Clinical evaluation of pelvic organ prolapse
POP is a clinical diagnosis classified by symptoms and the degree of anatomical deformity (descent), depending on the site of the defect and the pelvic organs that are involved.
There have been difficulties in designing an objective, reproducible system of grading prolapse.
Intra- and interobserver variation on each successive examination can be significantly high leading to confusion. This makes it difficult to compare successive examinations over time in the same woman by the same operator or different operators (16).The Pelvic Organ Prolapse Quantification system (POP-Q) (17) recommended by the International Consultation on Incontinence (IUGA/ICS) refers to an objective, site-specific system for describing, quantifying, and staging POP in women (15, 18). In this system, specific measurements at nine sites are recorded in a tic- tac-toe grid (Figure 56.1). There are six defined points for measurement in the POPQ system—Aa, Ba, C, D, Ap, and Bp—and three other landmarks—gh, tvl, and pb (see caption for Figure 56.1 for definitions). Each is measured in centimetres above or proximal to the hymen (negative number) or centimetres below or distal to the hymen (positive number) with the plane of the hymen being defined as zero (0). The hymen was selected as the reference point because it is more precisely identified. Pelvic organ prolapse quantification system (POP-Q) provides a standardized tool for documenting, comparing, and communicating clinical findings with proven interobserver and intraobserver reliability (17).
The Baden-Walker Halfway Scoring System is the next most commonly used system. It consists of four grades:
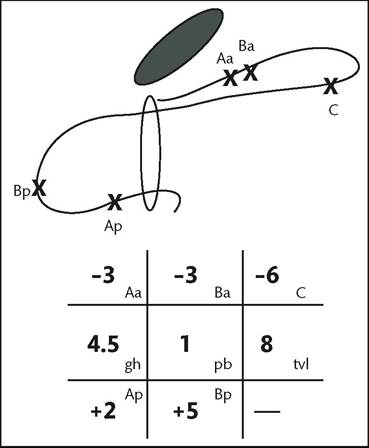
Figure 56.1 POP-Q scoring grid. Aa, point A anterior, Ap, point
A posterior, Ba, point B anterior; Bp, point B posterior; C, cervix or vaginal cuff; D, posterior fornix (if cervix is present); gh, genital hiatus; pb, perineal body; tvl, total vaginal length.
Source data from Persu C, Chapple CR, Cauni V, et al. Pelvic Organ Prolapse Quantification System (POP-Q) - a new era in pelvic prolapse staging.J Med Life 2011;4(1):75-81.
• Grade 0—no prolapse.
• Grade 1-halfway to hymen.
• Grade 2—to hymen.
• Grade 3—halfway past hymen.
• Grade 4—maximum descent.
Although descriptive, some shortcomings exist in the Baden- Walker system. For instance, a strategically placed 1 cm increase in prolapse results in an increase in the assigned stage. It does not provide information on the total vaginal length and the extent of gaping of the genital hiatus. In addition, inter-observer agreement was lower with the Baden-Walker system compared to the POP-Q system (19).
All examinations for POP should be performed with the woman's bladder empty (and if possible an empty rectum too). Fullness of the bladder or rectum has been shown to restrict the degree of descent of the prolapse (20). The choice of the woman's position during examination (e.g. left lateral, supine, standing, or lithotomy) is that which can best demonstrate maximum POP. If the prolapse can't be seen in one position, then examination with the woman standing may be considered. The degree of POP assessed with the patient in the lithotomy position correlates well with assessment performed upright; however, overall there is a higher degree of prolapse with upright examination (21).
The hymen remains the fixed point of reference for prolapse description. The descent of one or more of the anterior vaginal wall, posterior vaginal wall, the uterus (cervix), or the apex of the vagina (vaginal vault or cuff scar after hysterectomy) on maximum Valsalva or coughing needs to be measured. Level of the hymen is taken as a fixed point and descent of pelvic organs is measured in relation to the level of the hymen (Box 56.2).
A simplified POP-Q scoring, with the above-mentioned stages 1-4 without inclusion of stage 0, has been described by Swift et al.
(22). Higher-stage anterior vaginal wall prolapse will generally involve uterine or vaginal vault/apex (if uterus is absent) descent. Occasionally, there might be anterior enterocele (hernia of peritoneum and possibly abdominal contents) formation after prior reconstructive surgery. Posterior vaginal wall prolapse would usually be due to rectal protrusion into the vagina (rectocele). Higher-stage posterior vaginal wall prolapse after prior hysterectomy will generally involve some vaginal vault (cuff scar) descent and a possible enterocele. Enterocele formation can also occur in the presence of an intact uterus.Box 56.2 POP-Qstaging
• Stage 0: no prolapse is demonstrated.
• Stage I: most distal portion of the prolapse is more than 1 cm above the level of the hymen.
• Stage II: most distal portion of the prolapse is 1 cm or less proximal to or distal to the plane of the hymen.
• Stage III: the most distal portion of the prolapse is more than 1 cm below the plane of the hymen but everted at least 2 cm less than the total vaginal length.
• Stage IV: complete eversion of the total length or eversion at least within 2 cm of the total length of the lower genital tract is demonstrated.