Chapter 12 Postpartum Hemorrhage
This chapter deals primarily with APGO Educational Topic Area:
TOPIC 27 POSTPARTUM HEMORRHAGE
Students should be able to list the risk factors for postpartum hemorrhage (PPH) and to outline a basic approach to evaluation and management of immediate and delayed PPH.
Clinical Case
After a lengthy labor, a 22-year-old patient delivers her second child at term. Her infant is healthy, with good Apgar scores. Soon after her delivery, and before the placental expulsion occurs, sudden, profuse hemorrhage is noted.
It is estimated that, worldwide, 140,000 women die of postpartum hemorrhage (PPH) each year—1 every 4 minutes. More than half of all maternal deaths occur within 24 hours of delivery. In addition to death, serious morbidity may follow PPH. Sequelae include adult respiratory distress syndrome, coagulopathy, shock, loss of fertility, and pituitary necrosis (Sheehan syndrome).
The prevalence of PPH is about 4%. It can be sudden and profuse, or blood loss can occur more insidiously. PPH has been traditionally defined as a delivery-associated blood loss in excess of 500 mL for vaginal delivery and 1,000 mL for cesarean birth; however, these estimates actually represent the average blood loss for each mode of delivery, respectively. The estimation of blood loss is subjective, introducing wide variance and inaccuracy.
Additionally, the same absolute volume loss for a patient weighing 50 kg may have vastly different effects than it would for someone weighing 75 kg or for a patient with triplets versus a singleton. Thus, it is likely more appropriate and meaningful to use physiologic and objective criteria in defining clinical hemorrhage. Criteria in use include a 10% drop in hematocrit, need for transfusion, and signs and symptoms along the spectrum of physiologic effects of blood loss, described below.
For descriptive purposes, PPH is termed “primary” (also called early) if it occurs within 24 hours of delivery and “secondary” (or late) if it occurs between 24 hours and (usually) 12 weeks after delivery.
Primary PPH is of much greater importance, insofar as secondary PPH is generally much less serious in nature. RECOGNITION AND EARLY DETECTION
RECOGNITION AND EARLY DETECTION
PPH is not a diagnosis but, rather, a critically important sign that often occurs without warning and in the absence of risk factors. When present, however, these factors warrant heightened awareness about the risk of PPH (Box 12.1). Maternal hemodynamic responses to blood loss should also be monitored, insofar as these responses are indicators of well-being, volume deficit, and prognosis. The loss of 10% to 15% (500 mL for an average patient with a singleton pregnancy) of blood volume may be tolerated with no signs or symptoms. As blood loss approaches 20%, the first signs of intravascular depletion manifest, including tachycardia, tachypnea, and delayed capillary refill, followed by orthostatic changes and narrowed pulse pressure (due to elevated diastolic pressure secondary to vasoconstriction with maintenance of systolic pressure). Beyond approximately 30% volume loss, breathing and heart rate further increase, and overt hypotension develops. Finally, with profound blood loss above 40% to 50%, oliguria, shock, coma, and death may occur.
BOX 12.1 Risk Factors for Postpartum Hemorrhage
Prolonged labor
Augmented labor
Rapid labor
History of postpartum hemorrhage
Episiotomy, especially mediolateral
Preeclampsia
Overdistended uterus (macrosomia, multiple gestation, and hydramnios)
Operative delivery
Asian or Hispanic ethnicity
Chorioamnionitis
Data from Stones RW, Paterson CM, Saunders NJ. Risk factors for major obstetric haemorrhage. Eur J Obstet Gynecol Reprod Biol. 1993;48(1): 15–18; and Combs CA, Murphy EL, Laros RK. Factors associated with hemorrhage in cesarean deliveries. Obstet Gynecol. 1991;77(1):77–82.
The source and etiology of bleeding should be identified as soon as possible, and targeted interventions applied in order to minimize morbidity and prevent mortality.
The most common cause of PPH is uterine atony, representing about 80% of cases. Retained placenta, genital tract trauma, lacerations, and coagulation disorders are other causes. Hematomas can occur anywhere in the lower genital tract. Ruptured uterus and inverted uterus are rare but serious causes of PPH. GENERAL MANAGEMENT OF PATIENTS
PPH is an unequivocal emergency; all available resources should be mobilized immediately upon its recognition. A general approach to management is outlined in Box 12.2. Because most cases of PPH are caused by uterine atony, the uterus should be palpated abdominally, seeking the soft, “boggy” consistency of the relaxed uterus. If this finding is confirmed, oxytocin infusion should be increased and either methylergonovine maleate or prostaglandins administered if excessive bleeding continues.
Other questions that may help direct assessment include the following:
• Was expulsion of the placenta spontaneous and apparently complete? (Think: retained placental fragment?)
• Were forceps or other instrumentation used in delivery? (Think: laceration?)
• Was the baby large or the delivery difficult or precipitous? (Think: uterine atony?)
• Were the cervix and vagina inspected for lacerations?
• What was the admission or baseline hematocrit?
• Is the blood clotting? (Think: coagulopathy?)
While the cause of the hemorrhage is being identified, general supportive measures should be initiated (see Box 12.2).
BOX 12.2 Management of the Patient with Postpartum Hemorrhage
General Measures
Evaluate excessive bleeding immediately
Assess overall patient status
Notify other members of obstetrics team (i.e., obtain help!)
Monitor and maintain circulation
• Establish intravenous (IV) access: two large bore
• Type and cross-match blood
• Begin/increase crystalloid infusion
• Assess for clotting or check coagulation profile
Review clinical course for probable cause
• Any difficulty removing placenta?
• Were forceps used?
• Other predisposing factors?
Have operating room (OR) and personnel on standby
Evaluation: Perform in Rapid Succession
Assess hemodynamic status
Bimanual examination: assess for atony
• May palpate for retained placental fragments
• May palpate uterine wall for rupture
Inspect perineum, vulva, vagina, and cervix
• Identify lacerations, hematomas, inversions
• Recruit assistance for exposure
• You or assistant may re-inspect placenta
Assess clotting
Targeted Interventions
Atony
Immediate bimanual massage
Administer uterotonics (with requisite precautions)
• Oxytocin—IV: 10–40 units/1 L normal saline or lactated Ringer solution, continuous
• Methylergonovine—intramuscular (IM): 0.2 mg IM; may repeat in 2–4 hours
• 15-Methyl PGF2α—IM 0.25 mg every 15–90 minutes for up to 8 doses
• Dinoprostone—Suppository: rectal; 20 mg every 2 hours
• Misoprostol—800–1,000 µg rectally; one dose
• Intrauterine tamponade—Bakri balloon, packing
Operative measures
Uterine compression sutures
Sequential arterial ligation or selective arterial embolization
Hysterectomy
Retained Placenta
Manual removal; manage atony as above
Ultrasound assessment/guidance to assure complete removal
Suction curettage—ideally performed with ultrasound guidance in OR
Maintain suspicion for accreta—additional intervention required
Genital Tract Lacerations and Hematomas
Repair lacerations immediately
Exposure critical—get assistance, move to OR
No blindly placed sutures
Packing may be necessary
Observe stable, asymptomatic hematomas
Coagulopathy
Appropriate factor replacement
Identify underlying cause
Hemorrhage, infection, amniotic fluid embolism, other
Such measures include large-bore intravenous access; rapid crystalloid infusions; type, cross-match, and administration of blood or blood components as needed; periodic assessment of hematocrit and coagulation profile; and monitoring of urinary output.
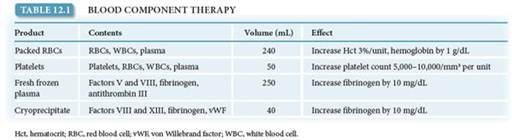
The judicious use of blood component therapy is key to management. Recently, there has been a shift in philosophy regarding transfusion of blood products, with greater willingness to intervene earlier and prevent coagulopathy rather than to delay treatment until coagulopathy is diagnosed. The mainstay of blood replacement therapy is packed red blood cells (PRBCs), with other components used as indicated for various disorders of the clotting cascade. Depending on the clinical scenario, the use of laboratory measurements to guide transfusion of plasma, cryoprecipitate, and platelets may be reasonable. However, in the setting of severe, ongoing hemorrhage (4 or more units of PRBCs needed over 1 hour or 10 or more units over 12 to 24 hours), the current recommendation is to transfuse blood products in a 1:1:1 ratio (i.e., for each unit of PRBCs transfused, 1 unit of fresh frozen plasma and 1 unit of random donor platelets should also be transfused). See Table 12.1 for an outline of blood products and their effects.BOX 12.3 Precautionary Measures to Prevent or Minimize Postpartum Hemorrhage
Before Delivery
Baseline hematocrit
Blood type and screen (cross-match for very high risk)
Intravenous access
Obtain baseline coagulation studies and platelet count, if indicated
Identify risk factors
In Delivery Room
Avoid excessive traction on umbilical cord
Use forceps and vacuum judiciously
Inspect placenta for complete removal
Perform digital exploration of uterus (if indicated)
Active management of the third stage
Visualize cervix and vagina
Remove all clots in uterus and vagina before transfer to recovery area
In Recovery Area
Closely observe patient for excessive bleeding Continue uterotonic agents
Frequently palpate uterus with massage Determine vital signs frequently
The management of PPH is greatly facilitated if patients at high risk are identified and preliminary preparations are made before the bleeding episode. Box 12.3 reviews such preliminary, precautionary measures.
MAJOR CAUSES AND THEIR MANAGEMENT
Uterine Atony
Ordinarily, the uterine corpus contracts promptly after delivery of the placenta, constricting the spiral arteries in the newly created placental bed and preventing excessive bleeding. This muscular contraction, rather than coagulation, prevents excessive bleeding from the placental implantation site. When contraction does not occur as expected, the resulting uterine atony leads to PPH.
Conditions that predispose to uterine atony include those in which there is extraordinary enlargement of the uterus (e.g., hydramnios and multiple fetuses), abnormal labor (both precipitous and prolonged or augmented by oxytocin), and conditions that interfere with contraction of the uterus (e.g., uterine leiomyomata and magnesium sulfate). The clinical diagnosis of atony is based largely on the tone of the uterine muscle on palpation. Instead of the normally firm, contracted uterine corpus, a softer, more pliable—often called “boggy”—uterus is found. The cervix is usually open. Frequently, the uterus contracts briefly when massaged, only to become relaxed again when the manipulation ceases. Because hemorrhage can occur in the absence of atony, other etiologies must be sought in the presence of a firm fundus.
Management of Uterine Atony
Management of uterine atony is both preventive and therapeutic. Active management of the third stage of labor (the interval between the delivery of the fetus and delivery of the placenta) has been shown to reduce the incidence of PPH by as much as 70%. The protocol for management of the third stage includes oxytocin infusion (usually 20 units in 1 L of normal saline infused at 200 to 500 mL/hour) initiated immediately following delivery of the infant or its anterior shoulder, gentle cord traction, and uterine massage. Some physicians do not begin oxytocin infusion until after delivery of the placenta to avoid placental entrapment; however, there is no firm evidence that the rates of entrapment are higher with active management than with other strategies.
Immediate breastfeeding may also enhance uterine contractility and, thus, reduce blood loss.Once uterine atony is diagnosed, management can be categorized as medical, manipulative, or surgical. Management must be individualized in cases of severe uterine atony, taking into account the extent of hemorrhage, the overall status of the patient, and her future childbearing desires (see Box 12.2). Bimanual uterine massage alone is often successful in causing uterine contraction, and this should be done while preparations for other treatments are under way (Fig. 12.1).
Uterotonic Agents
Uterotonic agents include oxytocin, methylergonovine maleate, misoprostol (an analogue of prostaglandin E1), dinoprostone (an analogue of prostaglandin E2), and 15-methyl prostaglandin F2α, administered separately or in combination. Methylergonovine maleate is a potent uterotonic agent that can cause uterine contractions within several minutes. It is always given intramuscularly, because rapid intravenous administration can lead to dangerous hypertension, and its use is often avoided in those with hypertensive disorders. Although it should be avoided or used with extreme caution in those with cardiac, pulmonary, liver, or renal diseases, 15-methyl prostaglandin F2α may be given intramuscularly or directly into the myometrium. Dinoprostone may be given by rectal suppository. More recently, misoprostol has been used for treatment and prevention of PPH. These prostaglandins result in strong uterine contractions. Typically, oxytocin is given prophylactically, as noted previously; if uterine atony occurs, the infusion rate is increased, and additional agents are given sequentially. Uterotonic agents are only effective for uterine atony. If the uterus is firm, the use of these agents is not necessary and other causes of bleeding should be explored.

FIGURE 12.1. Management of uterine atony with manual massage. One hand gently compresses the uterus through the abdominal wall. The other is inserted so that the pressure can be placed against the anterior lower uterine segment.
Occasionally, uterine massage and uterotonic agents are unsuccessful in bringing about adequate uterine contraction, and other measures must be used. Some practitioners use intrauterine compression with in utero packing or placement of a balloon compression device (e.g., Bakri, BT-cath, and Foley catheters) as a means of halting blood loss while preserving the uterus.
Surgical Management
Surgical management of uterine atony may include uterine compression sutures (B-Lynch or multiple squares), sequential arterial ligation (ascending or descending branches of the uterine, utero-ovarian, then internal iliac arteries), selective arterial embolization, and hysterectomy (Fig. 12.2). Very high success rates have been noted with surgical compression techniques, with consequent decreases in the use of hysterectomy and iliac artery ligations, both of which are associated with high rates of morbidity. Additional advantages of compression techniques include rapid execution and preservation of fertility.


FIGURE 12.2. Surgical treatment of atonic uterine hemorrhage. (A) Ligation of the uterine artery. The artery crosses over the ureter and is ligated beyond this point at the uterine corpus. (B) “B-Lynch” suture.
As in other clinical circumstances, recombinant factor VIIa is reserved for life-threatening hemorrhage despite virtually all other therapies. Extremely expensive, such therapy also increases the likelihood of subsequent and serious thrombosis.
Lacerations of the Lower Genital Tract
Lacerations of the lower genital tract are far less common than uterine atony as a cause of PPH, but they can be serious and require prompt surgical repair. Predisposing factors include instrumented delivery, manipulative delivery such as a breech extraction, precipitous labor, presentations other than occiput anterior, and macrosomia.
Although minor lacerations to the cervix are common in delivery, extensive lacerations and those that are actively bleeding usually require repair. To minimize blood loss caused by significant cervical and vaginal lacerations, all patients with any predisposing factors and any patient in whom blood loss soon after delivery appears to be excessive despite a firm and contracted uterus should have a careful repeat inspection of the lower genital tract. This vaginal examination may require assistance to allow adequate visualization. As a rule, repair of these lacerations is usually not difficult, if adequate exposure is provided.
Lacerations of the vagina and perineum (first-degree through fourth-degree vaginal and periurethral lacerations) are not common causes of substantial blood loss, although the continued steady loss of blood, which may come from deeper lacerations, may become so significant that their timely repair is requisite. Periurethral lacerations may be associated with sufficient edema to occlude the urethra, causing urinary retention; a Foley catheter for 12 to 24 hours usually alleviates this problem.
Retained Placenta
Normally, separation of the placenta from the uterus occurs because of cleavage between the zona basalis and the zona spongiosa facilitated by uterine contraction. Once separation occurs, expulsion is caused by strong uterine contractions. Retained placenta can occur when either the process of separation or the process of expulsion is incomplete. Predisposing factors to retained placenta include a previous cesarean delivery, uterine leiomyomata, prior uterine curettage, and accessory (succenturiate) placental lobe.
Placental tissue remaining in the uterus can prevent adequate contractions, leading to atony and excessive bleeding. After expulsion, every placenta should be inspected to detect missing placental cotyledons, which may remain in the uterus.
Sheared or abruptly ending surface vessels may indicate an accessory, or succenturiate, placental lobe. If retained placenta is suspected—either because of apparently absent cotyledons or because of excessive bleeding—it can often be removed by inserting two fingers through the cervix into the uterine cavity and manipulating the retained tissue downward into the vagina. If this is unsuccessful, or if there is uncertainty regarding the cause of hemorrhage, an ultrasound examination of the uterus can be helpful. Curettage with a suction apparatus and/or a large, sharp curette may be used to remove the retained tissue. Care must be exercised to avoid perforation through the uterine fundus. An additional concern is that overvigorous curettage can lead to Asherman syndrome, in which intrauterine adhesions can lead to a variety of complications, including menstrual irregularities, infertility, and future pregnancy loss.
Abnormal Placental Separation
Placental tissue may also remain in the uterus because separation of the placenta from the uterus may not occur normally. At times, placental villi penetrate the uterine wall to varying degrees, collectively called placenta accreta. More specifically, abnormal adherence of the placenta to the superficial lining of the uterus is termed placenta accreta, penetration into the uterine muscle itself is called placenta increta, and complete invasion through the thickness of the uterine muscle is termed placenta percreta. If this abnormal attachment involves the entire placenta, no part of the placenta separates. Much more commonly, however, attachment is not complete, with a portion of the placenta separating and the remainder attached. Major, life-threatening hemorrhage can ensue.
If a portion of the placenta separates and the remainder stays attached, hysterectomy is often required; however, an attempt to separate the placenta by curettage or other means of controlling the bleeding (such as surgical compression or sequential arterial ligation) may be appropriate in trying to avoid a hysterectomy in a woman who desires more children.
Other Causes
Hematomas
Hematomas can occur anywhere from the vulva to the upper vagina as a result of delivery trauma. Hematomas may also develop at the site of episiotomy or perineal laceration. Hematomas may occur without disruption of the vaginal mucosa such as when the fetus or forceps causes shearing of the submucosal tissues without mucosal tearing.
Vulvar or vaginal hematomas are characterized by exquisite pain with or without signs of shock. Hematomas that are ≤5 cm in diameter and are not enlarging can usually be managed expectantly by frequent evaluation of the size of the hematoma and close monitoring of vital signs and urinary output. Application of ice packs can also be helpful. Larger and enlarging hematomas must be managed surgically. If the hematoma is at the site of episiotomy, the sutures should be removed, and a search made for the actual bleeding site, which is then ligated. If it is not at the episiotomy site, the hematoma should be opened at its most dependent portion and drained; the bleeding site identified, if possible; and the site closed with interlocking hemostatic sutures. Often, specific sources of bleeding cannot be identified. If this is the case, surgical management involves “oversewing” the mucosal edges of the vaginal wall with interlocking suture. Drains and vaginal packs are often used to prevent reaccumulation of blood. It should be noted that large amounts of blood can dissect and accumulate along tissue planes, especially into the ischiorectal fossa, precluding easy identification. This may be seen in those with trauma involving the vaginal side walls and sulci. Thus, careful monitoring of hemodynamic status is important in identifying those with occult bleeding.
Coagulation Defects
Virtually, any congenital or acquired abnormality in blood clotting can lead to PPH. Abruptio placentae, amniotic fluid embolism, sepsis, and severe preeclampsia are obstetric conditions associated with disseminated intravascular coagulopathy. The treatment of coagulation disorders involves correction of the coagulation defect with appropriate factor replacement.
It also should be recalled that profuse hemorrhage itself can lead to coagulopathy, thus creating a vicious cycle of bleeding.
Amniotic Fluid Embolism
Amniotic fluid embolism is a rare, sudden, and sometimes fatal obstetric complication thought to be caused primarily by entry of amniotic fluid into the maternal circulation. Significant biochemical, as well as physical, mediators are thought to be involved in the development of the clinical scenario, which unfolds as five findings that occur in sequence: 1) respiratory distress, 2) cyanosis, 3) cardiovascular collapse, 4) hemorrhage, and 5) coma. Amniotic fluid embolism also often results in severe coagulopathy. Treatment is directed toward total support of the cardiovascular and coagulation systems.
Uterine Inversion
Uterine inversion is a rare condition in which the uterus literally turns inside out, with the top of the uterine fundus extending through the cervix into the vagina and sometimes even past the introitus (Fig. 12.3). Hemorrhage with uterine inversion is characteristically severe and sudden. Treatment includes manual replacement, which frequently requires administration of an agent that causes uterine relaxation (e.g., sublingual nitroglycerin, terbutaline, magnesium sulfate, and halogenated general anesthetics). If manual replacement fails, surgery is required.
Uterine Rupture
Uterine rupture should be distinguished from dehiscence of a low transverse incision, insofar as the clinical connotations are quite different. A uterine rupture is a frank opening between the uterine cavity and the abdominal cavity. A uterine dehiscence is a “window” covered by the visceral peritoneum. Significantly higher rates of maternal and fetal morbidity, and even maternal mortality, occur in cases of overt rupture.

FIGURE 12.3. Manual replacement of an inverted uterus.
Rupture can occur at the site of a previous cesarean delivery or other surgical procedure involving the uterine wall— from intrauterine manipulation or trauma, from congenital malformation (e.g., small uterine horn), or spontaneously. Abnormal labor, operative delivery, and placenta accreta can lead to rupture. Surgical repair is required, with the specific approach tailored to reconstruct the uterus, if possible. Care depends on the extent and site of rupture, the patient’s current clinical condition, and her desire for future childbearing. Rupture of a previous cesarean delivery scar often can be managed by revision of the edges of the prior incision, followed by primary closure. In addition to the myometrial disruption, consideration must be given to the neighboring structures, such as the broad ligament, parametrial vessels, ureters, and bladder. Regardless of the patient’s wishes for the avoidance of hysterectomy, this procedure may be necessary in a life-threatening situation. Careful assessment in the face of maternal hemodynamic changes and monitoring other signs, such as acute abdominal pain, change in abdominal contour, nonreassuring fetal heart patterns, and loss of fetal station, are critical in early detection and intervention in such cases.
 PREVENTION
PREVENTION
Several preventive strategies can help curtail the incidence of delivery-associated hemorrhage, and many are quite effective. Active management of the third stage of labor, which involves manual removal of the placenta and the administration of a uterotonic agent, has been shown to reduce the incidence of hemorrhage. In addition to preventing many cases of uterine atony, this approach will also reduce the incidence of uterine inversion. The incidence of retained placenta is not increased with these techniques.
Finally, all obstetric units and practitioners must have the facilities, personnel, and equipment in place to manage PPH properly. Clinical drills to enhance the management of patients with maternal hemorrhage are also helpful.
Clinical Follow-Up
Postpartum hemorrhage is a serious complication seen in obstetrics. Clinicians must have a systematic plan for management. Diagnosis and treatment typically are generally simultaneous. A team approach, involving obstetricians, nurses, and anesthesia, is necessary to minimize morbidity for the patient.
thePoint Visit http://thepoint.lww.com/activate for an interactive USMLE-style question bank and more!
More on the topic Chapter 12 Postpartum Hemorrhage:
- Chapter 12 Postpartum Hemorrhage
- Chorioamnionitis
- Chapter 11 Postpartum Care
- Chapter 13 Multifetal Gestation
- 8 Gestational Complications
- Chapter 12 Reproduction
- 13 Endocrine Disorders of Pregnancy
- Screening and Diagnosis of Complications of Shared Placentation
- Anaemia in pregnancy
- Changes in the respiratory system