Management of perineal trauma
The repair of perineal trauma should be undertaken by an appropriately qualified practitioner as soon as possible after delivery to reduce the risk of bleeding and tissue oedema.
Adequate analgesia will enable exposure of the trauma and good visualization without causing additional discomfort to the woman. Local anaesthesia with 1% lidocaine or an epidural top-up are suitable options for uncomplicated tears or episiotomies; however, in cases of severe trauma, significant pain, or bleeding, regional anaesthesia is required. Principles of asepsis, good lighting, and meticulous swab counts should be followed.For the repair of first- and second- degree tears or perineal skin injuries some practitioners prefer to leave the perineal skin unsutured to heal by secondary intention, as avoiding suture material has been associated with better skin sensation when assessed at 1 year postpartum (98). In two trials on suturing versus non-suturing of first- and second-degree perineal tears (99, 100), there was a similar degree of discomfort with both approaches, but the wound healing appears better after subcuticular closure.
Overall there is no consistent evidence to support one option over the other with regard to healing and recovery, however a Cochrane review concluded that there may be a better feeling of well-being if the wound is left unsutured (101).
Polyglactin 910 (Vicryl, Ethicon) and rapidly absorbable polyglactin 910 material (Vicryl Rapide) are the two most common suture materials used for perineal repair. The tensile strength of Vicryl Rapide is reduced in 10-14 days and it is absorbed in 42 days. Vicryl Rapide is associated with a significant reduction in the need for suture removal up to 3 months postnatally.
Studies have reported less short-term pain and lower resuturing requirements with polyglactin 910 compared to chromic catgut (102).
Rapidly absorbed polyglactin is associated with less shortterm pain, wound dehiscence, wound infection, and discomfort (103, 104). Comparing standard polyglactin 910 versus rapidly absorbed polyglactin 910, there was no difference in pain at 10 days or dyspareunia at 3 months, but there was a higher requirement for suture removal in the standard polyglactin 910 group (105).Repair of first- or second-degree tears
• First-degree tears and labial tears can be left unsutured, unless there is significant bleeding or concerns about suboptimal anatomical alignment. In unsutured bilateral labial tears there is a risk of labial adhesions and voiding difficulties.
• The first suture is inserted and tied just above the vaginal apex of the tear to secure haemostasis and optimal anchoring of the suture line.
• The vaginal part of the tear is sutured with a continuous, nonlocking technique, which is associated with less pain and dyspar- eunia compared to interrupted sutures (106).
• The perineal muscles are approximated and sutured with the same continuous suture, aiming to close the dead space and approximate the skin edges as well, which can subsequently be closed without tension. If the muscle tear is deep, a second continuous layer of suturing may be required.
• The perineal skin is closed with a continuous subcuticular suture.
• Episiotomy suturing can be undertaken using this continuous suturing technique (Figure 59.7).
• A vaginal and rectal examination is carried out following completion of the suturing, to ensure the repair is complete, restoration of
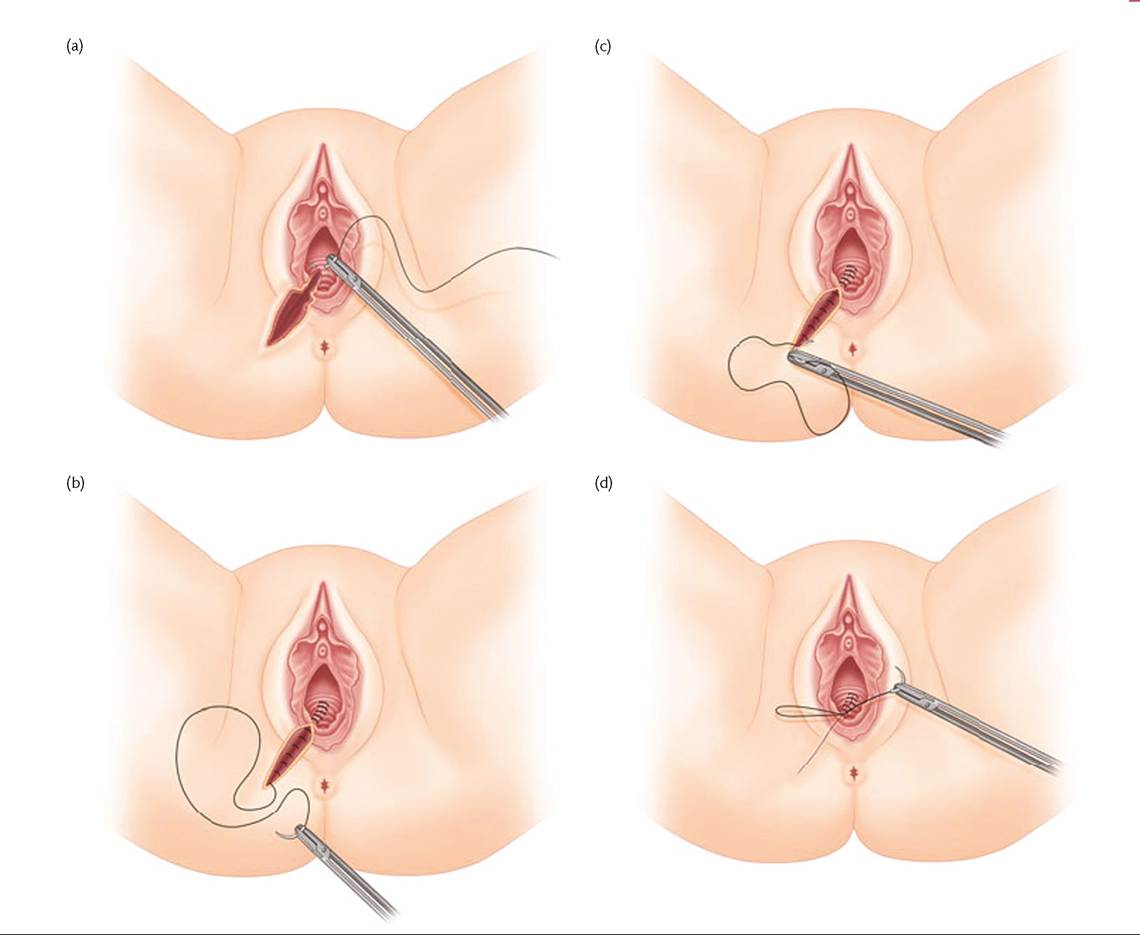
Figure 59.7 Episiotomy repair: continuous non-locking suturing technique for the repair of a mediolateral episiotomy. (a) The apex of the episiotomy is sutured and secured first. Using the same suture, suturing of the vaginal wall follows using a continuous layer. (b) Suturing of perineal muscles.
(c) Suturing of perineal skin using subcuticular continuous suture. (d) Knot placement and tying just above the level of hymen.
Reproduced from Kalis et al. Episiotomy In: SK Doumouchtsis (Ed) Childbirth Trauma, p. 81 (2016) with permission from Springer.
the anatomy is optimal, and there is no suture material inadvertently placed in the rectal canal.
Repair of third- and fourth-degree tears
Repair of third- and fourth-degree tears should be undertaken by a clinician who has undergone formal training and attained competence in repair of these injuries (3).
Although it is good practice to repair perineal trauma as soon as possible after the delivery, there is no difference in functional outcome if the repair is delayed for a few hours (e.g. because of a lack of trained staff) (107). Repair is best undertaken in the operating theatre with good lighting to achieve optimal exposure and access to the trauma, using aseptic technique, and under regional or general anaesthesia for muscle relaxation, which allows identification and mobilization of the torn ends of the anal sphincter.
• A buttonhole tear is repaired with two layers of interrupted polyglactin sutures to minimize the risk of a fistula. In the case of gross faecal contamination of the wound, a colorectal surgeon should be called for review and advice.
• In a fourth-degree tear, the anal epithelium is repaired with interrupted 3/0 polyglactin sutures with the suture knots in the anal canal.
• Internal anal sphincter injuries are repaired separately with interrupted sutures using a 3/0 polydioxanone (PDS) or polyglactin suture. Identification and repair of the internal anal sphincter separately is associated with better continence outcomes (108).
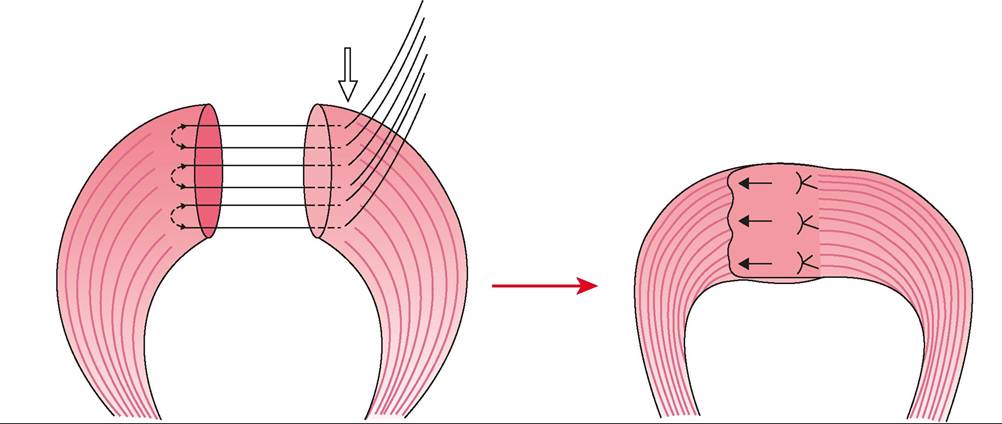
Figure 59.8 Technique of overlapping external anal sphincter repair.
Reproduced from Cardozo and Staskin (Eds) Textbook of Female Urology and Urogynecology 2nd Ed.
2006 Informa Healthcare p1117 with permission from Informa.• The torn ends of the external anal sphincter are held with Allis tissue forceps and sutured using either an overlap (Figure 59.8) (if the muscle is completely torn, i.e. 3B/3C) or end-to end approximation (Figure 59.9).
Although there is no difference in incidence of perineal pain, dyspareunia, faecal incontinence, or flatal incontinence between the two techniques, there is some evidence of a lower incidence of faecal urgency and lower anal incontinence symptom scores in the overlap group (90). A study of 64 women randomized to overlap or end-to-end repair reported differing results. For the primary outcome of faecal incontinence, there was a significant difference favouring overlap repair (0% vs 24%) (109). Faecal urgency was also significantly more likely in the end-to-end group. However, the authors of a Cochrane review concluded that there is insufficient evidence to recommend one method over the other (90).
• Following anal sphincter repair, a reconstruction of the perineal muscles will provide additional support to the repaired sphincter muscles and possible risks of subsequent trauma may be reduced.
• Repair of the vagina and perineum should proceed as for a second-degree tear.
• A rectal examination should be carried out to ensure that the repair is complete and no sutures have been placed inadvertently through the rectal mucosa.
• An indwelling catheter is left in the bladder for 12-24 hours.
• Broad-spectrum antibiotics intraoperatively and oral antibiotics for 5-7 days postoperatively are indicated, as wound infection and breakdown may result in fistula formation or anal incontinence.
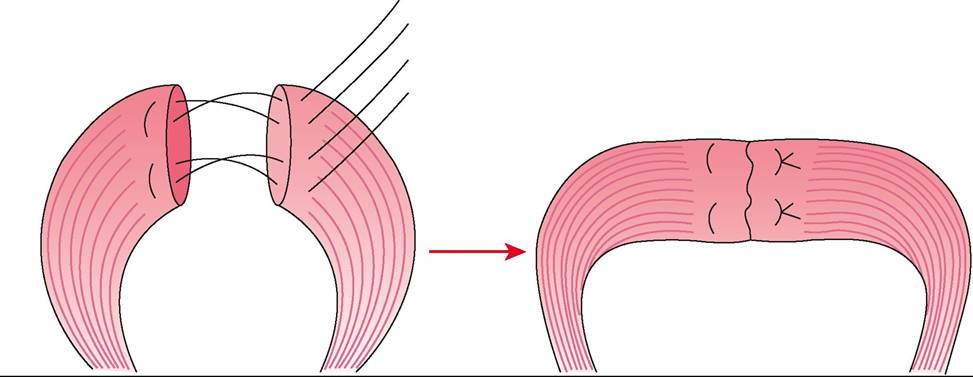
Figure 59.9 Technique of end-to-end external anal sphincter repair.
Reproduced from Cardozo and Staskin (Eds) Textbook of FemaJe Urology and Urogynecology 2nd Ed. 2006 Informa Healthcare p1115 with permission from Informa.
• Laxatives are recommended postnatally to avoid constipation, which could disrupt the repair. A stool softener plus a bulking agent for 10 days is recommended, although there is a higher incidence of anal incontinence in the early postnatal period with this regimen compared to stool softeners alone (110).
• Adequate pain relief such as diclofenac suppositories is recommended (111). Constipating analgesics should be avoided.
• Documentation of the extent of the tear and the type of repair, including diagrams, is useful for debriefing the woman and in case of litigation.
Outcomes following OASIS
The reported incidence of anal incontinence following OASIS seems to be lower in more recent studies than in the past, probably due to improvements in training for diagnosis and repair.
In the first 12 months postnatally, symptoms of anal incontinence have been reported in 21-43% of women with OASIS (112, 113). Sonographic evidence of internal anal sphincter injury in the early postnatal period is a significant risk factor for the development of anal incontinence (113). Diagnosis of internal anal sphincter trauma and optimal repair is therefore extremely important. Other independent factors associated with a higher risk of anal incontinence include fourth-degree tears (112) and evidence of persistent sphincter defects. The aetiology of anal incontinence in postnatal women is multifactorial. Anal sphincter defects account for only 45% of cases of anal incontinence (114). Pre-existing anal incontinence and pudendal nerve injury may play a role.
Follow-up after OASIS
Women with OASIS should be reviewed at 6-12 weeks postna- tally ideally in a dedicated clinic by a professional with training in perineal trauma, and access to endoanal ultrasound and anal manometry. Endoanal ultrasonography is more accurate than clinical examination for the diagnosis of sphincter defects. There is significant association between sonographic sphincter defects, anal incontinence symptom scores, and low sphincter pressures (115, 116). Sonographic sphincter defects are also predictive of the development of faecal incontinence in later life (117).
Women with mild symptoms such as faecal urgency can usually be managed by dietary modification, constipating agents, and physiotherapy with bowel retraining and biofeedback. Those with more severe incontinence symptoms should be referred to a colorectal surgeon. Counselling on mode of delivery in a future pregnancy should be offered.