Lifestyle factors influencing fertility
Age and fertility
Female age is the most important factor affecting the probability of achieving a conception due to its impact on the quantity and quality
Table 51.1 Types of infertility
| Type | Definition | Prevalence (95% CI) 31-50 years age, n = 4466 12 months' duration | Prevalence (95% CI) 31-50 years age, n = 4449 24 months' duration |
| Primary | Inability to achieve a conception | 10.5 (9.5-11.4) | 5.9 (5.2-6.6) |
| Secondary | Inability to conceive after having achieved a pregnancy before | 5.3 (4.7-6.0) | 2.9 (2.4-3.4) |
| Primary and secondary | Combination of above | 1.7(1.3-2.0) | 0.3 (0.2-0.5) |
of the oocyte/follicle pool.
Women reach their peak reproductive potential in their 20s. A gradual decline in fertility is observed after the age of 30 which becomes more pronounced after 35 years of age (Figure 51.1) (12).In contrast to gonadal function in women, sperm production in men continues through life. However, sperm quality can deteriorate as men get older which, along with a decrease in sexual activity, is thought to be responsible for reduced fertility in men over the age of 40 years (13).
Body mass index
Obesity can have a huge impact on both male and female fertility. In women, extremes of body weight, including low body mass index (BMI) (30 kg/m2), can result in hormonal and ovulatory dysfunction. Overweight (BMI ≥25-29.9 kg∕m2) and obese (BMI ≥30 kg∕m2) women undergoing IVF treatment have a reduced chance of pregnancy (relative risk (RR) 0.84; P = O.OO02) and a higher chance of miscarriage (RR 1.31; P (HSG), three-dimensional transvaginal scanning, saline infusion sonography, MRI, and hysteroscopy can all aid in confirming the diagnosis in these cases.
Ultrasound scanning of ovaries is useful for assessing antral follicle count as a marker for ovarian reserve. It also facilitates diagnosis of ovarian cysts, polycystic appearance of the ovary, and gaining information about the accessibility of the ovaries for transvaginal egg retrieval should IVF treatment be necessary.
Local examination: male partner
Examination of the male genitalia is helpful in cases with oligozoospermia or azoospermia. The location and volume of the testicles and any associated lumps should be noted. Reduced testicular volume (51.3 Example of a hysterosalpingogram.
Abnormalities in semen analysis
• Oligozoospermia: a sperm count below 15 million/mL is described as oligozoospermia and is often associated with poor sperm motility and morphology. In the majority of cases, the cause of oligozoospermia is unknown (idiopathic). The other known associations are illustrated in Figure 51.4.
• Azoospermia: absence of sperm in the semen sample can be due to problems with the sperm production (non-obstructive azoospermia) or the sperm transport (obstructive azoospermia). The causes linked to azoospermia are illustrated in Figure 51.5.
• Asthenozoospermia (reduced sperm motility): the WHO grading of sperm motility is from grades a to d implying a range from fast progressively motile to fully immotile sperm. The criteria for normal motility takes into account grade a (swimming fast in a straight line) and grade b (slightly slower moving in a curved line) sperm which should be 32% of the total sperm seen. Motility of the sperm is regulated by calcium pathway and influenced by reactive oxygen species, cell osmolality, and function of the flagellar
Table 51.3 Pros and cons of tubal patency assessment procedures
| Test | Pros | Cons |
| Hysterosalpingogram (HSG) | Minimally invasive Less costly Flushes tubes and relieves minor blockage Can provide additional information about uterine cavity anomalies | Radiation exposure Sensitivity to methylene blue dye Pelvic infection False-positive report in case of tubal spasm Doesn't allow assessment of pelvic cavity |
| Hysterosalpingo contrast sonography (HyCoSy) | Minimally invasive Avoids radiation exposure Can provide additional information about uterine cavity anomalies Allows assessment of ovaries and other pelvic pathology | Expensive—catheters and contrast foam False positive due to tubal spasm Poor ultrasound views due to bowel gas shadow or high BMI |
| Laparoscopy and dye test | Definitive test Allows assessment of pelvic cavity and additional procedures as necessary | Invasive Need for general anaesthesia Expensive Risk of injury to blood vessels, bladder, and bowel |
components (33).
Underlying genetic factors which are poorly understood and lifestyle factors can affect these mechanisms resulting in poor sperm motility (33)• Teratozoospermia: samples from infertile men are likely to show a higher proportion of abnormally shaped sperm, including abnormalities of the head, acrosome, midpiece, or tail. These may be associated with genetic, lifestyle, and environmental factors but the cause remains unexplained in the majority of cases. It has been proposed that the type of morphological abnormality is more important than the proportion of abnormal forms and a recent study has attempted to establish the reference ranges for morphological abnormalities in population of fertile and infertile men (34).
Further investigations in male factor infertility
Hormonal profile
Measurement of FSH, LH, testosterone, and prolactin may be helpful in identifying the underlying cause in men with significant
Table 51.4 World Health Organization criteria for semen quality
| Parameter | Normal value (lower limit of reference range) |
| Volume | 1.5 mL |
| Concentration (number of sperm per mL of semen) | 15 million/mL |
| Progressive motility (per cent swimming forward) | 32% |
| Morphology (per cent of normal shapes) | 4% |
Source data from Cooper TG, Noonan E, von Eckardstein S, Auger J, Baker HW, Behre HM, Haugen TB, Kruger T, Wang C, Mbizvo MT, Vogelsong KM. World Health Organization reference values for human semen characteristics. Reprod Update 2010;16(3):231-45.
oligozoospermia or azoospermia. High FSH levels suggest defective testicular sperm production while low FSH levels indicate a hypothalamus- or pituitary-related cause. Testosterone levels can be low due to a primary testicular cause or due to exogenous androgen abuse. Early- morning testosterone levels should be repeated for confirmation.
Hyperprolactinaemia is associated with oligozoospermia or sexual dysfunction and therefore persistently raised prolactin levels should be investigated further with a pituitary MRI scan to rule out prolactinomas.Genetic and chromosomal tests
Azoospermia or severe oligoasthenozoospermia can stem from a genetic cause such as sex chromosomal aberrations or specific gene defects. Karyotype abnormalities found in some infertile men include Klinefelter syndrome, where an additional X chromosome is present (47XXY), or a 46XX male phenotype.
Microdeletions of genes from the azoospermia factor (AZF) region of the long arm of the Y chromosome which provides instructions for spermatogenesis can be tested for counselling azoospermic men prior to surgical sperm retrieval and intracytoplasmic sperm injection (ICSI) treatment. Deletions found in the AZFa and AZFb regions suggest the possibility of a poor chance of sperm recovery during sperm retrieval, whereas those in the AZFc region are associated with a good chance of sperm recovery. These microdeletions could be transmitted through ICSI to the male offspring.
Azoospermia can also be associated with Kallman syndrome which is X-linked and results from failure of gonadotropin-releasing hormone (GnRH) neuron migration to the hypothalamus. Ciliary dyskinesia (autosomal recessive dynein deficiency in the sperm flagellum) can be associated with asthenozoospermia and myotonic dystrophy (autosomal dominant) can present as oligozoospermia.
Cystic fibrosis screening
The finding of a bilateral absence of vas deferens on examination of male genitalia should prompt screening for cystic fibrosis. In these cases there is reduced expression or increased mutation in the cystic fibrosis transmembrane regulator gene (CFTR) which plays an important role in regulating spermatogenesis.
Antisperm antibodies
The presence of sperm agglutination on routine semen analysis is an indication for antisperm antibody testing. The commonly used techniques are the mixed agglutinin reaction and the immunobead test, which use red blood cells or beads coated with immunoglobulin (Ig)-A/IgG antibodies to detect sperm containing the antisperm antibodies.
Sperm DNA fragmentation
Testing for DNA damage in sperm is not performed routinely and tests report on the percentage of sperm with DNA damage expressed as the sperm DNA fragmentation index (DFI). The damage to sperm DNA can be due to reactive oxygen species or due to an intrinsic defect in the process of spermatogenesis that makes the sperm more prone to damage. DNA fragmentation has been shown to be associated with an increased risk of birth defects, increased miscarriage rates, and reduced fertilization and implantation during IVF. However, evidence regarding this is conflicting. Also, there is a lack of consensus about appropriate cut-off values and effective interventions.
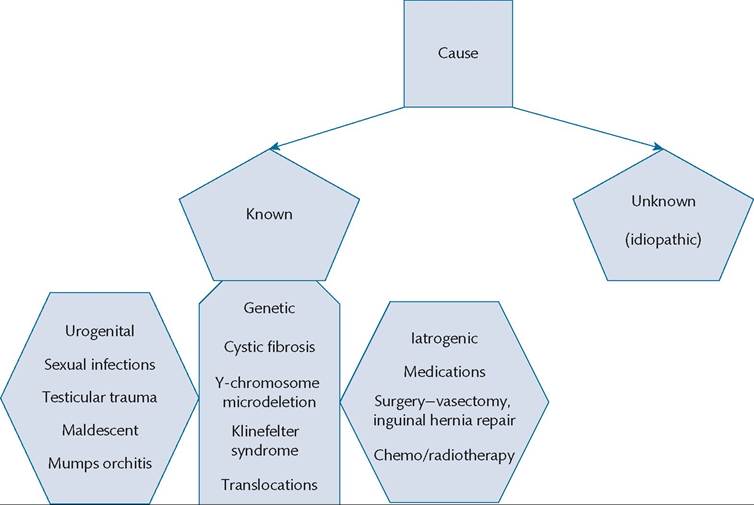
Figure 51.4 Aetiology of male infertility.
Lifestyle/environmental factors
Smoking
Endocrine disruptors-phthalates
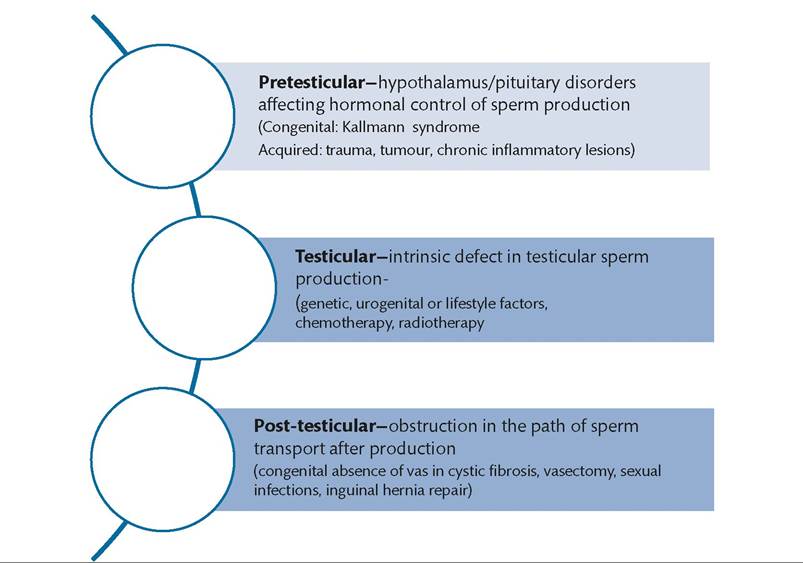
Figure 51.5 Causes of azoospermia.
Male genital tract imaging
Vasography is a means of assessment for finding the site of obstruction in obstructive azoospermia cases. Its use has gone out of fashion due to better techniques for surgical sperm retrieval and establishment of ICSI. Ultrasound scanning is useful in case of suspected testicular tumours and varicoceles. Venography provides accurate assessment of varicoeles but due to the invasive nature, it is used only for intended treatment and not for diagnostic purposes.
Additional investigations in the female partner
Ovarian reserve tests
The tests in current use include early follicular phase FSH level (between days 1 and 5 of the menstrual cycle), measurement of antral follicle count (AFC), and serum anti-Mullerian hormone (AMH) levels. AFC and AMH are considered to be good predictors of the ovarian response to controlled hyperstimulation used as part of IVF treatment but are poor predictors of pregnancy.
Basal FSH levels in women with regular cycles can be used as a screening test to predict the response to ovarian stimulation but the prediction is accurate only at higher levels (35).
AFC is done by means of transvaginal ultrasound scanning and best done in the follicular phase of cycle. Two-dimensional ultrasonography is used in routine practice but three- dimensional ultrasonography has also been shown to be helpful. Antral follicles of 2-10 mm in diameter are measured to assess AFC. Ultrasound measurements are subject to intra- and inter-observer variability and are operator dependent. Women with an AFC less than four are 8.7 times more likely to have an unsuccessful outcome following IVF (95% CI 2.4-31.7) than women with an AFC of four or more (36). The sensitivity and specificity of AFC to predict cycle cancellation has been found to be 66.7% and 94.7%, respectively (37).
AMH is secreted by the granulosa cells of the antral and preantral follicles in the ovaries and therefore is a good means to assess the reserve of primordial follicle pool. Initiation of follicular recruitment in each cycle is controlled by AMH and levels decline thereafter with age. There is no variation in the levels during a menstrual cycle and therefore the test can be done at any time, which is an advantage compared to FSH. Several studies have reported AMH to be a better marker of ovarian reserve compared to other tests but this has not been fully established. Current clinical application of using AMH is to predict the response to ovarian stimulation in IVF treatment where sensitivity and specificity has been estimated to be 82% and 76% respectively (37). Other scenarios where AMH has been found to be useful are in predicting the age at menopause (38), predicting the ovarian reserve after chemotherapy or surgery, and as a screening test for PCOS. However, technical problems with earlier assays used for measurement of AMH have come to light and newer assays are continuing to evolve with further studies awaited on their reliability and validity. Also, there are no agreed standards regarding the reference ranges from the different assays.
Hysteroscopy
In cases where intrauterine pathology is suspected on pelvic ultrasound scan, assessment of the uterine cavity by means of hysteroscopy is considered the gold standard investigation with a sensitivity of around 98% (39).
Hysteroscopic removals of endometrial polyps, resection of submucosal fibroids, and division of intrauterine adhesions have the potential to increase the pregnancy rates in women with unexplained infertility prior to fertility treatment (40). Hysteroscopy has also been shown to improve pregnancy rates if done prior to IVF treatment in women with previous unsuccessful attempts (RR 1.7; 95% CI 1.5-2.0) (40).
Summary of investigations
Figure 51.6 outlines a systematic approach to investigations in an infertile couple. It is important to consider how the result of each test will contribute to subsequent clinical decision-making and also to balance the benefits against potential costs and invasiveness.