Obesity and preconceptional counselling
Almost a third of women entering pregnancy in the United States are obese (10). The challenge of obesity in pregnancy is multifaceted. While obesity is foremost associated with reduced fertility, there are many other factors that must be considered.
Obesity in women of reproductive age is important both because of the risks of associated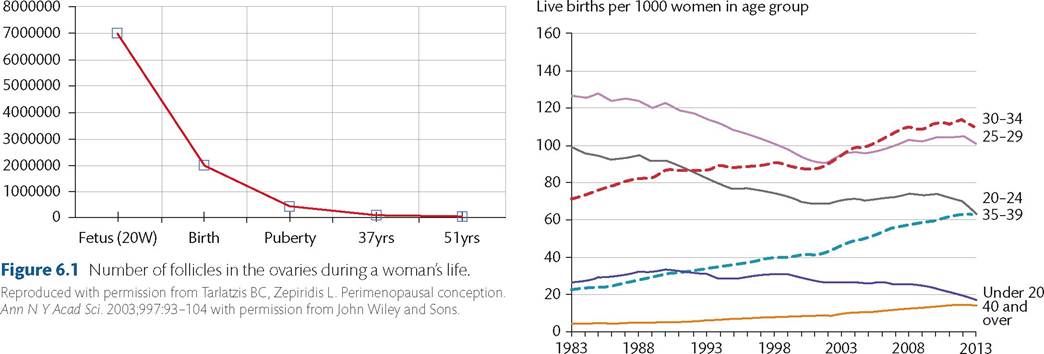
Figure 6.2 Maternal age groups at childbirth in England and Wales, 1983-2013.
Source data from Office for National Statistics, UK. Statistical Bulletin for Births in England and Wales. Retrieved from http://www.ons.gov.uk/ons/dcp171778_371 129.pdf. 2013.
downstream diseases (including type 2 diabetes and cardiovascular disease) and because obesity is associated with poor outcomes for both the pregnant woman and the fetus. Such outcomes include fetal anomalies, gestational diabetes, pre-eclampsia, medically indicated preterm birth, caesarean delivery, and fetal macrosomia; longer- term risks for offspring include childhood obesity and the metabolic syndrome.
Physiology of obesity in preconception
Studies have shown that there is reduced fertility in obese patients, which is hypothesized to be a result of insulin resistance-induced oligo-ovulation and anovulation from hormonal and metabolic parameters (11, 12). Although polycystic ovarian syndrome is known to be a key contributor in ovulatory dysfunction, there is an independent contributing factor from obesity as well. Key hormonal effects include reduction of sex hormone-binding globulin, which effectively leads to functional hyperandrogenism, an increased production of oestrogen, and subsequent reduction in gonadotropin secretion (12). Additionally, there is evidence to show that leptin, an adipokine produced by adipose tissue, can directly inhibit ovarian function (12, 13).
Table 6.1 Rate of Down syndrome at live birth, according to maternal age
| Maternal age at delivery (years) | Incidence of Down syndrome per 1000 live births |
Source data from Chuckle HS, Wald NJ, Thompson SG. Estimating a woman's risk of having a pregnancy associated with Down's syndrome using her age and serum alphafetoprotein level. BrJ Obstet Gynaecol1987;94(5):387-402.
Pregnancy after bariatric surgery
Pregnancy following bariatric or weight loss surgery presents unique challenges and considerations. Bariatric surgery is an option for weight loss provided by the National Health Service for patients with a body mass index of at least 40 kg/m2, or 35 kg/m2 with significant comorbidities. During preconceptional counselling, topics including timing of conception, health of mother and baby, and fertility can be discussed. Bariatric surgery has the potential to reduce the risks of gestational diabetes and large-for-gestational-age neonates but is also associated with some risks in pregnancy.
There is currently limited evidence to show that women should wait a specific time prior to conceiving (14, 15); however, according to the recommendations from the American College of Obstetricians and Gynecologists, women should be advised to delay conceiving until 12-24 months after surgery, the period when the most rapid weight loss occurs (16). Due to the different absorption pattern of the gastrointestinal tract following bariatric surgery, nutritional deficiencies have been reported, and dietary supplementation should be considered in this specific population of women in the preconception period (17). Specific daily nutrient supplementation recommendations include greater than 65 mg of iron, greater than 400 mcg of folic acid, greater than 400 IU of vitamin D, and 350 mcg of vitamin B.
The pathophysiology that contributes to obesity and infertility appears to be multifactorial, with contributions primarily from insulin resistance and altered hormone profiles (18). Some women undergo bariatric surgery in attempts to reverse some of these effects, and there have been reports of successful increases in fertility following bariatric surgery (17, 19).