Chapter 13 Multifetal Gestation
This chapter deals primarily with APGO Educational Topic Area:
TOPIC 20 MULTIFETAL GESTATION
Students should be able to distinguish different types of multifetal gestation based on embryologic development and ultrasound findings.
They should be able to describe the appropriate management and possible complications of multifetal gestation.Clinical Case
At the time of a gestational dating ultrasound examination at 17 weeks of pregnancy, a twin pregnancy is noted. While initially excited with this news, your patient and her partner have a number of questions and concerns about pregnancy and delivery.
The overall incidence of multiple gestations in the United States is almost 3%, but these pregnancies account for a disproportionate share of perinatal morbidity and mortality. The natural rate of twinning is approximately 1 in 90 and is slightly higher in African Americans than in whites. The rate is rising as a result of an increase in maternal age and the more frequent use of assisted reproductive technologies (ARTs) and ovulation induction agents. Since 1980, there has been a 70% increase in the frequency of twins and a 400% increase in triplet and higher order births. It is estimated that 43% of triplet and higher order gestations result from ART procedures and 38% from ovulation induction; spontaneous conception accounts for the remainder. Although the exact mechanism is not known, monozygotic twinning is also higher in pregnancies conceived using ART.
Twin gestations can be characterized as dizygotic (fraternal) or monozygotic (identical). Dizygotic twins occur when two separate ova are fertilized by two separate sperms. Monozygotic twins result from the division of the fertilized ovum after conception. There is a marked difference in the incidence of twinning in various populations, almost exclusively the result of the incidence of dizygotic twinning.
The incidence of monozygotic twinning is fairly constant around the world, at approximately 1 in 250 pregnancies. Increasing maternal age and increasing parity are independent risk factors for dizygotic twinning, and rates are higher among mothers of families with twins. NATURAL HISTORY
NATURAL HISTORY
The following describes the various developmental sequences possible when the monozygotic conceptus separates into twins (also called chorionicity), as shown in Figure 13.1:
• Diamnionic/Dichorionic: If division of the conceptus occurs within 3 days of fertilization, each fetus will be surrounded by an amnion and chorion. There may be two separate placentas or one “fused” placenta.
• Diamnionic/Monochorionic: If division occurs between the fourth and eighth day following fertilization, the chorion has already begun to develop, whereas the amnion has not. Therefore, each fetus will later be surrounded by an amnion, but a single chorion will surround both fetuses.
• Monoamnionic/Monochorionic: In 1% of monozygotic gestations, division occurs between days 9 and 12, after development of both the amnion and the chorion, and the twins will share a common sac.
• Division thereafter is incomplete, resulting in the development of conjoined twins. The fetuses may be fused in a number of ways, with the most common involving the chest and/or abdomen. This rare condition is seen in approximately 1 in 70,000 deliveries. This condition is associated with a mortality rate of up to 50%.
RISKS OF MULTIFETAL GESTATION
Multifetal pregnancies are associated with increased perinatal morbidity, three to four times that of a comparable singleton pregnancy. The most significant cause of morbidity is preterm labor and delivery.
Compared with singleton pregnancies, which are delivered at an average gestational age of 40 weeks, twins are delivered at an average of 35 weeks, triplets at 32 weeks, and quadruplets at an average of 30 weeks.
Thus, with each additional fetus, the length of gestation is decreased by approximately 2 to 3 weeks. Other associated morbidities include intrauterine growth restriction, hydramnios (in approximately 10% of multiple gestations, predominantly monochorionic gestations), preeclampsia (three times more frequent in twin gestations), congenital anomalies, postpartum hemorrhage, placental abruption, and umbilical cord accidents. Both spontaneous abortions and congenital anomalies are approximately twice as common in multiple gestations (Table 13.1).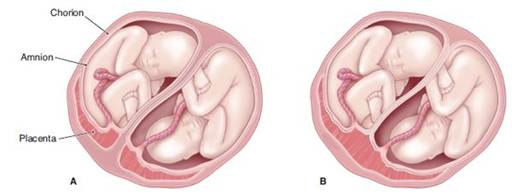

FIGURE 13.1. Chorionicity in twin pregnancies. (A) Two placentas, two amnions, two chorions: diamniotic dichorionic. (B) One placenta, two amnions, two chorions: diamniotic/dichorionic. (C) One placenta, two amnions, one chorion: diamniotic/monochorionic. (D) One placenta, one amnion, one chorion: monoamniotic/monochorionic. (Based on American College of Obstetricians and Gynecologists. Having Twins. Patient Education Pamphlet AP092. Washington, DC: ACOG; 2004.)
Because of the higher rates of multiple gestation, particularly higher-order multiple births (more than two), counseling for infertility treatment should include a discussion of the risks associated with multiple gestation and the option of multifetal pregnancy reduction. This procedure is defined as a first-trimester or early second-trimester termination of one or more fetuses in a multifetal gestation, to increase the chances of survival of the remaining fetuses and decrease long-term morbidity for the delivered infants. Of course, the primary approach to this problem is to try to prevent higher order multiple births. Physicians providing infertility treatment should follow guidelines designed to limit the risk of multiple gestation in the setting of ART or ovulation induction.
Twin–Twin Transfusion Syndrome
As development of a monochorionic gestation progresses, various vascular anastomoses between the fetuses can develop that, in turn, can lead to a condition known as twin–twin transfusion syndrome (TTTS). In this circumstance, through arteriovenous anastomoses, there is net flow from one twin to another, often with untoward pregnancy outcomes. The so-called donor twin can have impaired growth, anemia, hypovolemia, and other problems. The recipient twin can develop hypervolemia, hypertension, polycythemia, and congestive heart failure as a result of this preferential transfusion. A secondary manifestation involves amniotic fluid dynamics. The hypervolemia in the recipient twin leads to an increase in urinary output and, in turn, to an increase in amniotic fluid volumes (hydramnios). The opposite effect may occur in the donor twin—hypovolemia leads to decreased urinary output and, possibly, a decrease in amniotic fluid volume (oligohydramnios). Hydramnios in the one twin compounds the risk of preterm labor already present for multifetal pregnancies. Traditionally, serial removal of amniotic fluid from the sac of the recipient twin has been the only treatment option associated with improved survival. However, endoscopic intrauterine laser ablation of the vascular anastomoses has met with greater success in treating this difficult problem, especially in more severe cases. When available, fetoscopic laser photocoagulation has largely replaced serial amnioreduction as first-line therapy for TTTS. Other vascular abnormalities include the absence of one umbilical artery, which may be associated in 30% of cases with other congenital problems, especially renal agenesis. A single umbilical artery is seen in approximately 3% to 4% of twins, compared with 0.5% to 1% of singletons.
alt=image>
Monoamniotic Twins
In 1% of monozygotic twins, division occurs between 9 and 12 days following fertilization, resulting in both fetuses occupying a single sac composed of inner amnion and outer chorion.
The risk of entanglement of the umbilical cords, with subsequent fetal death, is considerable. Traditionally, arbitrary cesarean delivery (after steroids) at approximately 32 weeks of gestation was the usual management. Recent management, involving hospitalization at 26 to 28 weeks, steroid administration, and fetal heart rate monitoring several times daily, has allowed for the prediction of impending difficulty with cord entanglement. Pregnancies have been permitted to extend beyond 32 weeks. As a result, issues involving prematurity occur less frequently and tend to be less serious when delivery occurs later in gestation.Death of One Fetus
Multiple gestations, especially high-order gestations, are at increased risk for losing one or more fetuses remote from delivery. As summarized by the American College of Obstetricians and Gynecologists, no fetal monitoring protocol has been shown to predict most of these losses. Consensus about the preferred antepartum surveillance method and management once demise has occurred has not been reached. Whereas some advocate immediate delivery of the remaining fetus(es), if the death was the result of an abnormality of the fetus itself (i.e., rather than maternal or uteroplacental pathology) and the pregnancy is remote from term, expectant management may be appropriate.
The most difficult cases are those in which the fetal demise occurs in one fetus of a monochorionic twin pair. Because virtually 100% of monochorionic placentas contain vascular anastomoses that link the circulations of the two fetuses, the surviving fetus is at significant risk for sustaining damage caused by the sudden, severe, and prolonged hypotension that occurs at the time of the demise or by embolic phenomena that occur later. By the time the demise is discovered, the greatest harm has most likely already been done, and there may not be any benefit in immediate delivery, especially if the surviving fetuses are very preterm and otherwise healthy.
In such cases, allowing the pregnancy to continue may provide the most beneficial outcome. DIAGNOSIS
Most multifetal pregnancies are diagnosed using ultrasound. On a clinical basis, twin pregnancy should be suspected when the uterine size is large for the calculated gestational age. A difference of 4 cm or more between the weeks of gestation and the measured fundal height should prompt evaluation with ultrasound to detect the cause (e.g., inaccurate gestational age, multiple gestation, hydramnios, gestational trophoblastic disease, and pelvic tumor).
Serial ultrasound assessments have shown that only 50% of twin pregnancies detected in the first trimester result in the delivery of viable twins. The other 50% of cases deliver a single fetus because of intrauterine demise and ultimate resorption of one embryo/fetus (vanishing twin syndrome). During the first ultrasonographic examination that confirms a twin gestation, chorionicity should be determined because the potential morbidity and mortality associated with a monochorionic gestation is different from that of a dichorionic gestation. Chorionicity can be determined by ultrasound with almost 100% certainty as early as 9 to 10 weeks of gestational age.
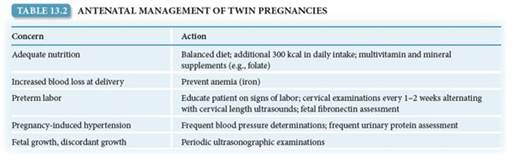
ANTENATAL MANAGEMENT
Once the diagnosis of twin pregnancy has been made, and chorionicity has been assigned, subsequent antenatal care addresses each of the potential concerns for mother and fetus, as listed in Table 13.2. Although the maternal blood volume is greater with a twin gestation than with a singleton pregnancy, the anticipated blood loss at delivery is likewise also greater. Anemia is more common in these patients, and a balanced diet during pregnancy, which may include increased intake of iron, folate, and other micronutrients, is important. Because of the increased risk of preterm labor in multiple gestations, careful attention to detection of uterine contractions is important, and the patient should be cautioned about signs and symptoms of preterm labor, such as abdominal pain, low back pain, a thin or increase in vaginal discharge, and vaginal bleeding. Cervical examinations to detect early effacement and dilation are often done every 1 to 2 weeks beginning in the midtrimester. When available, serial ultrasound assessments of endovaginal cervical length may be interspersed with the vaginal examinations.
Although assessment of fetal fibronectin may aid in predicting preterm delivery in women, it has limited predictive value in multifetal gestations. At each visit, blood pressure should be evaluated, and, if elevated, urine protein should be assessed. Beginning at 30 to 32 weeks, daily fetal kick counts are usually begun to help assess fetal well-being.
Ultrasonography
With multifetal gestations, periodic ultrasonographic examination should be performed approximately every 3 to 4 weeks, beginning at 16 to 18 weeks of gestation. At the initial evaluation, special attention is given to identification of fetal anomalies, and this is especially so in monochorionic gestations, among which such abnormalities are more frequently seen. A careful ultrasound examination to identify fetal anomalies is performed at 16 to 20 weeks, at which time fetal size permits such diagnoses. At each subsequent examination, growth of each fetus is assessed, and an estimate of amniotic fluid volume is made. Discordant growth is defined as a 15% to 25% reduction in the estimated fetal weight of the smallest fetus compared with the largest. Additional antenatal surveillance, such as the nonstress test or biophysical profile, is often used when there is growth restriction of one or more fetuses, discordant growth, or another high-risk situation such as maternal medical comorbidity.
INTRAPARTUM MANAGEMENT
Not surprisingly, the average duration of pregnancy is inversely related to the number of fetuses. The average length of pregnancy in twin gestations is about 35 weeks. Many consider the optimal time for twins to be delivered as between 38.0 and 39.6 weeks. Before that time, amniocentesis for fetal maturity assessment is generally recommended. Induction of labor or cesarean delivery is usually scheduled because the risk of fetal demise increases at 40.0 weeks and beyond.
Intrapartum management is largely determined by the presentation of the twins. In general, if the first (presenting) twin is in the cephalic (vertex) presentation, labor is allowed to progress to vaginal delivery, whereas if the presenting twin is in a position other than cephalic, cesarean delivery is often performed. During labor, the heart rate of both fetuses is monitored separately. Approaches to the delivery of twins vary, depending on gestational age or estimated fetal weight, presentation of the twins, and the experience of the attending physician. Regardless of the delivery plan, access to full obstetric, anesthetic, and pediatric services is mandatory because cesarean delivery may be required on short notice. About 40% of all twin pairs enter labor with both in the cephalic presentation. After delivery of the first twin, if the second fetus remains cephalic, vaginal delivery of the second twin generally proceeds smoothly. With proper monitoring of the second twin, there is no urgency in accomplishing the second delivery.
alt=image>
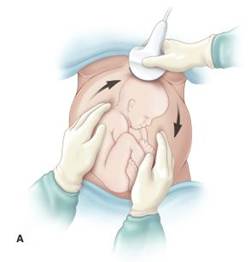
FIGURE 13.2. Delivery of second twin. (A) External cephalic version. (B) Breech extraction (internal podalic version).
Delivery Maneuvers
If the second twin is presenting in any way other than cephalic (40% of all twin deliveries), there are two primary manipulations that may affect vaginal delivery. The first is external cephalic version. Using ultrasonographic visualization, the fetus is gently guided into the cephalic presentation by abdominal massage and pressure (Fig. 13.2A). The second maneuver is breech extraction, in which the physician reaches a hand into the uterine cavity, grasps the lower extremities of the fetus, and gently delivers the infant via breech delivery (see Fig. 13.2B). Delivering the second twin via cesarean delivery is another management option but is usually reserved for cases in which there is an inability to safely deliver the second twin vaginally.
Complications
The possibility of a prolapsed umbilical cord must always be borne in mind when delivery of twins is to be accomplished. Twin gestations in which the first twin is in the breech presentation (20% of all twin deliveries) are most often delivered via cesarean delivery. Some clinicians and their patients plan for cesarean delivery unless both fetuses are in a cephalic presentation.
For patients with three or more fetuses, because of the potential for presentation of different fetal parts, delivery is accomplished by planned cesarean delivery in most cases.
Postpartum, the overdistended uterus may not contract normally, leading to uterine atony and postpartum hemorrhage (see Chapter 12).
Clinical Follow-Up
After the diagnosis of multiple fetuses is made, it is important to carefully review the management of pregnancy and delivery with your patient and her partner. Management of patients with a multiple gestation requires considerable planning and close follow-up, and they should be made aware of the differences in caring for a patient with multiple fetuses versus those with one fetus. Although outcome is generally favorable, a close relationship and more frequent visits are necessary. You should encourage your patient and her partner to ask questions and express concerns throughout her pregnancy.
thePoint Visit http://thepoint.lww.com/activate for an interactive USMLE-style question bank and more!
More on the topic Chapter 13 Multifetal Gestation:
- Triplet and Higher-Order Pregnancy
- Invasive Prenatal Diagnosis in Multiple Pregnancy
- Optimal Antenatal Care in Multiple Pregnancy
- Induction in special situations