Diabetes mellitus
Preconceptional counselling is equally important for women with type 1 or type 2 diabetes mellitus. The main goals of preconceptional counselling around diabetes includes the following: optimizing
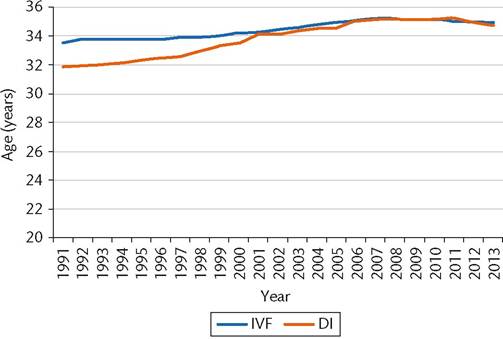
Figure 6.3 Average age of women undergoing in vitro fertilization (IVF) and donor insemination (DI) treatment using fresh eggs (1991-2013).
Source data from Human Fertilisation & Embryology Authority Fertility Treatment in 2013. Retrieved from http://www.hfea.gov.uk/docs/HFEA_Fertility_Trends_and_Figures_ 2013.pdf 2013.
and fetal outcomes, including congenital malformations, miscarriage, preterm delivery, pre-eclampsia, macrosomia, and perinatal mortality (20-22). In the first trimester, hyperglycaemia is a known teratogen, resulting in neural tube defects and fetal heart malformations (23, 24). As can be seen in Figure 6.5, studies have shown that hyperglycaemia is the primary driver in these adverse events, and therefore tighter glycaemic control in the preconception period is critical.
Goals for glycaemic control in the preconception period are in line with the conception period, which is to optimize glycaemic control. The following parameters provide a framework for glycaemic control in the preconception period, with a goal of near-normal blood glucose while avoiding hypoglycaemia:
• Fasting glucose concentration of 5.3 mmol/L or lower.
• 1-hour postprandial glucose concentration of 7.8 mmol/L or lower, or 2-hour postprandial glucose concentration of 6.4 mmol/ L or lower.
• Glycated haemoglobin level of less than 6.5% in the preconception period.
preconceptional glycaemic control; risk management of adverse fetal and maternal outcomes; education around diabetes self-care; medication changes; and managing pre-existing complications and comorbidities associated with diabetes. Women of reproductive age with type 1 or 2 diabetes should be counselled to supplement with folic acid, 1.0 mg daily, beginning at least 3 months before conception.
One of the important factors in consideration of the health of the fetus in a mother with diabetes is the physiology of glucose and insulin in pregnancy. Glucose readily crosses the placenta via the GLUT1 transporter, while insulin does not. Because of this, optimization of glycaemic control is of utmost importance in the preconception period due to the teratogenic effects of hyperglycaemia on the fetus. There are increased risks of both adverse maternal
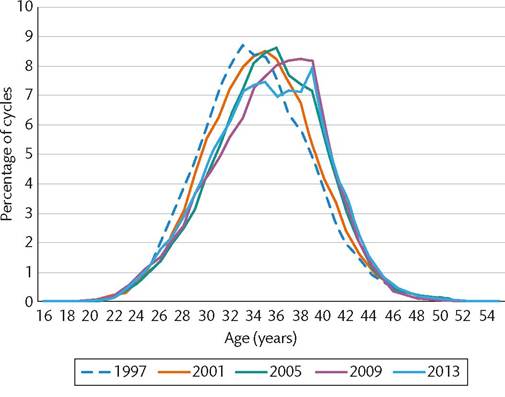
Figure 6.4 Percentage of cycles started by patients age at start of treatment (1997-2013).
Source data from Human Fertilisation & Embryology Authority. Fertility Treatment in 2013. Retrieved from http://www.hfea.gov.uk/docs/HFEA_Fertility_Trends_and_Figures. 2013.pdf. 2013.
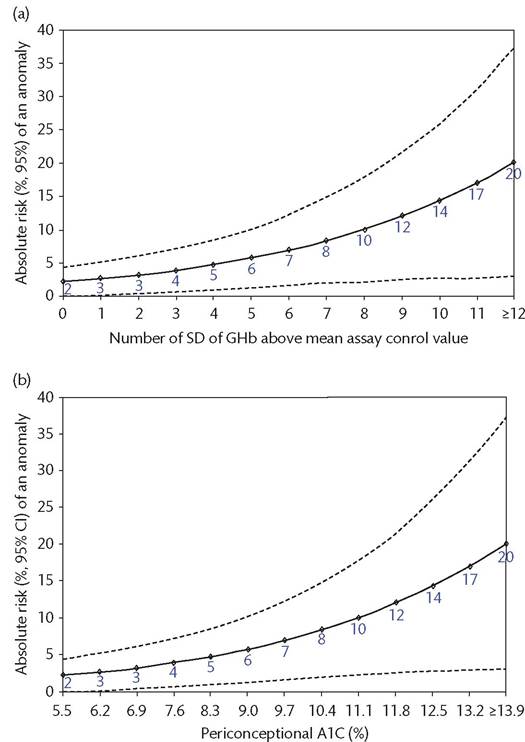
Figure 6.5 Risk of a major or minor anomaly according to periconceptional A1C.
Reproduced from Guerin A, Nisenbaum R, Ray JG. Use of maternal GHb concentration to estimate the risk of congenital anomalies in the offspring of women with prepregnancy diabetes. Diabetes Care. 2007;30(7):1920-5 with permission from American Diabetes Association.
• Avoid hypoglycaemia and maintain a capillary plasma glucose concentration of at least 4.0 mm/L.