Chronic kidney disease
CKD is often clinically and biochemically silent until renal function has deteriorated significantly. Symptoms are unusual until the GFR declines to less than 25% of normal and more than 50% of renal function can be lost before the SCr concentration rises above 120 μmol/ L.
However, women who become pregnant with a SCr concentration above 120 μmol∕L are at increased risk of an accelerated decline in renal function and poor pregnancy outcome (10, 52, 53). Women with the most severe prepregnancy CKD have the greatest risk of adverse pregnancy outcome and the greatest risk of a pregnancy- related decline in renal function, especially if associated with hypertension (10, 52-55). Clinical management of pregnant women with CKD aims to prevent pregnancy-induced harm to the mother's renal function and CKD-induced harm to the developing fetus.CKD is classified into five stages according to the level of renal function, (estimated glomerular filtration rate; eGFR) (Table 14.3) (56). In a prepregnancy Norwegian population, the overall prevalence of women with CKD was 3.3% (54). CKD stage 1 affected 2.4%, CKD 2, 0.8%, and CKD stage 3, 0.1% (54). There were no cases of CKD stages 4 and 5, which in other populations affects between 1:500 and 1:1000 women of childbearing age (20-39 years). Due to reduced fertility and an increased rate of early miscarriage, ongoing pregnancy in women with CKD stage 4 or 5 is rare. Conversely, up to 20% of women who develop early pre-eclampsia (≤30 weeks' gestation), especially those with heavy proteinuria, are found to have previously unrecognized CKD (57).
Women with CKD are less able to make the renal adaptations of healthy pregnancy. Their inability to boost renal hormones leads to normochromic normocytic anaemia (reduced erythropoietin), attenuated plasma volume expansion (reduced renin), and vitamin D deficiency (reduced 1,25 dihydroxycholecalciferol).
The gestational rise in GFR is blunted in women with moderate renal impairment and usually absent in those with a SCr concentration greater than 200 μmol∕L (2.26 mg/dL) (58, 59).The impact of pregnancy on maternal chronic kidney disease
Mild renal impairment during pregnancy (CKD stages 1-2)
Most women with CKD who become pregnant have mild renal dysfunction and pregnancy usually succeeds without affecting renal prognosis (Table 14.3). A case-controlled study of 360 women with primary glomerulonephritis and only mild prepregnancy renal dysfunction (SCr outcome (>24 weeks) and impact on maternal renal function
| SCr μmol∕L (mg∕dL) | Rate of fetal growth restriction (%) | Rate of preterm delivery (%) | Rate of preeclampsia (%) | Perinatal deaths (%) | Loss of >25% renal function | ||
| Pregnancy (%) | Persists postpartum (%) | ESRF in 1 year (%) | |||||
| 2.0) | 75 | 90 | 60 | 10 | 70 | 50 | 35 |
| Dialysis | >90 | 90 | 75 | 50a | N/A | N/A | N/A |
ESRF, end-stage renal failure.
Estimates are based on literature from 1 985 to 2011, with all pregnancies attaining at least 24 weeks' gestation.
a If conceived on dialysis, 50% of infants survival; if conceived before introduction of dialysis, there is 75% infant survival (10).
management of CKD in pregnancy relate to the management of associated clinical features rather than the type of renal disease.
Regular monitoring of maternal renal function (serum creatinine and urea levels, not eGFR), full blood count, blood pressure, MSU for infection and proteinuria, and when appropriate ultrasound imaging of renal tracts will identify most subclinical pathological changes and allow timely intervention to optimize perinatal and maternal renal outcome (Table 14.6).Prepregnancy preparation for women with chronic kidney disease
Ideally, all women with CKD should be made aware of the effects that pregnancy may have on their own long-term renal function, and of the risks of adverse pregnancy outcome, before they conceive (Table 14.5). Women with CKD often have amenorrhoea, but may still ovulate and should be considered fertile. Sexually active women with CKD who do not wish to become pregnant should therefore take appropriate contraceptive measures that consider clinical comorbidities.
Folic acid 400 mcg daily should be given as usual before conception until 12 weeks’ gestation. Low-dose aspirin (50-150 mg/day) should be started in early pregnancy to reduce the risk of pre-eclampsia and improve perinatal outcome (62). Regular drugs should be reviewed so that fetotoxic drugs (e.g. angiotensin-converting enzyme
Table 14.5 Odds ratio for pre-eclampsia, small for gestational age, or preterm birth by kidney function and blood pressure
| Blood pressure | eGFR >90 mL/min | eGFR 75-89 mL∕min | eGFR 60-74 mL∕min |
| 140/ 90 mmHg | 1.82 (95% CI 1.12-2.97; P = 0.015) (n = 304) | 2.58 (95% CI 1.40-4.75; P blood pressure | Consider prophylactic antibiotics. Drain obstruction as necessary |
| Nephrolithiasis | Renal colic, ureteric obstruction | Involve a urologist. Ureteroscopy or magnetic resonance urography can be used to remove or treat stones, while avoiding radiation exposure | |
| Diabetic nephropathy | Renal function, hypertension, and proteinuria | Maintain good control of maternal glucose, blood pressure, and screen for urinary infection | |
| Lupus nephritis | Distinguish from pre-eclampsia | Ask patient if it feels like a lupus flare. Check double-stranded DNA levels. Link with rheumatologist or nephrologist | |
| Dialysis | Mimic physiological changes of pregnancy | Almost daily haemodialysis allows mimicking of gestational physiological change | |
| Renal transplant | Pre-eclampsia, fetal growth restriction, deteriorating graft function | Delay pregnancy until stable graft function and allow immunosuppression to low-normal levels |
pregnancy, but much of the monitoring of women with CKD stages 1-2 can be done by primary care physicians.
Optimal management of pregnant women with CKD will often involve the combined expertise of specialists in obstetrics, nephrology, urology, fetal medicine, and neonatology. Impressive improvements in perinatal outcome over recent decades have been driven by advances in these specialties. Maternal renal conditions that have a genetic basis require specialist fetal medicine and genetic advice.
Specific kidney conditions during pregnancy
Primary glomerulonephritis
The histological type of primary glomerulonephritis does not affect pregnancy outcome as much as the clinical parameters of hypertension, level of renal impairment, proteinuria, and recurrent urinary infections (10). Severe vascular lesions on renal biopsy are associated with increased perinatal mortality, which probably reflects maternal clinical parameters (63). On the rare occasion that sudden renal impairment (SCr >120 pmol/L), or an active urinary sediment with red cell casts occurs before 34 weeks' gestation in the absence of pre-eclampsia, a renal biopsy may detect a glomerular lesion that would benefit from targeted therapy. However, in pregnancy the plethoric kidney is more prone to bleed and more awkward to biopsy, so should only be undertaken by an experienced operator (64). New-onset heavy proteinuria (nephrotic range, >5 g/24 hours) could be managed with a trial of steroids and in the absence of a prompt clinical response, a renal biopsy should be considered.
After 34 weeks, early delivery becomes an option. Postpartum, pregnancy- induced proteinuria and renal impairment will improve, therapeutic options broaden, and clinical management, including renal biopsy, becomes less difficult.Immunoglobulin A nephropathy
Immunoglobulin (Ig)-A nephropathy is the commonest primary glomerulonephritis in young people and is consequently highly represented in pregnant women (65). IgA nephropathy presents with macroscopic haematuria, often during an acute gastrointestinal or respiratory tract illness. The diagnosis is made by histological examination of a renal biopsy that shows IgA deposits in the glomerular mesangium (65). The clinical course is variable, but progression towards end-stage renal failure is more common in the presence of hypertension, proteinuria, and severe histological lesions (65). Initial treatment is aimed at controlling hypertension and proteinuria with an angiotensin- converting enzyme inhibitor or angiotensin II receptor blocker, but both agents are fetotoxic and need to be replaced by other antihypertensive agents during pregnancy. Thromboprophylaxis with low-molecular-weight heparin is prudent if there is proteinuria (PCR >100 mg/mmol). Progressive IgA nephropathy has been treated with immunosuppression with limited success.
Pregnancy and renal outcomes for women with IgA nephropathy follow the same general principles stated for all women with CKD. Those with preconception CKD stage 3 or 4, (but not CKD stage 1 or 2), hypertension, nephrotic range proteinuria, and the most severe histological lesions on renal biopsy are more likely to have an accelerated decline in renal function postpartum compared with women who have IgA nephropathy, but don't become pregnant (66). Similarly, these clinical features increase the risk of pre-eclampsia, fetal growth restriction, and preterm labour (67).
Henoch-Schonlein purpura nephritis
Henoch-Schonlein purpura (HSP) is a small vessel vasculitis that predominantly affects children.
Renal involvement (HSP nephritis) is present in approximately 50% of cases and shares histological similarities with IgA nephropathy (65). Women who had HSP nephritis as children usually make a good recovery, but are at an increased risk of recurrent proteinuric hypertension during their pregnancies (68). Immunosuppressive treatment appears to be of no proven benefit. Management aims to control hypertension and reduce the risk of pre-eclampsia with low-dose aspirin.Lupus nephritis
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disorder directed against nuclear antigens, which predominantly affects young women (69). Lupus nephritis affects up to 50% of women with SLE and is often subclinical (70). Active lupus nephritis is characterized by an increase serum creatinine concentration, active urinary sediment (haematuria, red cell casts, and leucocytes), proteinuria, and hypertension (69). Lupus nephritis runs a relapsing and remitting course and during pregnancy is best managed by a multidisciplinary team of obstetricians, nephrologists, and rheumatologists.
Women who have well-controlled SLE before conception are at low risk of an adverse pregnancy outcome (71). Furthermore, it is rare for women with SLE to develop lupus nephritis for the first time during pregnancy (72). The risk of a flare of lupus nephritis during pregnancy is influenced by clinical disease activity at conception and predicted using subclinical markers of immunological activity (72, 73). These include elevated levels of anti-double-stranded (ds) DNA and anti-C1q antibodies and low levels of complement C3 and C4 (73). The risk of pre-eclampsia, fetal growth restriction, and preterm labour is driven by the usual prepregnancy clinical factors that drive an adverse pregnancy outcome with other renal diseases. These include maternal hypertension, the level of renal impairment, proteinuria, elevated maternal body mass index, and specific to lupus nephritis, a longer clinical history of lupus nephritis with renal flares (73). Low-dose aspirin, 75-150 mg nocte from 12 weeks' gestation until childbirth, is recommended to reduce the risk of pre-eclampsia (74).
During the second half of pregnancy, a relapse of lupus nephritis may present with similar clinical signs as pre-eclampsia: specifically, hypertension, proteinuria, elevated serum creatinine, thrombocytopenia, and hyperuricaemia. Indeed, women with lupus nephritis are at increased risk of pre-eclampsia (73). Distinguishing features of lupus nephritis include haematuria with an active urinary sediment (red cell casts) and extrarenal manifestations affecting the skin and joints or other visceral organs. Furthermore, most pregnant women with lupus nephritis will recognize the symptoms associated with a typical lupus flare. Active lupus nephritis is associated with a rising titre of anti-dsDNA antibodies and a failure of the gestational rise in serum complement (C3 and C4) levels from the first to second half of pregnancy (72).
Women with active lupus nephritis are at an increased risk of adverse fetal outcomes, especially if associated with antiphospholipid antibodies (lupus anticoagulant, anticardiolipin IgG antibodies, and anti-beta-2 IgG antibodies) (75). Maternal hypertension and a high SLE disease activity index (SLEDAI) compounds these risks (75).
Management of lupus nephritis in pregnancy
Prednisolone, azathioprine, and hydroxychloroquine have all been safely used during pregnancy and while breastfeeding to keep lupus nephritis in remission (76). Mycophenolate mofetil is widely used outside pregnancy for the control of lupus nephritis, but it is teratogenic. Women who switch from mycophenolate mofetil to azathioprine while their lupus nephritis is quiescent and in anticipation of pregnancy, have good pregnancy outcomes and rarely develop renal flares (77). Rituximab is a monoclonal antibody that depletes B cells and has shown promise to ameliorate lupus nephritis. However, rituximab crosses the placenta to deplete B cells in the fetus and should not be used during pregnancy (76).
A flare of lupus nephritis during pregnancy can be treated with intravenous methylprednisolone 500 mg and an increase oforal prednisolone to around 40 mg daily. During pregnancy, steroid-resistant and progressive lupus nephritis has been successfully treated with tacrolimus and intravenous cyclophosphamide. However, when a severe flare of lupus nephritis occurs during pregnancy, the effects of this life-threatening condition on the mother, as well as the effects of toxic drugs on the fetus, need to be balanced against the likelihood of a successful fetal outcome. Sometimes, difficult decisions regarding continuation of the pregnancy need to be taken. Additional treatment includes antihypertensive medication to control blood pressure (to ≤140∕90 mmHg) and thromboprophylaxis with low-dose aspirin and low-molecular-weight heparin, especially in the presence of antiphospholipid antibodies and proteinuria greater than 1 g/24 hours. Lupus nephritis is slightly more likely to flare postpartum, but there is no evidence to support the use of prophylactic steroids in anticipation of a peripartum disease flare.
Autosomal dominant polycystic kidney disease
Women with autosomal dominant polycystic kidney disease (ADPKD) who have normal renal function and blood pressure, usually have a successful, uncomplicated pregnancy (78). However, pre-existing hypertension in ADPKD is a significant risk factor for pre-eclampsia and fetal prematurity (78). Children born to mothers with ADPKD will of course have a 50% risk of inheriting the gene associated with ADPKD. New treatments for slowing the progression of renal cysts and reducing the decline in renal function are emerging, but are not yet recommended in pregnancy (79).
Reflux nephropathy/vesicoureteral reflux
Reflux nephropathy or vesicoureteral reflux (VUR) is a congenital urological abnormality that usually presents in childhood with recurrent urinary tract infections. Retrograde passage of urine is associated with renal scars and is a common cause of CKD in young women. During pregnancy, women with VUR are at risk of ureteric obstruction, even if VUR has been surgically corrected. An ultrasound scan of the renal tracts before pregnancy, or in the first trimester can be a useful comparator, if symptoms of urinary outflow obstruction develop in later pregnancy. Relief of the obstruction may require nephrostomy or ureteric stenting.
Pregnant women with persistent VUR are twice as likely to develop acute pyelonephritis compared with those who have had spontaneous or surgical resolution of VUR (80). These women should therefore be screened for asymptomatic bacteriuria every 4-6 weeks throughout pregnancy. There should be a low threshold for prescribing prophylactic antibiotics to reduce the risk of recurrent UTIs and preserve renal function. Women with persistent VUR, especially those with a history of upper UTI, and who are contemplating pregnancy should consider prepregnancy correction of VUR to reduce maternal and fetal morbidity. As with other forms of CKD, women with VUR and reduced GFR, proteinuria, and hypertension have the greatest risk of adverse pregnancy outcome (80, 81). Almost 50% of neonates born to mothers with VUR will themselves have VUR and should therefore be offered screening with a micturating cystogram (81).
Diabetic nephropathy
Diabetic nephropathy is the most common cause of end-stage renal disease (ESRD) in high-resource nations (82). However, the early stages of diabetic nephropathy are asymptomatic. An initial rise in glomerular capillary pressure leads to renal hyperfiltration, elevated GFR, and microalbuminuria. Pregnancy augments the hyperfiltration of early diabetic nephropathy, which implies that diabetic and gestational hyperfiltration work through separate, but synergistic mechanisms. This explains why women with diabetic nephropathy show a gestational increase in proteinuria, which does not necessarily indicate pre-eclampsia. Women with diabetes can also be reassured that pregnancy does not trigger the onset of diabetic nephropathy and those who have established diabetic nephropathy with well-preserved renal function and normal blood pressure, do not progress more rapidly to ESRD due to pregnancy.
Diabetic nephropathy (urinary albumin:creatinine ratio >300 mg/g) affects approximately 2.5% of pregnant women with both type 1 and type 2 diabetes (83). Microalbuminuria (urinary albumin:creatinine ratio 30-299 mg/g) is also equally prevalent among pregnant women with type 1 and type 2 diabetes at approximately 4% (83). Good control of maternal blood glucose levels and hypertension before conception and during pregnancy improve both perinatal and maternal outcomes (83, 84). Conversely, poor glycaemic control and blood pressure greater than 130/80 mmHg are associated with an increased rate of pre-eclampsia and preterm childbirth (85).
Over time, diabetic nephropathy leads to a gradual reduction in GFR. Women with diabetic nephropathy and moderate to severe renal impairment (SCr >125 μmol∕L) have more than a 40% chance of an accelerated decline in renal function, usually associated with pre-eclampsia or an exacerbation of hypertension (86).
Renal replacement therapy and pregnancy
Pregnancy on dialysis
Women with ESRD have reduced fertility, which may be associated with amenorrhoea or anovulatory cycles and they are predisposed to premature menopause. Improved haemodialysis (HD) systems and intensified dialysis regimens have however increased the likelihood of women conceiving while on HD (87). Diagnosis of pregnancy can be difficult, due to irregular menses and a raised beta-human chorionic gonadotropin which is not diagnostic of pregnancy in women with ESRD. Transvaginal ultrasonography is therefore necessary if pregnancy is suspected. Pregnancy outcomes for women on HD have improved markedly over recent years with HD regimens that successfully mimic the physiological increase in GFR of healthy pregnancy. Live birth rates of up to 85% have been found in women on the most intensive HD regimens (88). A dedicated multidisciplinary renal and obstetric team is crucial for a good pregnancy outcome.
Fewer women conceive on peritoneal dialysis (PD) than on HD (89). There are, however, several case reports of successful pregnancies in women on PD. Meeting the increased GFR and physiological demands of healthy pregnancy is challenging on PD. Furthermore, women with large polycystic kidneys or polyhydramnios may be unable to accommodate peritoneal fluid in the third trimester. A switch to HD may therefore be necessary to maintain a pregnancy. When it is necessary to initiate dialysis during pregnancy HD is the preferred modality. Complications of PD include peritonitis that should be treated in the same way as non-pregnant patients with intraperitoneal antibiotics.
Women who conceive with residual renal function but then start dialysis have a better pregnancy outcome compared with women who conceive on an established dialysis regimen (90). For this reason, HD should be considered in women with a serum urea concentration greater than 20 mmol/L (87). Urea crosses the placenta to the fetus and a high fetal urinary urea concentration causes an osmotic diuresis, which is associated with polyhydramnios on less rigorous dialysis regimens. Preterm rupture of membranes and maternal hypertension are other causes for preterm delivery. Frequent dialysis will also reduce the need for large fluid shifts which may compromise uteroplacental blood flow. In those women who have some residual renal function, fluid balance is easier to manage, which increases the likelihood of a successful pregnancy outcome.
Women who increase their HD regimen to between 37 and 56 hours per week are more likely to have a successful pregnancy outcome compared with women on a lower HD intensity regimen (Figure 14.3) (88). Fluid balance and weight gain should recognize an average gestational weight gain of 0.5 kg per week during the second and third trimesters. Maternal blood pressure should be kept below 140/90 mmHg. Rises in blood pressure might initially respond to extra fluid removal, but resistant hypertension in a euvolaemic woman may herald gestational hypertension requiring antihypertensive medication. Women on HD with anuria will clearly not produce proteinuria and therefore the obstetrician will have to use other symptoms and signs of pre-eclampsia to make the diagnosis.
Increased dialysis will lead to hypokalaemia and a higher concentration of potassium in the dialysate or potassium supplements may be necessary. Furthermore, a gestational reduction in serum sodium concentration necessitates a concomitant reduction in dialysate sodium concentration to around 135 mmol/L and the gestational reduction in serum bicarbonate concentration (1822 mmol/L) should be matched with a low-bicarbonate dialysate. Increased dialysis frequency will also allow a greater protein intake, which is variably recommended to be between 1.2 and 1.8 g/ kg/day.
Anaemia and haemorrhage are common in the dialysis population. Haemoglobin and iron status need to be monitored monthly; iron supplements and erythropoietin should be given to maintain Hb between 100 and 110 g/L. The dose of erythropoietin needs to be increased by 50-100% during pregnancy. It does not cross the placenta and consequently there have been no reports of teratogenicity or polycythemia in the infant. The dialysis circuit should be heparinized as usual. Folic acid supplementation (2-5 mg/day) is recommended throughout pregnancy and low-dose aspirin (50-150 mg/ day) taken from shortly after conception may reduce the risk of preeclampsia. The requirement for calcium and vitamin D supplements is also likely to change as pregnancy progresses and plasma levels of calcium, phosphate, and vitamin D need to be monitored and doses of phosphate binders and vitamin D analogues adjusted accordingly.
If preterm labour has not eventuated, planned induction of labour at 37 weeks' gestation is recommended (87). Caesarean section is reserved for clinical indications. Breastfeeding on dialysis is possible if maternal euvolaemia is maintained and drugs toxic to the neonate are avoided.
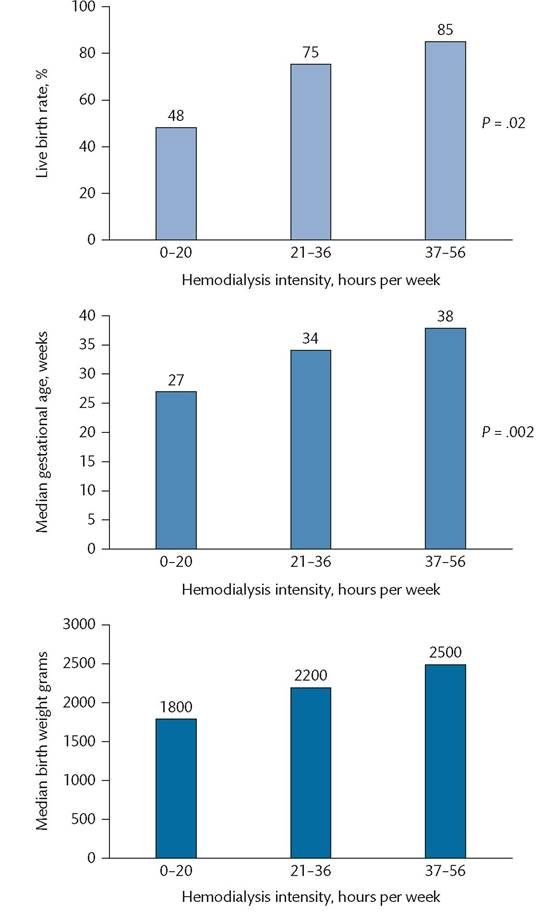
0-20, n = 46; 21-36, n = 16; 37-56, n = 13.
In written with established ESRD.
Figure 14.3 Improved pregnancy outcomes with greater haemodialysis intensity.
Reproduced from Hladunewich M, Schatell D. Intensive dialysis and pregnancy. Hemodialysis International 2016; 20: 339-348 with permission from John Wiley and Sons.
Renal transplantation and pregnancy
A successful pregnancy outcome is much more likely and much easier to manage if a woman with ESRD receives a renal transplantation. Fertility usually returns within 6 months of a transplantation, by which time renal function and immunosuppressive therapy have usually stabilized. Over 1500 pregnancies from women with renal transplants have been reported (91, 92). Among these pregnancies, approximately 75-80% result in a live birth (92). As for all CKD, pregnancy outcome depends on clinical parameters, specifically Immunosuppression for renal transplants during pregnancy
Despite physiological immune tolerance during pregnancy, continued therapeutic immunosuppression is necessary to maintain graft survival. Prednisolone is safe in pregnancy as only one-tenth of the maternal concentration is found in cord blood. Azathioprine passes easily across the placenta, but it is not converted to its active metabolite, 6-mercaptopurine, by the immature fetal liver. Azathioprine has had an excellent safety record during pregnancy.
During pregnancy, the gestational rise in plasma volume leads to a fall in plasma concentration of calcineurin inhibitors (e.g. tacrolimus and ciclosporin). If trough drug levels are to be kept within the prepregnancy therapeutic range, the dose of tacrolimus or ciclosporin needs to be increased as pregnancy progresses (93). To avoid toxic side effects during pregnancy (e.g. hypertension), the dose of calcineurin inhibitor should be adjusted to keep levels at the lower end of the therapeutic range. Postpartum, the plasma volume returns to non-pregnancy levels within a few days and calcineurin inhibitor doses should be promptly reduced to prepregnancy levels.
Women taking mycophenolate mofetil should be switched to azathioprine. Women taking sirolimus should be switched to tacrolimus, despite several reports of good pregnancy outcomes with sirolimus. In anticipation of pregnancy, it is prudent to switch from drugs with an unknown or harmful safety profile to those known to be safe.
High-dose steroids remain a first-line therapy for an acute rejection episode during pregnancy. In steroid-resistant rejection, difficult decisions may need to be taken about escalating the immunosuppression to prevent graft rejection and unknown harm to the fetus. There are many case reports of good pregnancy outcomes using multiple immunosuppressant therapies (94).
Pregnant women on immunosuppression should receive prophylactic antibiotics for all surgical interventions, including childbirth. Furthermore, immunosuppressed women should be screened regularly for asymptomatic bacteriuria, and treated when pathogenic bacteria is isolated. Just one UTI during pregnancy in a transplant patient is an indication for low-dose antibiotic prophylaxis for the duration of the pregnancy.
The pelvic transplant kidney does not obstruct childbirth. A spontaneous vaginal delivery should therefore be the aim if obstetric circumstances allow. Caesarean section is, however, often necessary. The dose of corticosteroids should be temporarily increased in the perioperative period.
Postpartum care
Breastfeeding should be encouraged in women with renal transplants and a thriving infant. Small amounts of ciclosporin and tacrolimus are detectable in breast milk, but none is evident in the breastfed infant. Azathioprine is not detectable in breast milk. In general, mothers taking immunosuppressive drugs and who are keen to breastfeed should continue to do so as long as the neonate is thriving.