assessment of the endometrium does not reliably differentiate infertile and fertile women and may interrupt an early pregnancy. Therefore, the endometrial biopsy is no longer performed to assess ovulation or the endometrium.

FIGURE 42.3. Biphasic basal body temperature pattern that occurs with an ovulatory cycle. HSG, hysterosalpingography; LH, luteinizing hormone.
Ovulatory Dysfunction
If oligo-ovulation (sporadic and unpredictable ovulation) or anovulation (absence of ovulation) is established, usually based on clinical and laboratory data, further testing is indicated to determine the underlying cause. A common cause of ovulatory dysfunction in reproductive-age women is polycystic ovary syndrome (PCOS); other causes include thyroid disorders and hyperprolactinemia. Women with PCOS often present with oligomenorrhea and signs of hyperandrogenism such as hirsutism, acne, and weight gain (see Chapter 40).
Some infertile women present with amenorrhea, and this usually signifies anovulation. Important causes of amenorrhea include pregnancy (a pregnancy test should always be given), hypothalamic dysfunction (usually stress-related), ovarian failure, and obstruction of the reproductive tract. Laboratory testing for ovulatory dysfunction may include assessment of serum levels of human chorionic gonadotropin (hCG), thyroid-stimulating hormone, prolactin, total testosterone, dehydroepiandrosterone sulfate, follicle-stimulating hormone (FSH), LH, and estradiol. Treatment of the etiology of ovulatory dysfunction may lead to resumption of ovulation and improved fertility.
Anatomic Factors
The pelvic anatomy should be assessed as a part of the infertility evaluation. Abnormalities of the uterus, fallopian tubes, and peritoneum can all play a role in infertility.
Uterus
Uterine abnormalities are commonly not sufficient to cause infertility; these disorders are usually associated with pregnancy loss. However, assessment of the uterus is particularly important if there is a history that causes concern, such as abnormal bleeding, pregnancy loss, preterm delivery, or previous uterine surgery. Potential uterine abnormalities include leiomyomas, endometrial polyps, intrauterine adhesions, and congenital anomalies (such as a septate, bicornuate, unicornuate, or didelphic uterus), as shown in Figure 42.4. Assessment of the uterus and endometrial cavity can be accomplished with several imaging techniques; sometimes, a combination of modalities is necessary to best assess pelvic anatomy (Box 42.1).
Fallopian Tubes and Peritoneum
The fallopian tubes are dynamic structures that are essential for ovum, sperm, and embryo transport and fertilization. At ovulation, the fimbriated end of the fallopian tube picks up the oocyte from the site of ovulation or from the pelvic culde-sac. The oocyte is transported to the ampullary portion of the fallopian tube where fertilization occurs (see Fig. 42.2). Subsequently, a zygote and then an embryo are formed. At 5 days following fertilization, the embryo enters the endometrial cavity, where implantation into the secretory endometrium occurs, followed by further embryo growth and development.

FIGURE 42.4. Uterine abnormalities. (A) X-ray hysterosalpingogram confirms a didelphic uterus, with paired contrastfilled cervical canals (arrowheads) and uterine cavities (arrows). (B) Three-dimensional sonogram indicating a septate uterus. The endometrium is separated into two components (short arrows) and the uterine fundus (long arrow) has a smooth external contour. Courtesy of Dr. Beryl Benacerraf. (From Doubilet PM, Benson CB. Atlas of Ultrasound in Obstetrics and Gynecology. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:291.)
The fallopian tubes and pelvis can be evaluated with hysterosalpingography (HSG) or laparoscopy.
Hysterosalpingogram
There are several important characteristics of a normal HSG (Fig. 42.5). The uterine cavity should be smooth and symmetrical; indentations or irregularities of the cavity suggest the presence of leiomyomas, endometrial polyps, or intrauterine adhesions. The proximal two thirds of the fallopian tube should be thin, approximately 1 mm in thickness. The distal third comprises the ampulla and should appear dilated in comparison to the proximal portion of the tube. Free spill of dye from the fimbria into the pelvis is appreciated as the cul-de-sac and other structures such as bowel are outlined by the accumulating dye. Failure to observe dispersion of dye through a fallopian tube or throughout the pelvis suggests the possibility of pelvic adhesions that restrict normal fallopian tube mobility. Examples of abnormal HSGs are shown in Figure 42.6.
BOX 42.1 Procedures Used in the Evaluation of Female Infertility
Transvaginal Ultrasonography: Provides assessment of the cervix, uterus, and ovaries.
3D Transvaginal Ultrasonography: Provides reconstructed coronal views of the uterus, allowing easier diagnosis of uterine abnormalities.
Saline Infusion Sonography: Provides assessment of the myometrium, endometrium, and adnexa; sometimes used in conjunction with magnetic resonance imaging.
Hysterosalpingography: Provides information about the uterus and fallopian tubes’ structure and function.
Magnetic Resonance Imaging: Provides information about uterine abnormalities, including fibroids.
Hysteroscopy: Provides in vivo assessment and treatment of intrauterine abnormalities identified by imaging studies, such as removal of small leiomyomata, polyps, and adhesions.
Laparoscopy: Provides in vivo assessment and treatment of pelvic abnormalities, including endometriosis. Saline infusion of the fallopian tubes can also be performed to test their patency.
Pelvic Adhesions
Pelvic adhesions that affect the fallopian tubes or peritoneum may occur because of pelvic infection (e.g., pelvic inflammatory disease and appendicitis); endometriosis; or abdominal or pelvic surgery, particularly tubal surgery. The sequelae of any of these processes or events can include fallopian tube scarring and obstruction. Pelvic infections are usually associated with sexually transmitted infections that cause acute salpingitis; commonly implicated organisms are Chlamydia trachomatis and Neisseria gonorrhea (see Chapter 29). Endometriosis occurs with higher frequency in infertile women compared with fertile women and can cause scarring and distortion of the fallopian tubes and other pelvic organs (see Chapter 31).
Hysteroscopy and Laparoscopy
The HSG detects approximately 70% of anatomic abnormalities of the genital tract. When there are abnormalities, further diagnostic evaluation and treatment can be performed with hysteroscopy and laparoscopy. Hysteroscopy evaluates the endometrium and the architecture of the uterine cavity. Laparoscopy assesses pelvic structures, including the uterus, ovaries, and fallopian tubes as well as the pelvic peritoneum. During laparoscopy, chromotubation should be performed: similar to the HSG, a catheter is placed in the uterus, and colored dye is injected into the uterus while tubal patency and function is directly assessed by laparoscopy. Laparoscopy also allows the diagnosis and treatment of any pelvic abnormalities, such as adhesions and endometriosis.

FIGURE 42.5. A hysterosalpingogram demonstrating a patent female reproductive tract with normal anatomy.

FIGURE 42.6. Abnormal hysterosalpingograms. (A) Bilateral hydrosalpinges (dilated fallopian tubes) with distal obstruction at the fimbriated ends; no free spill of dye seen. (B) Bilateral proximal tubal occlusion; uterus overdistended with radiopaque dye.
MALE INFERTILITY
Because male infertility is common, it is important to also perform a semen analysis when evaluating the female partner.
Semen Analysis
The semen specimen is usually obtained by masturbation after 2 to 3 days of abstinence; frequent ejaculation may lower the sperm concentration. It is important to collect the entire ejaculate, because the first part contains the greatest density of sperm. Analysis of the specimen should be performed within 1 hour of ejaculation (see Table 42.1). The standard semen analysis evaluates the quantity and quality of seminal fluid, sperm concentration, and sperm motility and morphology. Normal semen measurements have been established by the World Health Organization (Table 42.2). A normal semen analysis excludes a male cause for infertility in more than 90% of heterosexual couples. Certain abnormalities identified by the semen analysis are associated with specific etiologies of male infertility (Table 42.3). Sperm function can be further evaluated with specialized diagnostic tests, but these tests are not routinely used.

Besides the semen analysis, the postcoital test originally used to assess the viability of sperm contained in ovulatory cervical mucus is now considered of limited diagnostic and therapeutic usefulness. Furthermore, conventional fertility treatments, such as intrauterine insemination (IUI) and in vitro fertilization (IVF), bypass any abnormalities of the cervix or cervical mucus.
Causes of Male Infertility
If the results of the semen analysis are abnormal, the test should be repeated in 1 to 2 weeks. Persistent abnormalities in the semen necessitate further investigation. The male partner should be evaluated by a urologist or reproductive endocrinologist who specializes in male infertility. Occasionally, male infertility may be the presenting sign of a serious medical condition, such as testicular cancer or a pituitary tumor. Etiologies of male infertility include congenital, acquired, and systemic disorders that can be grouped into the following categories: hypothalamic–pituitary disease that causes gonadal dysfunction (1%–2%), testicular disease (30%–40%), post-testicular defects that cause disorders of sperm transport or ejaculation (10%–20%), and unexplained infertility (40%–50%).
Spermatogenesis
Abnormalities in spermatogenesis are a major cause of male infertility. Unlike oocytes, which undergo development in a cyclic fashion, sperm are being produced constantly by the testes. As sperm develop within the germinal epithelium of the testis, they are released into the epididymis where maturation occurs before ejaculation. Sperm production and development takes approximately 70 days. Therefore, abnormal results of the semen analysis reflect events that occurred more than 2 months before the specimen collection. Alternatively, a minimum of 70 days is required to observe changes in sperm production following initiation of any therapy.

Endocrinology
Further evaluation of the infertile male includes endocrine testing. Endocrine evaluation is appropriate for individuals with abnormal sperm concentrations or signs of androgen deficiency. Serum testosterone, FSH, and LH levels will identify primary hypogonadism (low testosterone, or elevated FSH and LH) or secondary hypogonadism (low testosterone, FSH, and LH). A low LH level in the presence of oligospermia (sperm concentration < 5 million/mL) and a normal testosterone level may indicate exogenous steroid use. A serum prolactin level should be assessed in men with low testosterone levels.
Genetics
Genetic abnormalities may affect sperm production or transport. Genetic testing is indicated in men with azoospermia (no sperm) and severe oligospermia. The most common abnormalities identified include gene mutations in the cystic fibrosis transmembrane conductase regulator (CFTR), somatic and sex chromosome abnormalities, and microdeletions of the Y chromosome. Men with mutations in one or both copies of the CFTR gene often exhibit congenital bilateral absence of the vas deferens or other obstructive defects but have no pulmonary symptoms. A karyotype may reveal abnormalities, such as Klinefelter syndrome (47 XXY) or chromosome inversions and translocations. Special testing must be performed to search for Y chromosome microdeletions because they are not detected by routine karyotype analysis; these microdeletions are associated with altered testicular development and spermatogenesis. If a genetic condition is identified, genetic counseling is strongly recommended prior to conception. Advanced paternal age has been shown to be associated with increased rates of spontaneous autosomal-dominant mutations with risk progressively increasing with increasing age; however, currently there are no standardized protocols in place to screen for these. There is also data to suggest increased miscarriage rates and pregnancy loss rates with paternal age over 40 years.
Diagnostic Procedures
Men with azoospermia can be further evaluated by two diagnostic procedures. If an obstructive process is suspected (obstructive azoospermia), then sperm should accumulate just before the obstruction. For example, men with congenital absence of the vas deferens or those who underwent a vasectomy have a swollen epididymis where constant production of sperm results in a small collection. Percutaneous epididymal sperm aspiration and microsurgical epididymal sperm aspiration procedures can retrieve motile, healthy sperm. If no obstruction is present (nonobstructive azoospermia) and a testicular abnormality is suspected, a testicular biopsy may identify a few sperm present in the seminiferous tubules. With either procedure, small numbers of sperm are obtained compared with a normal ejaculated specimen. These retrieved sperm are used to fertilize a single oocyte obtained from the female partner via IVF, a technology called intracytoplasmic sperm injection (ICSI).
UNEXPLAINED INFERTILITY
For some couples, comprehensive evaluation of both partners does not identify an etiology for their infertility. Specifically, test results identify a normal semen analysis, evidence of ovulation, a normal uterine cavity, and patent fallopian tubes. Approximately 15% of infertile couples are considered to have unexplained infertility. This diagnosis usually signifies the presence of one or more mild abnormalities in the highly orchestrated sequence of events that results in successful conception. These abnormalities may lie below the level of detection of current tests. These couples have a low rate of spontaneous conception, approximately 1% to 3% each month; this rate is influenced by the age of the female partner and the duration of infertility. If laparoscopy is performed on the female partner, subtle abnormalities such as pelvic adhesions and mild endometriosis may be identified and treated. However, it is reasonable to proceed with medical treatment of infertility without performing laparoscopy.
TREATMENT
A couple’s infertility may be related to one or several abnormalities in one or both partners. Numerous medical, surgical, and assisted reproductive technology (ART) therapies are available for treating the infertile couple. For couples with unexplained infertility, empiric treatment may overcome the negative effects of one or more mild abnormalities. These couples, as well as the majority of infertile couples, tend to proceed through fertility treatment in a stepwise fashion, starting with conservative and then with more aggressive ovarian stimulation, inseminations, and eventually proceeding to IVF (explained below).
Surgical procedures are indicated in certain circumstances. If a woman presents with pelvic pain and infertility, laparoscopy may be used to identify and treat the cause of her pelvic pain as well as evaluate pelvic anatomy from a fertility standpoint. If an obstructed fallopian tube is identified with HSG, it may be possible to correct the obstruction surgically. For these operations to be successful, the endosalpinx must be healthy. If the tubal damage is significant enough to impair gamete transport, then an ART such as IVF may be necessary. When indicated, abnormalities of the uterine cavity, such as submucosal leiomyomas, endometrial polyps, intrauterine adhesions, and a septum, can be surgically corrected with a hysteroscopic procedure.
Ovarian Stimulation
Ovulation induction is indicated in women with anovulation or oligo-ovulation. However, any identified condition associated with ovulatory disorders should be treated before initiating ovulation induction therapy. Such conditions include thyroid disorders, hyperprolactinemia, PCOS, and high levels of stress (including psychologic stress, intense exercise, and eating disorders).
Clomiphene
The most commonly used medication for ovulation induction is clomiphene citrate. Clomiphene is a selective estrogen receptor modulator that competitively inhibits estrogen binding to the estrogen receptors at the hypothalamus and pituitary. The anti-estrogen effects of clomiphene induce gonadotropin release from the pituitary, which stimulates follicle development in the ovaries. Clomiphene is administered daily for 5 days in the follicular phase of the menstrual cycle, starting between cycle days 3 and 5. If ovulation does not occur, the dose is increased for the subsequent month. Women with ovulatory disorders associated with oligomenorrhea may not have regular menses and may require a progesterone-induced menses to start their clomiphene cycle. When used in women who are already ovulatory, clomiphene may stimulate development of several mature follicles.
With clomiphene, ovulation can occur between 5 and 12 days after the last pill, and it can be monitored in several ways. Urine LH kits can be used each day starting on cycle day 10; when ovulation occurs, exposure to sperm through intercourse or IUI should occur. Transvaginal ultrasound performed on cycle day 11 or 12 may identify a developing follicle. When ultrasound is used and a mature follicle is identified (average diameter > 18 mm), ovulation can be triggered by administering a subcutaneous injection of hCG. The exogenous hCG effectively simulates the LH surge and ovulation occurs; this practice enables the proper timing of intercourse or insemination. Some couples prefer to not monitor ovulation and have regular midcycle intercourse. In this situation, a serum progesterone level on cycle day 21 may suggest that ovulation has occurred. The use of clomiphene is associated with a 10% risk of multiple gestations, the majority of which are twin gestations, and a small risk of ovarian hyperstimulation and cyst formation.
Controlled Ovarian Hyperstimulation
Alternatively, exogenous gonadotropins can be given to stimulate follicular development. The use of gonadotropins is commonly referred to as controlled ovarian hyperstimulation (COH). This therapy aims to achieve monofollicular ovulation in anovulatory women (particularly those who do not respond to clomiphene) and ovulation of several mature follicles in other infertile women. Available preparations include purified human menopausal gonadotropins (FSH and LH are extracted from the urine of postmenopausal women) and recombinant human FSH. The dose of medication is tailored to a woman’s age, body weight, infertility diagnosis, and response to previous fertility treatments. These medications are more potent than clomiphene and require frequent monitoring of follicle growth that usually includes transvaginal ultrasonography and serum estradiol measurements. When at least one mature follicle is identified (average follicle diameter of 18 mm and serum estradiol concentration > 200 pg/mL), hCG is administered to trigger ovulation. Timed inseminations are commonly performed within 12 to 36 hours from hCG administration. The risks of this therapy include ovarian hyperstimulation syndrome, which can require intensive therapy; a 25% incidence of multiple gestations; and an increased risk of ectopic pregnancy.
Intrauterine Insemination
Before performing IUI, an ejaculated semen specimen is washed to remove prostaglandins, bacteria, and proteins. The sperm is then suspended in a small amount of medium. To perform IUI, a speculum is inserted into the vagina, the specimen is placed in a thin flexible catheter, and the catheter is advanced through the cervix into the uterine cavity where the specimen is deposited (Fig. 42.7). A total motile sperm count (concentration multiplied by motility) of at least 1 million must be present, insofar as pregnancy is rarely achieved with lower counts. In couples with infertility, and particularly in those with mild male infertility, pregnancy rates are increased with IUI. However, more severe male infertility may necessitate the use of ART to achieve pregnancy. If the male partner is azoospermic and no sperm are identified during testicular biopsy, or if a woman does not have a male partner, IUI with an anonymous donor sperm is an available alternative.

FIGURE 42.7. Intrauterine insemination technique.
Assisted Reproductive Technologies
All fertility procedures that involve manipulation of gametes, zygotes, or embryos to achieve conception comprise the ARTs. In the United States, IVF accounts for more than 99% of all ART procedures. The process of IVF involves ovarian stimulation to produce multiple follicles, retrieval of the oocytes from the ovaries, oocyte fertilization in vitro in the laboratory, embryo incubation in the laboratory, and transfer of embryos into a woman’s uterus through the cervix. The required medications for IVF include gonadotropins to stimulate follicle development, a gonadotropin-releasing hormone analogue (agonist or antagonist) to prevent premature ovulation during follicle development, and hCG to initiate the final maturation of oocytes prior to their retrieval. As with COH, the IVF process necessitates careful monitoring of ovarian response with transvaginal ultrasonography and serum estradiol measurements.
Depending on the etiology of infertility, fertilization can be achieved “naturally,” by placing tens of thousands of sperm together with a single oocyte, or with ICSI (Fig. 42.8). Therefore, IVF provides the tools necessary to bypass the normal mechanisms of gamete transport, fertilization, and embryo transport. After oocyte retrieval, daily progesterone supplementation is necessary to insure the appropriate secretory changes in the endometrium and to support the potential pregnancy; if conception occurs, supplementation is continued until at least 10 weeks of gestation.

FIGURE 42.8. Intracytoplasmic sperm injection. (A) An oocyte is being held by a holding pipette. The injection pipette contains a single sperm. (B) The injection pipette has penetrated the zona pellucida and plasma membrane of the oocyte, and the sperm has been microinjected into the oocyte. (Courtesy of James H. Liu, MD. From Fritz MA, Dodson WC, Meldrum D, Johnson JV. Infertility. In: Precis, An Update in Obstetrics and Gynecology: Reproductive Endocrinology. 3rd ed. Washington, DC: American College of Obstetricians and Gynecologists; 2007:161.)
Indications for IVF include absent or blocked fallopian tubes, tubal sterilization, failed surgery to achieve tubal patency, severe pelvic adhesions, severe endometriosis, poor ovarian response to stimulation, oligo-ovulation, severe male factor infertility, unexplained infertility, and failed treatment with less aggressive therapies. Success rates with IVF depend on the etiology of infertility and the age of the female partner. The chance of conception with one IVF cycle depends on the number and quality of embryos transferred and can be as high as 40% to 50%, with a 30% rate of multiple gestations and at least a 15% rate of spontaneous abortion. In certain situations, embryo quality and number and, thus, chance of conception can be improved using donor gametes.
COUNSELING
A team approach is frequently helpful in ensuring that patients receive an adequate workup and appropriate counseling. Counseling of patients who are treated with ART should include information regarding the risk of multiple gestation, ethical issues surrounding multifetal pregnancy reduction, the stress associated with undergoing ART, and adoption. Clinicians should also be familiar with any state laws regarding infertility services and treatment and insurance coverage insofar as the cost of these treatments is very high and most often covered in a limited way or not at all by third-party payers.
Clinical Follow-Up
Because the couple has excellent health care coverage, they agree to undergo a comprehensive workup, which demonstrates a normal Day 21 progesterone, normal hysterosalpingogram, and a normal semen analysis. When given the option of expectant management or clomiphene ovulation induction with intrauterine insemination, they opt for the latter and achieve pregnancy in 3 months. They ultimately deliver a healthy baby girl at term.
thePoint Visit http://thepoint.lww.com/activate for an interactive USMLE-style question bank and more!