Physiological changes to thekidney during healthy pregnancy
Renal glomerular function during pregnancy
Renal adaptation to pregnancy is anticipated during the luteal phase of each menstrual cycle. Renal blood flow and glomerular filtration rate (GFR) increase by 10-20% before menstruation (1).
If pregnancy is established, the corpus luteum persists and these haemodynamic changes continue (2). By 16 weeks' gestation, GFR is 55% above non-pregnant levels (2). This increment is mediated through an increase in renal blood flow that reaches a maximum of 70-80% above non-pregnant levels by the second trimester and then falls to around 45% above non-pregnant levels at term (3).The changes to renal physiology in healthy pregnancy can both hide and mimic renal disease. The gestational increase in GFR leads to a fall in serum creatinine (SCr) concentration, so that values considered normal in the non-pregnant state may be abnormal during pregnancy (Table 14.1). Serum creatinine is not, however, linearly correlated with creatinine clearance and is influenced by muscle mass, physical exercise, racial differences, and diet.
The gestational rise in renal blood flow also causes the kidneys to swell so that bipolar renal length increases by approximately 1 cm (Figure 14.1). During the third trimester renal blood flow falls, leading to a decrease in creatinine clearance and an increase in serum creatinine (1). Serum urea levels, however, continue to fall in the third trimester due to reduced maternal hepatic urea synthesis.
The renal pelvis and ureters dilate and appear obstructed to those unaware of these changes. The right renal pelvis dilates by up to 0.5 mm each week from 6 to 32 weeks, reaching a maximum diameter of 2 cm (90th centile) until term (4). The left renal pelvis reaches a maximum diameter of 8 mm (90th centile) at 20 weeks' gestation (4).
Other physiological changes simulate the classic features of nephrotic syndrome.
For example, in healthy pregnancy, proteinuria increases as pregnancy progresses. However, a random urinary protein (mg):creatinine (mmol) ratio (PCR) should not normally exceed 0.20 mg/mmol (95th centile), while a PCR greater than 0.27 mg/mmol is a good predictor of significant proteinuria (5). In healthy pregnancy, the serum albumin level falls by 5-10 g/L, serum cholesterol and triglyceride concentrations increase markedly (Table 14.1), and towards term, dependent oedema affects most pregnancies.Renal tubular function during healthy pregnancy
Increased alveolar ventilation causes respiratory alkalosis to which the kidney responds by increased bicarbonaturia and a compensatory metabolic acidosis. The result is that maternal pH remains stable at 7.4. Reduced tubular glucose reabsorption leads to glycosuria in approximately 10% of pregnant women, even when maternal blood glucose levels are normal. During the first trimester urinary urate excretion increases, but then decreases towards term so that plasma urate rises again to non-pregnancy levels.
A healthy pregnant mother gains a total of 6- 8 kg of fluid, of which approximately 1.2 L is intravascular plasma. Plasma osmolality falls by 10 mOsmol/kg by 5-8 weeks' gestation due to a decrease in both the threshold for thirst and for the release of antidiuretic hormone (vasopressin) (6). During pregnancy, vasopressin is degraded by placental vasopressinase, such that the maternal posterior pituitary produces four times as much vasopressin to maintain physiological concentrations at term. Failure of the maternal pituitary to keep up with the increased metabolic clearance of vasopressin leads to a transient polyuric state in the third trimester, which is known as transient diabetes insipidus of pregnancy (7). This condition can be controlled with desmopressin and cured by childbirth.
Renal endocrine function during pregnancy
The kidney also acts as an end1ocrine organ, producing three hormones, namely erythropoietin, active vitamin D, and renin.
The production of all three hormones increases during healthy pregnancy but their effects are masked by other changes. In early pregnancy, peripheral vasodilatation exceeds renin-aldosterone-mediated plasma volume expansion, so diastolic blood pressure decreases by 12 weeks. Conversely, plasma volume expansion exceeds the erythropoietin- mediated increase in red cell mass, causing a ‘physiological anaemia', which should not normally lead to a haemoglobin concentration of less than 95 g/L (8). Similarly, extra active-vitamin D produced by the placenta circulates at twice non-gravid levels, but concomitant halving of parathyroid hormone levels, hypercalciuria, and increased fetal requirements keep plasma ionized calcium levels unchanged (9).Table 14.1 Physiological changes to common indices of renal function during healthy pregnancy (mean ± SD)
| Non-pregnant | I First trimester | Second trimester | Third trimester | |
| Effective renal plasma flow (mL/min) | 480 ± 72 | 841 ±144 | 891 ±279 | 771 ± 175 |
| GFR (mL/min) inulin clearance | 105 ± 24 | 162 ± 19 | 174 ± 24 | 165 ± 22 |
| GFR (mL/min) 24-hour creatinine clearance | 98 ± 8 | 151 ± 11 | 154 ± 15 | 129 ± 10 |
| Serum creatinine (mmol/L) | 73 ± 10 | 60 ± 8 | 54 ± 10 | 64 ± 9 |
| Plasma urea (mmol/L) | 4.3 ± 0.8 | 3.5 ± 0.7 | 3.3 ± 0.8 | 3.1 ± 0.7 |
| Plasma urate (mmol/L) | 246 ± 59 | 189 ± 48 | 214 ± 71 | 269 ± 56 |
| Plasma osmolality (mOsmol/kg) | 290 ± 2.2 | 280 ± 3.4 | 279 ± 2.9 | 279 ±5.0 |
| Fast. cholesterol (mmol/L) | 5.0 ± 0.3 | 5.5 ± 0.4 | 6.9 ± 0.4 | 7.8 ± 0.4 |
Acute kidney injury in pregnancy
Acute kidney injury (AKI) has replaced the term acute renal failure, as kidneys can be injured before function fails.
'The common causes of AKI are outlined in Box 14.1. AKI is rare in early pregnancy. When it does occur, it is usually associated with septic abortion, a complication largely confined to low-resource nations or those without legalized abortion services. Rarely, severe hyperemesis gravidarum can cause dehydration and prerenal AKI. AKI at the time of childbirth is most commonly caused by gestational syndromes such as pre-eclampsia and abruption placentae (Box 14.1).Pregnancy is a prothrombotic state, associated with changes to the vascular endothelium and clotting factors that predispose pregnant women to acute glomerular capillary thrombosis. Whereas non-pregnant patients who suffer an acute prerenal insult (e.g. haemorrhage, dehydration, or septic shock) may develop AKI if inadequately treated, the same prerenal insult in pregnancy is more likely to develop into renal cortical necrosis with permanent renal impairment.
The principles of AKI management are aimed at identification and correction of the precipitating cause (summarized in Table 14.2). While definitive management to treat the cause of AKI is carried out, the patient should be supported with optimal fluid resuscitation guided by fluid balance monitoring. If oliguria persists despite euvolaemia, with deteriorating renal function or fluid overload, then fluid restriction followed by renal replacement therapy should be considered. The indications for acute renal replacement therapy (dialysis) in pregnancy include hyperkalaemia (potassium >7.0 mmol/L) refractory to medical treatment, pulmonary oedema refractory to diuretics, acidosis producing circulatory problems, and uraemia. There is no absolute level of uraemia above which dialysis is mandatory for new-onset AKI, but a serum urea over 25-30 mmol/ L or SCr greater than 500-700 mmol/L (5.65-7.91 mg/dL), usually indicates a need for dialysis.
Pre-eclampsia and the kidney
Women with pre-existing renal disease are more vulnerable to preeclampsia, especially with associated chronic hypertension (10, 11).
Pregnant women with moderate to severe renal disease (chronic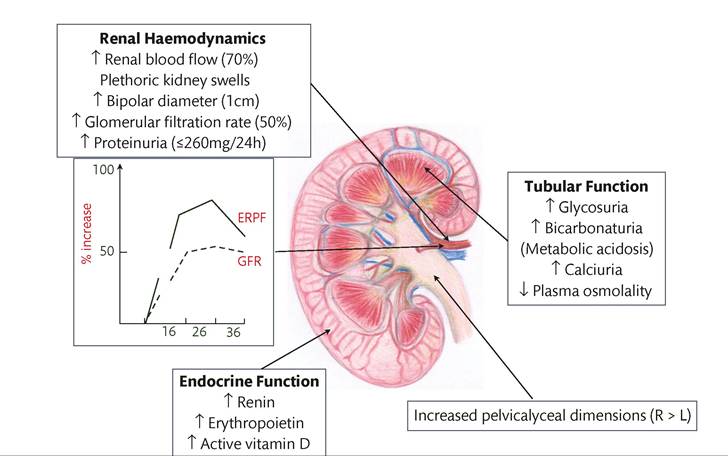
Figure 14.1 Changes to renal physiology during healthy pregnancy. ERPF, effective renal plasma flow; GFR, glomerular filtration rate. Reproduced from Williams D and Davison JM. Chronic Kidney Disease in Pregnancy. BMJ 2008; 336: 211-215 with permission from BMJ Publishing Group Ltd.
Box 14.1 Causes of acute kidney injury in pregnancy
Prerenal
• Volume depletion: hyperemesis gravidarum, peripartum haemorrhage, diabetes insipidus
• Oedematous states: nephrotic syndrome, peripartum cardiomyopathy
• Hypotension: sepsis, peripartum cardiomyopathy, amniotic fluid embolus
• Renal hypoperfusion: drugs (e.g. NSAIDS)
• Renovascular disease: renal artery stenosis, more commonly congenital in young women
Intrinsic renal disease
• Pre-eclampsia: glomerular endotheliosis
• Microangiopathic haemolytic anaemia (MAHA) (e.g. HUS, TTP)
• Acute fatty liver of pregnancy (AFLP)
• Acute-on-chronic kidney disease (e.g. flare of lupus nephritis)
• Vasculitis (e.g. granulomatosis with polyangiitis, formerly Wegener's granulomatosis)
Post-renal disease; obstructive
• Acute obstruction of renal tracts (e.g. calculi, papillary necrosis)
• Congenital urological anomalies (e.g. pelviureteric junction or vesico- ureteric junction obstruction, even if previously ‘surgically corrected')
kidney disease (CKD) stages 2-5) should be offered low-dose aspirin (50-150 mg/each evening from 12 weeks' gestation) to reduce their risk of pre-eclampsia and perinatal death (12).
Suspected proteinuria on urinary dipstick testing (≥1+ proteinuria) should be assessed with a spot urinary PCR, rather than a 24hour urine collection (13, 14). New-onset proteinuria (PCR >30 mg/ mmol) in conjunction with new-onset hypertension is sufficient to make a diagnosis of pre-eclampsia (14). However, the level of proteinuria is a poor predictor of maternal and neonatal complications and taken in isolation should not be used as an indication for premature delivery.
Pregnant women who develop proteinuria (PCR >100-300 mg/mmol; the threshold depends upon other maternal risk factors for thrombosis) should be offered thromboprophylaxis with low-molecular-weight heparin until at least 4 weeks postpartum and fully mobile.Pre-eclampsia itself is often associated with mild AKI (SCr up to 125 μmol∕L; 1.41 mg/dL) and complete postpartum recovery of renal function is usual. Only if pre-eclampsia is associated with another renal insult such as peripartum haemorrhage, will AKI be severe enough to require transient renal replacement therapy.
Postpartum, only 2-5% of women who had pre-eclampsia are found to have underlying renal disease (15). Women who have had pre-eclampsia should nevertheless be checked for persistent postpartum hypertension and proteinuria. Gestational hypertension usually resolves within 3 months of delivery, but severe preeclampsia-induced hypertension and heavy proteinuria can take up to 24 months to disappear (16). Persistent microalbuminuria is suggestive of underlying renal disease and may also herald a predisposition to future cardiovascular disease (17).
The diagnosis of pre-eclampsia is difficult if there is chronic hypertension and pre-existing proteinuria, especially as these two parameters become more marked in late pregnancy. Furthermore, hyperuricaemia and fetal growth restriction are common features of both pre-eclampsia and chronic renal impairment, but new-onset hepatic transaminitis and thrombocytopenia support a diagnosis of pre-eclampsia (18).
Pre-eclampsia and AKI: clinical management of renal impairment and fluid balance
The cure for pre-eclampsia is delivery of the fetus, but the maternal condition can transiently deteriorate postpartum (19). A rise in maternal SCr concentration from around 70 μmol∕L (0.79 mg/dL) to greater than 120 μmolTh (1.36 mg/dL) would be an indication for delivery to prevent irreparable renal impairment. Dialysis is very rarely necessary, but is most common in women who double their SCr in the first 24-48 hours after birth (20).
Fluid balance is critical to the successful management of AKI during pregnancy. Too little intravascular fluid provokes prerenal failure, especially damaging to chronically impaired kidneys, while too much fluid risks pulmonary oedema, adult respiratory distress syndrome, and maternal death. Furthermore, transient oliguria (90 μmol∕L; 1.0 mg/dL) should have their fluid balance guided by clinicians on a high dependency unit. The rate of fluid replacement should take account of an assessment of current volume status, assessed by jugular venous pressure, lung fields, oxygen saturations, skin turgor, hourly urine output, and estimated insensible loses. Once euvolaemic, the rate of intravenous fluid replacement should equal the previous hour's urine output plus insensible losses—usually 30-50 mL/hour if apyrexial and not bleeding. The amount of intravenous fluid replacement can be reduced once the mother can take oral fluid and her renal impairment starts to improve. Intravenous fluid regimens that stick to a fixed hourly replacement can lead to fluid overload in oliguric woman and to reduced intravascular volume in those having a diuresis. Fluid replacement should include blood to replace blood losses, then isotonic sodium chloride or compound sodium lactate (Hartmann's solution). Dextrose solutions are hypotonic and lead to maternal hyponatraemia (5% dextrose contains only 30 mmol/ L NaCl, compared with 150 mmol/L NaCl in 0.9% sodium chloride solution). Low-dose ‘renal' dopamine infusions should not be used.
If AKI progresses with oliguria and a rising SCr, despite adequate intravascular volume and blood pressure, then fluid intake should be restricted to avoid fluid overload. Under these circumstances, renal replacement therapy will eventually be necessary. This is a rare eventuality affecting less than 1:10,000 pregnancies. Women who have had a pregnancy affected by AKI are at increased risk of adverse outcome in a future pregnancy, even if they make a full recovery from the initial insult (21).
Thrombotic microangiopathies and pregnancy
Thrombotic microangiopathies (TMAs) are rare, life-threatening causes of AKI during pregnancy. They are characterized by platelet consumption within microvascular thrombi leading to thrombocytopenia, haemolysis, and multiorgan failure (22). TMAs can be triggered by several disease processes, but the final common pathway results in activated, proinflammatory, procoagulant endothelial cells (23). A careful medical history, elucidation of organ involvement, and correct interpretation of blood tests will identify the type of TMA, which is essential for successful management.
During pregnancy, the HELLP (haemolysis, elevated liver enzymes, low platelets) syndrome is the most frequently observed TMA. HELLP syndrome has overlapping features with preeclampsia, thrombotic thrombocytopenic purpura (TTP), and antiphospholipid syndrome. HELLP syndrome usually presents with acute hepatic pain and marked elevation of liver transaminases, suggestive of liver infarction (24). Although delivery is the cure for HELLP syndrome, the postpartum clinical condition can progress for several days before improvement. Hypertension, proteinuria, abnormal clotting, and fetal growth restriction are more evident in women with HELLP syndrome compared with other forms of TMA. In the absence of postpartum resolution, rarer forms of TMA should be considered, namely TTP, which most commonly affects the nervous system and haemolytic uraemic syndrome (HUS), which most commonly causes AKI. Pregnancy predisposes to both TTP and HUS.
Haemolytic uraemic syndrome
HUS is characterized by severe AKI with thrombocytopenia and haemolysis and usually presents in late pregnancy or peripartum. Women with HUS typically have a much higher serum creatinine (creatinine>150 pmol/L) than is seen in pre-eclampsia/HELLP syndrome with marked thrombocytopenia (frequently given peripartum. NSAIDs reduce renal blood flow and in combination with hypotension and hypertension can lead to AKI (31). Women with reduced intravascular volume, especially with preexisting renal impairment, are particularly vulnerable and should not be prescribed NSAIDs. Aminoglycosides are also nephrotoxic and should be prescribed with care and attention to drug plasma levels in women with CKD.
Acute renal tract obstruction in pregnancy
Obstruction of the renal tracts during pregnancy may be due to renal calculi, congenital renal tract abnormalities, or gestational overdistension syndrome.
Nephrolithiasis
Gestational dilatation of the renal tracts, urinary stasis, and hypercalciuria all create an ideal environment for renal stone formation. However, renal colic is no more common during pregnancy than the non-gravid state, due to increased excretion of renal stone inhibitors. These include magnesium, citrate, nephrocalcin, and uromodulin. Renal colic affects approximately 1:200 to 1:1000 pregnancies, usually in the second and third trimester, and creates challenging management issues (32).
The passage of a renal calculus down the ureter causes intense intermittent pain. Renal colic is often associated with fever, urinary tract infection (UTI), and haematuria. Renal ultrasound will identify a renal calculus in about half of these women. In those with a normal ultrasound, but suggestive symptoms, magnetic resonance urography will avoid radiation, or if magnetic resonance urography is contraindicated, low-dose computed tomography can be used with minimal radiation exposure to the fetus (33).
Uncomplicated cases are those with a unilateral stone less than 1 cm in diameter, no sign of infection, good pain control, and normal maternal renal function. Under these circumstances, conservative management will result in up to 75% of pregnant women passing their stone spontaneously (32). Conservative management includes generous hydration, antibiotics, and pain relief with opiates, or prior to the third trimester, NSAIDs.
Failure of conservative management, or pregnant women with an obstructed single kidney or bilateral ureteric obstruction, or signs of infection, or a large stone larger than 1 cm require surgical intervention. If infection is suspected, drainage with an ultrasound- guided percutaneous nephrostomy or ureteric stent may be considered. However, both a nephrostomy and stent usually need to remain in place for the rest of pregnancy, require regular changes to avoid infection or encrustation, and only delay the need for definitive treatment. Ureteroscopy is now regularly used to insert a double J stent or accurately deliver local stone crushing lithotripsy. These techniques have been successfully and safely used in all stages of pregnancy (34).
Women who are recurrent stone formers with persistent hypercalciuria despite increased fluid intake can use thiazide diuretics in pregnancy to increase distal tubular reabsorption of calcium. Uric acid and cystine stones rarely form in pregnancy due to gestational bicarbonaturia, which naturally alkalinizes the urine. If problematic, both conditions may be controlled by increasing urine output and further alkalinization of the urine to a pH higher than 6. During pregnancy, D-penicillamine may be necessary for severe cases of stone-forming cystinurics and xanthine oxidase inhibitors for uric acid stones (35). However, data on these two drugs in pregnancy are limited and there are concerns about allopurinol causing major malformations when used in the first trimester (36).
Congenital ureteric obstruction
Women with congenital obstructive uropathies at the renal pelvis or vesicoureteric junction are at increased risk of acute urinary outflow obstruction in the second half of pregnancy, even if the original obstruction had been surgically corrected. Ultrasonography of the renal pelvis at the end of the first trimester provides a useful baseline with which to compare future imaging. A repeat renal ultrasound scan is indicated if there is pain suggestive of obstruction, persistent or recurrent infections, or a rise in serum creatinine. Gestational urinary outflow obstruction may require a temporary nephrostomy or ureteric stent (Figure 14.2).
Women with a single kidney and ureteric abnormalities are particularly vulnerable to develop outflow tract obstruction and AKI during pregnancy. An incomplete obstruction can cause renal impairment with an apparently good urine output. High back-pressure compresses and damages the renal medulla, leading to a loss of renal concentrating ability and production of dilute urine that is passed through an incomplete obstruction. Women born with a single

Figure 14.2 A postpartum nephrostogram of an obstructed pelviureteric junction showing a dilated collecting system in a solitary cross-fused left kidney. A 28-year-old primigravida presented with loin pain at 22 weeks' gestation. She had severe hypertension (180/ 110 mmHg) and a SCr concentration that rose rapidly to 298 pmol/L, despite a urine output of 4 L/24 hours. Pelvicalyceal dilatation (36 mm diameter) was noted and within days of a nephrostomy, her symptoms, hypertension, and SCr had all returned to normal. The pregnancy continued to 37 weeks and the nephrostomy remained in situ until 6 weeks postpartum, at which time it was replaced by a ureteral stent. The nephrostomy tube and ureteral stent can be seen on the nephrostogram.
kidney may also have other Mullerian duct anomalies that impact on pregnancy outcome, most notably a unicornuate uterus (37).
Gestational renal overdistension syndrome
During pregnancy, the renal tracts rarely become grossly overdistended. Women with renal tract overdistension present with severe loin pain, most commonly on the right side and radiating to the lower abdomen. The pain is positional, inconstant, and characteristically relieved by lying on the opposite side and tucking the knees up to the chest. Urinalysis will reveal haematuria. A renal ultrasound scan will detect a hydronephrotic kidney and grossly dilated pelvicalyceal system. Occasionally, a urinoma will be evident around the kidney indicating rupture of the renal pelvis.
Women with severe unremitting pain, haematuria, and grossly distended renal tracts on ultrasonography usually have immediate pain relief following decompression of the system with either a ureteric stent or nephrostomy. Gestational overdistension can rarely unmask a previously asymptomatic weakness in a diseased kidney, leading to kidney rupture (38). Under these circumstances, immediate surgery and almost invariably an emergency nephrectomy is needed (38).
Urinary tract infection
Urinary frequency, nocturia, urge incontinence, and strangury are common symptoms of both healthy pregnancy and UTI. If these symptoms coexist with dysuria or offensive-smelling urine, a UTI should be suspected. Microscopy and culture of a freshly voided mid-stream urine (MSU) sample will allow quantification of pyuria (white blood cells in the urine) and growth of a urinary pathogen. Bacterial UTI is the most common cause of pyuria and is considered significant if microscopy of an un-spun MSU reveals more than ten white blood cells/μL. Urine culture is conventionally recognized as significant if there is growth of greater than 105 colony-forming units (CFU)∕mL of a single recognized uropathogen, in association with pyuria. Low counts of bacteriuria (102-104 CFU/mL) may still be significant if symptomatic women have a high fluid intake or are infected with a slow-growing organism. If left untreated, most symptomatic women with ‘low-count bacteriuria' will develop 105 CFU/ mL within days. Haematuria and proteinuria are unreliable indicators of an UTI, but are important signs of renal disease.
The most common uropathogens are Gram-negative bacteria: Escherichia coli, Proteus mirabilis, Enterobacter species, and Klebsiella pneumoniae. Pregnant women who are symptomatic of a UTI, which is dipstick positive for nitrite (produced by most uropathogens) and leucocyte esterase (produced by white blood cells) should start empirical antibiotic treatment. As E. coli and enterococci are responsible for about 75% of uncomplicated UTIs, empirical treatment with nitrofurantoin 100 mg twice daily for 3 days is a good first-line choice. After 48 hours, the results of urine culture will allow a definitive choice of antibiotic. Women with glucose-6- phosphate dehydrogenase (G6PD) deficiency should avoid nitrofurantoin. Some authorities recommend that nitrofurantoin is avoided in the third trimester due to theoretical concerns it will cause neonatal haemolysis. Despite hundreds of thousands of prescriptions, there are no well-documented cases of nitrofurantoin-induced neonatal haemolysis (39). It is the author's practice to prescribe nitrofurantoin in the third trimester to women at high risk of pyelonephritis and at low risk of G6PD deficiency.
Trimethoprim 200 mg twice daily for 3 days is more likely to be active against E. coli and Enterococcus than ampicillin or cephalosporins and can be used as a second-line choice for empirical treatment of a suspected UTI. Trimethoprim should be avoided in the first trimester as it is a folic acid antagonist associated with an increased risk of neural tube defect (40). Bacterial multidrug resistance is induced by empirical antibiotic treatment. However, until new technologies accelerate our choice of antibiotic through point of care testing, an empirical choice of antibiotic remains necessary (41).
Asymptomatic bacteriuria
Asymptomatic bacteriuria, growth of a uropathogen in the absence of symptoms, occurs in 2-10% of pregnant women. Onsite tests, including dipstick testing for nitrites and the dipslide with Gram staining, have good specificity to rule out asymptomatic bacteriuria, but lack sensitivity and therefore miss many cases of asymptomatic bacteriuria (42). Currently, culture of a MSU sample remains a useful screen for asymptomatic bacteriuria.
Pregnancy-induced structural and immune changes to the urothelium make it more likely that a lower UTI will ascend to cause acute pyelonephritis (43, 44). Women with underlying renal disease are particularly at risk of UTI and pyelonephritis and should be screened for asymptomatic bacteriuria every 6 weeks (Box 14.2). Healthy women with a singleton pregnancy and asymptomatic bac- teriuria also have an increased relative risk of pyelonephritis, but the absolute risk is much lower (2.4%) than previously estimated (30%) (43, 44). A previous Cochrane review concluded that antibiotic treatment of asymptomatic bacteriuria reduced the incidence
Box 14.2 Pregnant women at risk of asymptomatic bacteriuria and ascending urinary tract infection and for whom screening with MSU every 4-6 weeks is recommended
• Past history of asymptomatic bacteriuria
• Previous recurrent UTIs
• Pre-existing renal disease, especially scarred kidneys due to reflux nephropathy
• Structural and neuropathic abnormalities of the renal tracts
• History of renal calculi
• Pre-existing diabetes mellitus but not gestational diabetes
• Sickle cell disease and trait
• Low socioeconomic group and less than 12 years of higher education
of pyelonephritis compared to placebo or no treatment (odds ratio 0.24; 95% confidence interval 0.19-0.32) (45). For this reason, antibiotics have been readily prescribed for asymptomatic bacteriuria. However, there are concerns that widespread antibiotic use may lead to bacterial multidrug resistance, and also of a possible increased risk of cerebral palsy in children exposed to antibiotics in utero. Hence it seems prudent to reserve the treatment of asymptomatic bacteriuria to women at high risk of renal complications (Box 14.2). Asymptomatic bacteriuria has also been thought to be associated with an increased risk of preterm delivery and low birth weight (46), but a contemporary multicentre study has shown no such association between asymptomatic bacteriuria in mid-trimester and preterm birth or growth restriction (44).
Screening for recurrent infections should begin 1 week after completion of initial treatment and then 6-weekly for the rest of pregnancy. Recurrent infections or a first infection in a pregnant woman at high risk of pyelonephritis (Box 14.2) should be treated with an antibiotic that reflects antibacterial sensitivities for 7-10 days. Women with renal disease who have had two episodes of asymptomatic bacteriuria or cystitis should be considered for low-dose antibiotic prophylaxis—guided by the sensitivities of the most recent infective organism. Antibiotic prophylaxis will reduce the risk of pyelonephritis for the remainder of pregnancy and until 4-6 weeks postpartum (47). Suitable regimens for long-term antibiotic prophylaxis include nitrofurantoin 50-100 mg every night (nocte), trimethoprim 100-150 mg nocte, amoxicillin 250 mg nocte, or cephalexin 125-250 mg nocte (47). These women should have a renal ultrasound scan to check for structural abnormalities or renal calculi.
Acute pyelonephritis
The same uropathogens that cause asymptomatic and symptomatic infections are responsible for acute pyelonephritis. Therefore, the prevalence of asymptomatic bacteriuria in a pregnant population dictates the incidence of acute pyelonephritis. In the United States, acute pyelonephritis affects approximately 1:200 pregnancies (48). Unless acute pyelonephritis is treated promptly there is an increased risk of AKI, respiratory distress, anaemia, sepsis, and preterm birth (48).
Most women with acute pyelonephritis present with back ache, fever, rigors, and costovertebral angle tenderness, while about half have lower urinary tract symptoms, nausea, and vomiting. Bacteraemia is present in approximately 20% of pregnant women with acute pyelonephritis and a small proportion of these women will develop septic shock, and increased capillary leak leading to pulmonary oedema (48). It is important however to differentiate the hypotension due to reduced intravascular volume (fever, nausea, and vomiting) from that due to septic shock. Women with pyelonephritis who are at risk of serious complications are those who present with the highest fever, tachycardia, at greater than 20 weeks' gestation, and who have received tocolytic agents and injudicious fluid replacement. Acute pyelonephritis can trigger uterine contractions and preterm labour (49). Antibiotic treatment of pyelonephritis will reduce uterine activity, but those with recurrent infection are at increased risk of preterm labour.
Management of acute pyelonephritis
Women suspected of acute pyelonephritis should be admitted to hospital for at least 24 hours. Laboratory tests should include full blood count, SCr, electrolytes, C-reactive protein, urine, and blood culture. Renal tract ultrasound scanning is recommended to identify any underlying structural abnormality or calculi. Pregnant women with pyelonephritis and septic shock need intensive care. Assessment of hydration will optimize fluid balance, aiming for a urine output greater than 30 mL/hour to minimize renal impairment and reduce the risk of pulmonary oedema. Intravenous antibiotics should be started empirically until sensitivities of blood and urine cultures are known.
Gram-negative bacteria causing pyelonephritis in pregnancy are usually sensitive to intravenous cefuroxime 750 mg-1.5 g every 8 hours, or ceftriaxone 1 g depending on the severity of the maternal condition and until sensitivities are known (48). Women allergic to beta-lactam antibiotics can be given intravenous gentamicin (1.5 mg/kg every 8 hours) for the initial treatment of acute pyelonephritis. A single-dose regimen (7 mg/kg every 24 hours) should be avoided during pregnancy to reduce the small risk of eighth nerve damage to the fetus (50). Serum concentrations of gentamicin should be measured and dose adjustments made according to levels. Intravenous antibiotics should be continued until the patient has been afebrile for 24 hours. Oral antibiotics should then be given for 7-10 days, according to bacterial sensitivities, or if not available, as for symptomatic lower UTI (50).
Following one episode of pyelonephritis, pregnant women should have monthly urine cultures to screen for a recurrence (51). The risk of recurrent pyelonephritis can be reduced with antimicrobial prophylaxis, according to the sensitivities of the initial bacterial infection until 4-6 weeks postpartum (51).