Chorioamnionitis
The term chorioamnionitis applies to the inflammation of the fetal membranes and the placenta as a result of the entry of microorganisms usually from the maternal lower genital tract into the amniotic sac.
The membranes bear the brunt of the inflammatory process rather than the placenta. Maternal polymorphs first infiltrate the lower pole of the amniotic sac followed by their accumulation in the intervillous space immediately beneath the chorionic plate, the so-called intervillositis (36). Inflammatory cells are rarely seen elsewhere in the intervillous space and villitis is very rarely seen except in listeriosis (36) and vertical transmission of blood-borne maternal infections. Later in the process, fetal leucocytes migrate out from fetal vessels in the chorionic plate, and subsequently an angiitis of the umbilical cord vessels occurs with migration of fetal leucocytes into the Wharton's jelly, the so-called funisitis, a marker of more generalized FSIRS (37), probably mediated in part by widespread endothelial injury (Figure 17.1) (38).FSIRS is associated with hypotension, neonatal seizures, need for intubation, meconium aspiration syndrome, multiorgan dysfunction, chorioamnionitis, preterm delivery, a clinical diagnosis of hypoxic ischaemic encephalopathy or neonatal encephalopathy (39-41), IVH (42), white matter damage, periventricular leucomalacia, bronchopulmonary dysplasia, and cerebral palsy in the term and near-term infant (Figure 17.1) (43). It is probably the most common antecedent of low Apgar scores and other indicators of neonatal depression (41, 44). Fetal demise from overwhelming sepsis or growth restriction may occur (45), as well as polymicrogyria (a migratory disorder of the cerebral cortex) (46). In a meta-analysis, clinical chorioamnionitis had a relative risk (RR) of 1.9 (95% confidence interval (CI) 1.4-2.5) for development of cerebral palsy in preterm infants and a RR of 4.7 (95% CI 1.316.2) in term infants (47). However, the literature is relatively silent on the risk of cerebral palsy associated with intrauterine infection before the peripartum period in term infants and on the contribution of extrauterine infection.
Chorioamnionitis is a strong risk factor for neonatal encephalopathy and cerebral palsy (48). It accounts for 11-22% of cases of cerebral palsy in term and near-term infants, and carries an odds ratio of 9.3 for unexplained cerebral palsy (49). Fetal exposure to chorioamnionitis has two potent noxious elements, namely, hyperthermia and inflammation. Current diagnosis of clinical chorioamnionitis is based on maternal fever of at least 38.0°C, and any two of uterine fundal tenderness, purulent and/or foulsmelling vaginal discharge, fetal tachycardia, maternal tachycardia, raised inflammatory markers including C-r eactive protein, and white cell count. However, 10% or less of cases with histological chorioamnionitis had signs of clinical chorioamnionitis. Uterine tenderness is subjective and abolished after epidural analgesia. Purulent or offensive vaginal discharge is subjective and attenuated by antiseptic gels and lubricants used for vaginal examination during labour. Labour is an inflammatory process and is associated with increase in the levels of inflammatory markers. Collectively, the criteria used for the diagnosis of clinical chorioamnionitis are
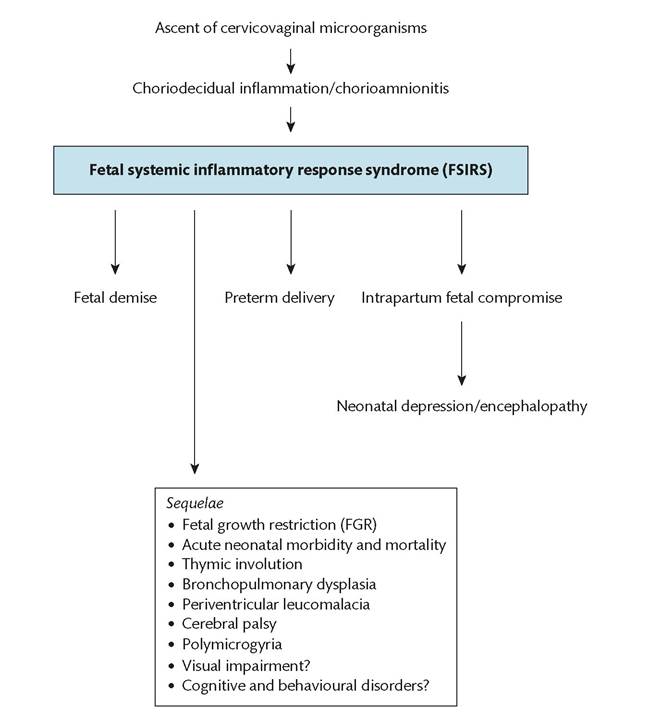
Figure 17.1 Short-, medium-, and long-term complications of Chorioamnionitis.
insensitive and reflects the fact that the fetal compartment is sequestrated and not contiguous with the maternal. In the authors' institution, maternal temperature and fetomaternal tachycardia are the most commonly used criteria to make the diagnosis of clinical chorioamnionitis.
More on the topic Chorioamnionitis:
- 8 Gestational Complications
- Chapter 17 Premature Rupture of Membranes
- 5 Normal Labor and Delivery, Operative Delivery, and Malpresentations
- Chapter 9 Abnormal Labor and Intrapartum Fetal Surveillance
- General characteristics of innate immunity and fetal host response to infection
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020
- Chapter 12 Postpartum Hemorrhage
- Chapter 15 Preterm Labor
- Chapter 16 Third-Trimester Bleeding