Diagnostic categories in infertility
Based on the previously discussed investigations, infertile couples can be classified into five main diagnostic categories. Male factor infertility accounts for 30% of cases. Ovulation disorders account for 25% and tubal factor for 20% of cases (10) whereas endometriosis is the underlying factor in approximately 2-10%.
One in four couples will have unexplained infertility where no obvious cause is found after standard infertility investigations (10).Ovulation disorders
The hypothalamic-p ituitary-o varian axis orchestrates the process of follicular recruitment and ovulation in each monthly cycle. Disruption of this well-coordinated rhythmic activity can lead to ovulation disorders which have been classified by WHO into three groups (Table 51.5).
Tubal factor infertility
The fallopian tubes play an important role in natural conception by assisting the transport of eggs from the ovaries and providing a site where they can be fertilized by viable sperm. The ciliary action of the endosalpinx helps the migration of the fertilized egg to the uterus for implantation.
Blocked or damaged tubes can result from pelvic inflammatory disease such as that caused by chlamydial infection. Pelvic abscess or infection following on from appendicitis or bowel problems and adhesions related to abdominal/pelvic surgery can also be responsible for tubal damage and subsequent infertility.
Male factor infertility
Impaired sperm production or their transport can result in male infertility. Most cases are idiopathic but known causes include genetic factors, testicular maldescent or trauma, and congenital absence of vas (often related to cystic fibrosis), sexual infections, and iatrogenic causes (Figure 51.4).
Unexplained infertility
In a quarter of all couples, standard tests including semen analysis, serum progesterone to detect ovulation, and tubal patency test are normal and infertility is deemed to be unexplained.
A number of putative factors which cannot be diagnosed by the standard tests have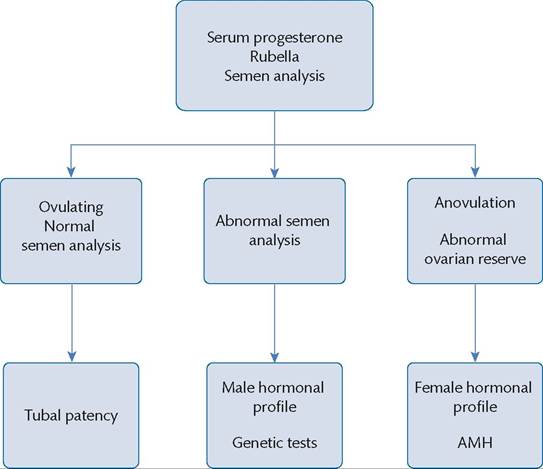
Figure 51.6 Hierarchy of investigations. AMH, anti-Mullerian hormone.
been thought to be linked to this condition, including mild ovulatory dysfunction, compromised tubal transport, suboptimal gamete quality, and immunological causes.
Lack of a specific diagnosis is challenging for the couples but some feel reassured by the fact that, in the absence of an absolute barrier to conception, the chances of spontaneous pregnancy are relatively high (41). The prognosis is better for those with a shorter duration of infertility and younger age of the female partner or where a previous conception has occurred.
Endometriosis
Endometriosis is a common condition that is characterized by presence of endometrial tissue outside the uterine cavity in sites
such as the ovarian fossa, pelvic peritoneum, and uterovaginal and rectovaginal folds. Symptoms include pelvic pain, dysmenorrhea, dyspareunia, or heavy bleeding but some women may be totally asymptomatic. Infertile women are six to eight times more likely to have endometriosis (42). The precise mechanism by which endometriosis affects fertility remains to be elucidated (Table 51.6) (43) but a number of theories have been proposed. These include an abnormal immune response affecting implantation, pelvic adhesions posing an obstruction to egg pick up after release or transport down the fallopian tube, and increased cytokine levels in the peritoneal and follicular fluid impacting the oocyte quality.
Table 51.5 Ovulation disorders
| WHO group | I Disorder | I Cause | I Factors |
| Group I | Hypogonadotropic hypogonadism | Hypothalamus and pituitary dysfunction | Functional hypothalamic dysfunction—excessive weight loss such as in anorexia nervosa, exercise, stress, drugs, iatrogenic Kallmann syndrome (isolated gonadotropin deficiency and anosmia) Pituitary tumour, pituitary infarct (e.g. Sheehan syndrome)Idiopathic |
| Group II | Normogonadotropic normogonadism | Ovarian dysfunction | Polycystic ovary syndrome Thyroid dysfunction Hyperprolactinaemia Androgen excess (congenital adrenal hyperplasia, androgen-secreting adrenal and ovarian tumour) |
| Group III | Hypergonadotropic hypogonadism | Ovarian failure | Iatrogenic (e.g. surgical menopause, after radiotherapy or chemotherapy) Genetic (e.g. Turner syndrome) Autoimmune causes Infection Idiopathic |
Source data from World Health Organization. 1975. The Epidemiology of Infertility. Report of WHO Scientific Group on the Epidemiology of Infertility, Technical Report Series No. 582. Geneva: World Health Organization.
Table 51.6 The precise mechanism by which endometriosis affects fertility remains to be elucidated but a number of theories have been proposed
| Mechanism | I Possible effect |
| Distortion of pelvic anatomy/ pelvic adhesions | Ovum release, ovum pick-up by the tube, tubal transport of fertilized egg |
| Increased concentration of inflammatory markers such as prostaglandins and cytokines in peritoneal fluid | Can effect egg, sperm, embryo, or fallopian tube function |
| Altered cell-mediated immunity, increased IgA, IgG, and lymphocytes in endometrium | Impaired endometrial receptivity |
| Endocrine and ovulatory disorders | Luteal phase dysfunction, abnormal follicular growth |
| Altered progesterone and cytokine in follicular fluid | Poor oocyte quality affecting embryo development |
| Reduced expression of integrin and enzyme necessary for implantation | Reduced implantation |
Source data from Endometriosis and infertility: a committee opinion.
The Practice Committee of the American Society for Reproductive Medicine. Fertility and Sterility, 2006;86 Suppl 5:S156-60.
Management
The management of subfertile couples starts in primary care with prepregnancy advice on lifestyle measures to optimize BMI and smoking cessation—where appropriate. Information about timing and frequency of intercourse can be helpful for some couples. Preconception folic acid supplementation is recommended to reduce the risk of neural tube defects in the newborn. Existing medical conditions should be treated with input from appropriate specialists and the impact of any regular medication on fertility and pregnancy should be considered. Cervical smears should be up to date and abnormal smears should be managed prior to initiating fertility treatment.
Management of ovulation disorders
WHO group I disorders (hypogonadotropic hypogonadism)
Women with a BMI less than 18 kg/m2 with or without a history of an eating disorder can benefit by weight gain towards a normal BMI of 19 kg∕m2 or above. Women with hypothalamic anovulation can be treated with pulsatile administration of GnRH agonists or gonadotropins to induce ovulation. Intravenous pulsatile administration of GnRH is administered by means of a portable pump and mimics normal cycle physiology resulting in unifollicular ovulation. This is an advantage compared to the use of gonadotropins which can result in multifollicular ovulation, thus increasing the chance of multiple pregnancy and ovarian hyperstimulation. The disadvantage, however, is that the use of a pump can be inconvenient for many women.
WHO group II disorders (PCOS)
Lifestyle modifications in the form of weight loss and structured exercise have been shown to be beneficial in improving the hormonal profile and insulin resistance in obese women with PCOS (44).
Oral ovulation induction
Cases diagnosed with oligo-ovulation or anovulation due to PCOS can be treated with ovulation-induction medications with the aim to induce single follicle ovulation.
The first-line treatment is usually with clomiphene citrate which is a selective oestrogen receptor modulator. It blocks the negative feedback effect of oestrogen on the hypothalamus resulting in increased gonadotropin secretion and induction of ovulation. Clomiphene is taken orally with a starting dose of 50 mg from day 2-3 of the menstrual cycle for 5 days. The dose can be increased by 50 mg each month in case of no ovulation to a maximum dose of 150 mg. Minor side effects include nausea, headache, hot flushes, and blurring of vision. Multiple pregnancies are a major risk. An increased risk of borderline ovarian cancer associated with clomi- phene use has not been confirmed (45). Ovulation can be detected by using urinary LH kits or measuring the serum LH level and intercourse is timed to the LH surge. Clomiphene is recommended for up to six ovulatory cycles as the majority of pregnancies are seen within this timeframe. A conception rate of up to 22% per cycle in women ovulating on clomiphene has been reported (46). If a conception doesn't result, further investigations should be carried out to rule out tubal factor. Tamoxifen is an alternative to clomi- phene and advised in a dose of 20-40 mg for 5 days starting from day 3 of the cycle. The antioestrogenic effect of tamoxifen is milder than clomiphene and this reduces the effect on cervical mucus. Pregnancy rates have been reported similar to clomiphene (OR 1.00; 95% CI 0.48-2.09) (47).
In women with PCOS, who are not ovulating on clomiphene alone, adding metformin to clomiphene can increase ovulation and pregnancy rates but may not improve livebirth rates (48).
The aromatase inhibitor, letrozole, has also been used for ovulation induction in women with PCOS. It is taken orally starting from day 2-3 of the cycle for 5 days in doses from 2.5 to 7.5 mg daily. The efficacy of letrozole compared to clomiphene in improving the pregnancy and live birth rate has been extensively researched and further studies have been recommended to strengthen the evidence (49).
Therefore, letrozole has not yet established its place in routine clinical practice.Second-line ovulation induction strategies
Women who fail to respond to clomiphene can be offered the second-line option of exogenous gonadotropins or laparoscopic ovarian drilling. The use of gonadotropins is associated with increased chances for multiple pregnancy and hyperstimulation. Ultrasound monitoring is therefore mandatory.
Ovarian diathermy has been shown to reduce testosterone and LH levels with correction of the hormonal imbalance associated with PCOS, resulting in restoration of ovulation. The procedure has been shown in some studies to be as effective as medical treatments, without the risk of hyperstimulation. However, the risks associated with the surgical procedure and general anaesthetic remains. There are also concerns about the long-term effect on ovarian function which can compromise future fertility (50).
WHO group III disorders (ovarian failure)
Women with a diagnosis of ovarian failure need oestrogen supplementation in the form of hormonal replacement therapy or a combined oral pill. Assisted reproduction by means of egg donation is usually necessary for conception.
Hyperprolactinaemia
Raised prolactin levels can decrease the pulsatile secretion of gonadotropin leading to anovulation and subfertility. Dopamine agonists such as bromocriptine, cabergoline, pergolide, quinagolide, and cabergoline have been used to treat hyperprolactinaemia. Cabergoline has the most favourable profile in terms of efficacy and tolerability as well as a long plasma half-life that enables once- or twice-weekly administration. Dopamine agonists are effective in over 80% of cases in normalizing the prolactin levels and reverting anovulation related to hyperprolactinaemia. Side effects include nausea, headache, postural hypotension, and fatigue.
Thyroid dysfunction
Clinical thyroid disorders, subclinical thyroid dysfunction, and thyroid autoimmunity have all been linked to poor outcomes following fertility treatment and pregnancy. The prevalence of positive thyroid peroxidase antibodies is higher in infertile women and can increase the risk of spontaneous miscarriage following IVF treatment (RR 1.99; 95% CI 1.42-2.79; P systematic review has found that IUI does not increase the probability of pregnancy when compared to timed intercourse (OR 4.57; 95% CI 0.21-102) (60). Undergoing ovarian stimulation prior to IUI (stimulated IUI) has also not been found to increase the pregnancy rate (OR 1.68; 95% CI 1.00-2.82) or live birth rate (OR 1.34; 95% CI 0.77-2.33) compared to IUI alone (60). IUI is less invasive than IVF and evidence from the same review based on two randomized trials has shown no difference in the live birth rate when comparing IVF versus IUI in cycles with ovarian stimulation (two randomized controlled trials, 86 couples: OR 1.03; 95% CI 0.43-2.45) (60).
Erectile dysfunction
The mainstay of treatment for erectile dysfunction is phosphodiesterase type 5 inhibitors including sildenafil, tadalafil, vardenafil, and avanafil. They act by causing vasodilatation secondary to release of cyclic GMP and administration is through the oral route. Side effects could include changes in vision, sense of smell, vascular tone, or platelet aggregation due to cross-reaction with multiple different phosphodiesterase receptors. Alprostadil is the injectable alternative to the oral medications and at doses of 10-20 mcg induces erections in up to 80% of patients. A surgical approach in the form of micro- vascular arterial bypass penile revascularization or penile implant is reserved for cases refractory to medical management.
Ejaculatory disorders
Disordered ejaculation can present as premature ejaculation, delayed ejaculation, or anejaculation. A combination of behavioural psychotherapy and serotonin reuptake inhibitors (SSRI) including paroxetine, fluoxetine, sertraline, citalopram, and fluvoxamine are used in the management of premature ejaculation. Dapoxetine is a purpose-built SSRI for on-demand treatment of premature ejaculation as it has a short half-life and can be used 1-3 hours before planned intercourse. Alternative medications prescribed are topical lignocaine, phosphodiesterase inhibitors, or tamsulosin. Psychotherapy is the mainstay of treatment for delayed ejaculation. Anejaculation or retrograde ejaculation is difficult to treat and pharmacological treatment has limited success. Sperm can be recovered from urine in cases of retrograde ejaculation to be used in IVF/ICSI cycle. Electro-ejaculation for sperm recovery could be considered in men with anejaculation due to neurological impairment. The option of surgical sperm retrieval remains if other measures are unsuccessful.
Assisted conception for male factor infertility
The introduction of ICSI technique for fertilization in the early 1990s has revolutionized the management of male infertility cases with very low sperm count and motility as it allows injection of a single sperm per egg to achieve fertilization. The focus is now shifting towards using it in non-male factor infertility despite not being supported by evidence.
The main concerns regarding the ICSI technique are the invasive nature of procedure, lack of an effective method for selecting sperm for injection, and the risk of genetic defects in the offspring. The latter has now been attributed to underlying genetic abnormality in the male partner and the overall health of the babies born following ICSI has been found to be satisfactory.
Management of unexplained infertility
The majority of couples with unexplained infertility can expect to become pregnant without active fertility treatment. An observational Dutch study found that 81% (356/437) of couples with unexplained infertility had an ongoing pregnancy within 5 years of diagnosis, with 74% (263/356) pregnancies being conceived spontaneously (41).
Accurate prediction of the prognosis of natural conception in these couples is useful in counselling and avoiding unnecessary treatment (61). A popular prediction model (62) has identified female age of less than 35 years, duration of infertility less than 2 years, and secondary infertility as good prognostic factors which favour higher odds of spontaneous conception.
Expectant management
Expectant management is recommended as a first-line strategy in couples with a good prognosis for natural conception. Expectant management is cost-effective compared to active treatment (63). The period of expectant management needs to take into account the age of the female partner, duration of fertility, and the couple's preferences. The United Kingdom National Institute for Health and Clinical Excellence guidance suggests waiting for a period of 2 years before moving on to active treatment (10).
Clomiphene citrate
Oral clomiphene citrate therapy has been empirically used for the management of unexplained infertility. It is thought to correct subtle ovulatory dysfunction. Clomiphene has been popular because it is inexpensive compared to other fertility treatments, is non-invasive, and needs less clinical monitoring.
However, studies comparing clomiphene with expectant management have shown a comparable live birth rate (OR 0.79, 95% CI 0.45-1.38) (66) and less cost-effectiveness (63) suggesting no overall benefit with clomiphene use. A Cochrane review has also shown no improvement in pregnancy rates (64).
Intrauterine insemination
IUI is another commonly used management approach which theoretically allows sperm to avoid any hostile cervical factors and increases the number of motile sperm within the upper genital tract around the time of ovulation in a natural or stimulated cycle. IUI in an unstimulated (natural) cycle involves monitoring urinary or serum LH from day 10 to day 12 of the treatment cycle to detect an LH surge. Insemination is performed 20-30 hours after detection of an LH surge. In stimulated cycles, clomiphene or gonadotropins is used to promote ovulation from more than one (ideally two) mature follicles. Human chorionic gonadotropin is administered to trigger ovulation and IUI is scheduled 36-40 hours later.
Unstimulated IUI is not clinically effective (65) or cost- effective (63) when compared to expectant management and may result in lower live birth rates in comparison to stimulated IUI (66). Stimulated IUI has a risk of multiple pregnancy almost similar to IVF with a single embryo transfer or IVF cycles using a low dose of gonadotropins for ovarian stimulation (modified natural cycle IVF) (67).
In vitro fertilization
The rationale of IVF in unexplained infertility is that it is able to bypass known as well as unknown barriers to conception, but it is an invasive and more expensive procedure compared to IUI with a risk of multiple pregnancy and hyperstimulation. A primary strategy of offering IVF straight after a period of expectant management has demonstrated a shorter time to pregnancy and higher per-cycle pregnancy rates compared to treatment with oral agents or gonadotropins in patients with unexplained infertility (68). However, no conclusive difference in the live birth rates have been seen in women undergoing IVF as a primary treatment, when compared to stimulated IUI regardless of whether clomiphene or gonadotropin was used for stimulation (69).
Management of endometriosis
Minimal/mild endometriosis
Medical treatment options for mild and minimal endometriosis include progestogens, combined oral contraceptive pill, danazol, and GnRH agonists. These drugs suppress ovulation and none is effective in terms of improving pregnancy rates when compared to a placebo or expectant management (70). However, they are helpful in alleviating the symptoms of pain. Laparoscopic ablation/excision of minimal to mild endometriosis can increase live birth rates (71). IUI with controlled ovarian stimulation is an alternative option for these women with potential to increase the pregnancy rates compared to expectant management or IUI alone (72).
Ovarian endometriomas
Ovarian endometriomas can be managed surgically by aspiration or cystectomy. The latter has been shown to be associated with increased spontaneous pregnancy rates when compared with aspiration (73). Women with endometriomas should be counselled regarding the risks of reduced ovarian function after surgery and the possible loss of the ovary (72). Surgery should therefore be offered only for symptomatic large endometriomas (>4 cm) or when there is a suspicion of malignancy (74).
Moderate/severe endometriosis
Women with moderate or severe endometriosis are usually considered for laparoscopic excisional surgery to increase the chances of spontaneous conception and improvement in symptoms. Early referral for IVF is considered due to concern about compromised ovarian and tubal function. Hypothalamic- pituitary downregulation for 3-6 months with a GnRH agonist prior to IVF has been shown to increase the odds of clinical pregnancy (75). Pregnancy rates for women with endometriosis-related infertility after IVF are, however, lower than those with tubal factor infertility (OR 0.56; 95% CI 0.44-0.70) (76).
Assisted conception
IVF is the recommended treatment for couples with prolonged unresolved infertility unresponsive to other forms of treatment. The process includes controlled ovarian hyperstimulation, pituitary downregulation, and an ovulation trigger followed by surgical oocyte retrieval. Retrieved eggs are fertilized in the laboratory using sperm from the male partner and cultured in incubators to create embryos which are subsequently transferred to the uterine cavity. Complications associated with IVF include ovarian hyperstimulation syndrome and multiple pregnancies.
Despite technological improvements over time, the live birth rate per fresh IVF cycle is just under 30% (77). The outcome is enhanced by replacement of frozen embryos, where available, and by repeated attempts in women who are able to respond to stimulation. The chance of a live birth after three complete cycles of IVF reaches 42.3% (78). Cumulative live birth rates have been shown to increase to 65.3% (95% CI 64.8-65.8%) by the sixth cycle (77) and up to 83% by the eighth cycle (78). Older women with a longer duration of infertility and no previous pregnancies have a bleaker prognosis. Poor performance over one or more cycles is the main reason for medical advice against continuing further treatment. Psychological distress following unsuccessful attempts and financial pressures are other common reasons for discontinuing treatment.