Complications of perineal trauma
Postpartum haemorrhage
Vaginal and cervical tears may result in postpartum haemorrhage, which is managed with primary surgical repair and vaginal packing as required. In ongoing bleeding after suturing, pelvic arterial embolization may be considered (118).
Haematomas
Paravaginal (infralevator and supralevator) haematomas
The LAMs divide the paravaginal space into an upper or supralevator fossa and a lower or infralevator fossa (Figure 59.10). A paravaginal
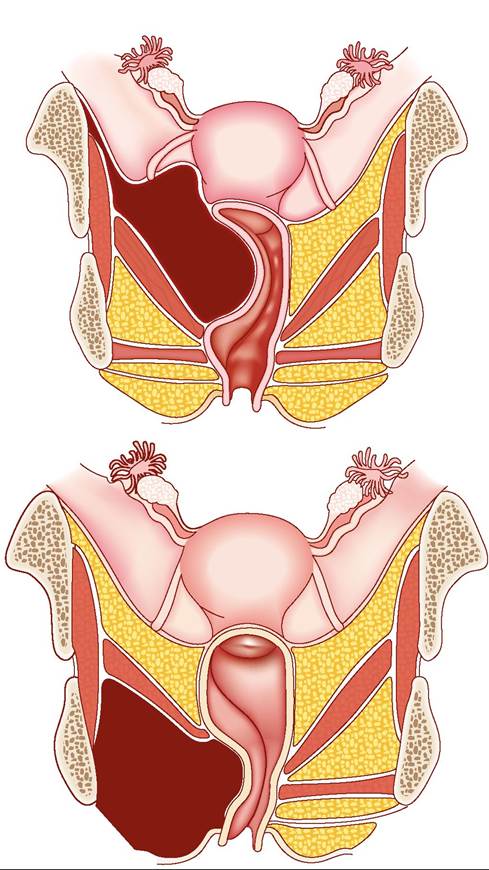
Figure 59.10 (a) Infralevator haematoma. (b) Supralevator haematoma.
Reproduced with permission from Nikolopoulos and Doumouchtsisl Healing process and complications. In: SK Doumouchtsis (Ed) Childbirth Trauma, p. 201 (2016) with permission from Springer
haematoma is typically confined to the upper or lower compartment, although massive haemorrhage can extend through the levator barrier.
Haemorrhage into the infralevator space can cause extensive oedema and ecchymosis of the labia, perineum, and lower vagina with severe vulval, vaginal, and perineal pain. Anorectal tenesmus and urinary retention may be caused by extension of the haematoma.
A supralevator haematoma can be palpable as a mass protruding into the vaginal wall potentially causing vaginal or rectal pain and pressure symptoms.
In small infralevator haematomas, ice packs, analgesia, and bladder catheterization may be adequate. Surgical evacuation is indicated in large or expanding haematomas, to prevent tissue ischaemia and necrosis, septicaemia, and further haemorrhage.
Treatment options for supralevator haematomas include conservative measures with vaginal packing for 12-24 hours and haemoglobin monitoring. If bleeding is ongoing, arterial embolization or ligation may be indicated.
The use of balloon tamponade has been reported (119).Vulval haematoma
Vulval haematoma usually results from injuries to the branches of the pudendal artery during vaginal delivery and sometimes in conjunction with episiotomy. Superficial haematomas can extend anteriorly over the mons to the inguinal ligament. Necrosis caused by pressure and rupture of the tissue surrounding the haematoma may lead to external haemorrhage.
Large haematomas usually require exploration in theatre. Initial resuscitation with intravenous fluids may be required, and blood should be sent for haemoglobin, coagulation screen, and crossmatch.
Following a skin incision, the haematoma is evacuated and bleeding points are identified and ligated. The dead space is obliterated with interrupted sutures and the skin incision is closed appropriately. Antibiotic prophylaxis, urinary catheterization, rectal examination, and adequate analgesia are advisable.
Perineal pain and dyspareunia
Perineal pain is common after perineal trauma and was reported to affect 92% of women, resolving in 88% of cases at 2 months (120). In most cases pain is manageable with simple analgesia, however, a small number of women will develop chronic pain. Pain following OASIS can be severe. Severe perineal pain has been observed in 100% of women on day 1 and 91% of women on day 7 following third-degree and fourth-degree tears (121, 122).
Treatment options for perineal pain include oral or rectal analgesia (122). Following primary repair after third- or fourth-degree tears, laxative use will prevent from faecal impaction and possible damage to the recently repaired sphincter muscles. Laxatives result in an earlier and less painful first bowel motion and earlier discharge home (122).
Women who practise perineal massage have lower perineal pain scores than those who do not. Pain refractory to conservative measures may be addressed with local perineal injections with hydrocortisone, Marcaine, and hyaluronidase, which appear well tolerated and lead to a significant improvement in pain scores (123).
Perineal trauma is associated with a decrease in sexual function at 6 months postpartum. Second-degree tears are associated with an 80% increased risk of dyspareunia and third/ fourth- degree tears with a 270% increased risk of dyspareunia (124, 125). Dyspareunia is pain that occurs during sexual intercourse, and affects a significant number of women following childbirth—approximately 20% at 3 months postpartum (122, 126). Twenty per cent ofwomen take longer than 6 months before sexual intercourse becomes comfortable. Suboptimal repair of an episiotomy or vaginal tear can also lead to longstanding perineal discomfort and dyspareunia, so attention to anatomy and good surgical technique is important (127).
Dyspareunia secondary to scarring or tightness at the fourchette following suturing is initially treated with dilators and topical oestrogens. Significant scarring and constriction of the introitus may require surgical revision. The appropriate surgical procedure depends on the site and extent of the vaginal constriction, the state of the surrounding tissue, and the overall length and calibre of the vagina. Fenton's procedure, Z-plasty, vaginal incision of constriction ring, vaginal advancement, or placement of free skin graft are reported techniques (128). Levator muscle spasm can be treated with botulinum toxin injections (129).
Perineal wound infection and breakdown
In one study, one in ten women with a perineal tear that required suturing developed perineal wound infection, defined as the presence of any two of the following markers: perineal pain, wound dehiscence, or purulent vaginal discharge (130). Antepartum risk factors for infection include extremes of maternal age, smoking, poor hygiene, poor nutrition, and pre-existing medical conditions such as diabetes, immunocompromise, severe anaemia and bacterial vaginosis, chlamydia, gonorrhoea, or trichomonas infection. Intrapartum factors include prolonged rupture of membranes, thick meconium, prolonged labour, intrapartum pyrexia, multiple internal examinations, operative vaginal delivery, poor aseptic technique, manual removal of placenta, and retained products.
Postpartum factors include delayed or omitted prophylactic antibiotics, suboptimal haemostasis, haematoma, contamination of wound, and residual dead space following repair (131). In cases of second-degree tears, antibiotics are not routinely required. Antibiotic prophylaxis in cases of third/fourth-degree tears results in a lower risk of wound infection (132). Broad-spectrum antibiotics including anaerobic cover are recommended. Most perineal infections resolve with antibiotics and good perineal hygiene.Perineal wound breakdown can lead to significant morbidity and has an incidence of 0.1-4.6% (133-135). Up to 80% of wound dehiscence cases are secondary to wound infection. There is limited evidence on best practice for the management of perineal wound breakdown. Most practitioners manage these cases conservatively, whereas others offer secondary suturing. A common approach is to allow healing by secondary intention; however, this is a slow process. Resuturing of perineal wound dehiscence within the first 2 weeks following childbirth is another approach and may be associated with less perineal pain during the healing process for up to 6 months after delivery, an improvement of dyspareunia, continuation of exclusive breastfeeding, and increased satisfaction with the aesthetic result of the perineal wound (136). Although there is insufficient evidence to support or refute secondary suturing, the time of presentation and the degree of granulation formation may influence the choice of management.
Labial complications
Spontaneous approximation and healing of labial lacerations may lead to distorted anatomy and dyspareunia. Prevention of labial or clitoral adhesions may be achieved through personal hygiene techniques and instructing women to manually gently separate the labia several times a day while urinating. Oestrogen cream has been used for the management of adhesions of the external genitalia. Surgical correction may be necessary when medical treatment fails (137).
Obstetric fistula
Obstetric fistula, an opening between the vagina and the bladder and/or the rectum, is most frequently caused by unattended prolonged labour, when the pressure of the baby's head against the mother's pelvis causes ischaemia to delicate tissues and necrosis. Obstetric fistula is one of the most severe childbirth injuries that occur when labour is allowed to progress for a long period without timely intervention. More than 2 million women worldwide live with vesicovaginal fistula or recto-vaginal fistula and the majority of them reside in Africa and Asia (138-140).