Classification and types of childbirth trauma
Perineal trauma may occur spontaneously or surgically, in the form of an episiotomy (4). The current classification of perineal trauma according to the Royal College of Obstetricians and Gynaecologists is as follows (3) (Figure 59.1):
• First degree: laceration of the vaginal epithelium or perineal skin only (Figure 59.2).
• Second degree: involvement of the perineal muscles but not the anal sphincter (Figure 59.3).
• Third degree: disruption of the anal sphincter muscles (Figure 59.4). This is further subdivided into:
■ 3a: less than 50% thickness of external anal sphincter torn
■ 3b: greater than 50% thickness of external anal sphincter torn
■ 3c: external and internal sphincters torn.
• Fourth degree: a third-degree tear with additional disruption of the anal epithelium (Figure 59.5).
• Buttonhole tears are isolated tears of the anal mucosa and the vaginal epithelium without involvement of the anal sphincters.
OASIS encompasses both third- and fourth-degree tears.
Levator ani muscle injuries
The levator ani muscle (LAM) plays a major role in the biomechanical properties of the birth canal and pelvic floor. During labour and delivery, the LAM stretches beyond its limits (5, 6). In passive muscles, a stretch of 50% may cause significant injury, whereas in maximally activated muscles, a stretch of 30% results in injury (7).
The reported incidence of LAM trauma varies widely and has been reported to range between 13% and 26% in women who have a vaginal delivery (8-11). A magnetic resonance imaging (MRI)-based study of the LAM found no defects in nulliparous women (12). In contrast, defects were found in 20% of women after their first vaginal birth. An even greater number of women sustain irreversible distension of the levator hiatus. Acute LAM injuries can be diagnosed clinically by digital examination.
MRI, transperineal ultrasound, and transvaginal ultrasound can also be used for diagnosis (13). Levator avulsion can be part of a large vaginal tear and is associated with a twofold risk of significant anterior and apical compartment prolapse, with less effect on posterior compartment prolapse (11).There are various definitions of LAM injury, according to mode of assessment and imaging modality. According to DeLancey et al., a proposed LAM injury MRI-based classification is as follows:
The left and right muscles are scored separately. A score of 0 is assigned if there is no damage visible on MRI, 1 if less than half of the muscle is missing, 2 if more than half, and 3 if the complete muscle bulk is lost. The total score is sum of both sides, ranging from 0 to 6 and is categorized as follows: 0, normal or no defect; 1-3, minor defect; 4-6 major defect. (14)
Nerve injuries
Pudendal nerve injury can be associated with pelvic floor dysfunction. Nerve compression and stretching during labour and delivery can lead to incontinence. This is reversible in most cases, although in severe cases incontinence may persist (11, 12). The mechanism of denervation injury is similar to nerve injury in patients with
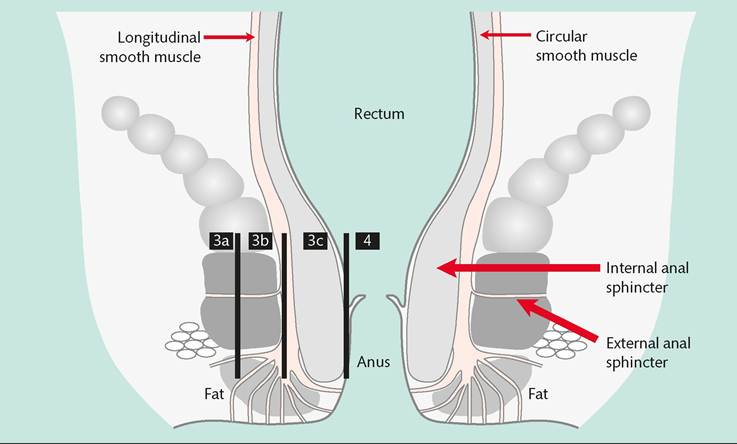
Figure 59.1 Classification of anal sphincter injury.
Reproduced from Cardozo and Staskin (Eds) Textbook of Female Urology and Urogynecology 2nd Ed. 2006 Informa Healthcare p1112 with permission from Informa.
chronic constipation (15). It has been associated with the duration of the second stage of labour, size of the baby, and instrumental delivery (16). A study looking at 96 nulliparous women before and after delivery found that vaginal delivery caused partial denervation of the pelvic floor in most women with 80% showing subsequent reinnervation (17).
Connective tissue injuries
During pregnancy, collagen and elastin, components of connective tissue, undergo modifications in order to increase vaginal distensi- bility and capacity.
During labour and delivery, extensive stretching may result in collagen damage. The endopelvic fascia and other connective tissue structures may undergo overstretching, tearing, and detachment from their bony attachments. After delivery, remodelling of the connective tissue takes place, but the new tissue is not as strong as the original (18).Injuries at the level of the uterine ligaments may result in uterine prolapse. Increases in intra-abdominal pressure generated by pregnancy itself can cause trauma to these structures, especially in a twin pregnancy, macrosomia, or polyhydramnios. At the level of vaginal apex and posterior compartment, trauma resulting in defects of the pericervical ring and rectovaginal fascia may present as enterocele or high rectocele. The rectovaginal fascia may get overdistended, ruptured, or become detached from the arcus tendineus (19).
Injuries to the pubocervical fascia may result in cystocele or rarely anterior enterocele (8, 19). Loss of support of the vaginal fornices may result in paravaginal defects (20). Injuries to the pubourethral ligaments and pubocervical fascia can be associated with urethrocele, hypermobility of the urethra and bladder neck, and stress urinary incontinence. Direct injury to the urethral sphincter may also cause stress urinary incontinence (8, 19). Trauma to the lower posterior compartment and perineum can result in low rectoceles and perineal tears.
Prolapse is more common in parous compared to nulliparous women (21). Vaginal childbirth, particularly operative vaginal delivery, increases the risk of pelvic organ prolapse (POP) (22, 23). At

Figure 59.2 First-degree tear.

Figure 59.3 Second-degree tear.

Figure 59.4 Third-degree tear.
6 months postpartum, stage 2 POP was noted in 18% of primiparous Spanish women delivered vaginally compared to 7% of women who delivered by caesarean (24). Similar findings were shown in a multicentre study from the United States (25). No difference in prolapse rates was seen in women delivered by elective caesarean section, compared to those delivered by caesarean after active labour and full cervical dilatation (22). A study of vaginally parous women found that those who had more than one spontaneous laceration were more likely to have prolapse 5-10 years after delivery (23). No increase in POP was found in association with episiotomy.
Pubic bone injuries
Injuries to the pubic bones and symphysis pubis can be evaluated by MRI. An observational study of women who underwent MRI after delivery showed pubic bone fractures in 38% of women at high risk for pelvic floor injury (second stage of labour >150 minutes or <30 minutes, anal sphincter injury, use of forceps, maternal age >35 years, and birth weight >4000 g) and in 13% of women at low risk for pelvic floor injury. Bone marrow oedema in the pubic bones was present in 61% of women (26). Separation of the pubic symphysis at childbirth is uncommon. A review showed an incidence of pubic symphysis diastasis to be 1 in 500 (27).
These injuries can be associated with significant and prolonged pain and disability. Although conservative treatment is sufficient in most cases, invasive orthopaedic treatments are sometimes required.

Figure 59.5 Fourth-degree tear.