Evaluation of female urinary incontinence
A focused history, clinical examination, and urodynamic testing forms the basis of the assessment of a woman suffering from UI. Validated questionnaires such as the Bristol Female Lower Urinary Tract Symptoms (MBFLUTS) questionnaire and bladder diaries are usually administered prior to a consultation, to enable subjective assessment of the effect of symptoms on the patient's quality of life and to gauge its impact on bowel and sexual function.
History taking
History taking is a key element in the assessment of patients with UI and enables the clinician to tentatively categorize patients as having SUI, UUI, or MUI based on their symptoms. History also helps in assessing patients with stand-alone or associated voiding disorders. Typically, symptoms associated with SUI include leak on cough, sneeze, or high-impact physical exertion and occasionally with a change in posture and coital activity. Patients with UUI complain of frequency, nocturia, and urgency with or without incontinence. There may be an overlap of symptoms and occasionally urgency incontinence may be triggered by activities such as coughing and can mimic stress incontinence. Additional MUI is very common finding and it is therefore imperative that management be directed towards the predominant symptom (11). Voiding disorders manifest with symptoms of straining to void, slow and strained stream, misdirected urinary stream, and feeling of incomplete emptying (12). If, however, the patient complains of continuous leakage and extra-urethral urinary leakage loss, it may indicate urinary fistula and these symptoms need appropriate investigations. Women may complain of pelvic floor symptoms of vaginal or uterocervical prolapse in the form of a bulge at the vaginal introitus, vaginal fullness, double-voiding, needing to digitate the vagina to empty bowels, and sexual dysfunction.
Although pelvic floor disorders are frequently found in women who have delivered vaginally, it is not uncommon to find nulliparous women and those who have had elective caesarean births suffering from symptoms of UI. That being said, obstetric history, in particular the parity, mode of delivery, instrumental deliveries, associated vaginal trauma, and birth weight are some important risk factors. Equally, gynaecological conditions such as large fibroids and ovarian cysts may precipitate UI. The symptoms of UI worsen after menopause. In patients with voiding disorders it is not unusual to have a past surgical history of retropubic continence- enhancing operations such as the Marshall-Marchetti-Krantz or Burch colposuspension. Spinal surgery or complex colorectal surgeries in the past may also be relevant.
Chronic medical conditions, such as diabetes, connective tissue disorders, neurological disorders, in particular Parkinson's disease, multiple sclerosis, spinal cord injuries, and chronic obstructive airway disease should be ruled out. Medications such as diuretics, alpha-blockers, alpha-agonists, and so on may also contribute to lower urinary tract symptoms. Finally, it is important to enquire about the intake of caffeine, alcohol, and carbonated drinks.
Physical examination
A thorough physical examination should follow to elicit positive evidence to support a history of UI. Typically, this involves a general examination to establish body mass index and is followed by abdominal, pelvic, and rectal examinations. A focused neurological examination may be indicated in some patients; however, a quick assessment of sacral segments (S2-S4) is always performed by testing for reflexes such as the bulbocavernosus or the anal ‘wink’ reflex. Abdominal examination may reveal a mass; more often, abdominal scars may provide clues to previous surgery that may be relevant to the patient’s symptoms.
Local genital examination should commence, looking for signs of vaginal atrophy or evidence of maceration of vulval tissues secondary to urinary leakage.
Demonstration of urinary leak preferably in the supine and standing positions should follow this and one should look for signs of vaginal/uterocervical prolapse. A large anterior (or occasionally posterior) vaginal prolapse may produce a relative obstruction of the urethra that can impair bladder emptying. Paradoxically, a posterior vaginal wall prolapse may splint the bladder neck and mask SUI; compressing the prolapse may uncover ‘occult’ incontinence.Investigations
Urinalysis
Urine microscopy, culture, and sensitivity testing should be performed in all cases to determine if there is any evidence of haema- turia, pyuria, glycosuria, or proteinuria. Urinary tract infections and evidence of bladder cancer should be tested for before proceeding with further investigations.
Assessment of residual urine
Measurement of post-void residual urine volume by ultrasonography can test for a bladder-emptying abnormality or incontinence associated with chronic urinary retention. A post-void residual urine volume of 50 mL or less is considered normal and above 200 mL merits further investigation.
Imaging
An ultrasound scan of the urinary tract to demonstrate the anatomy of the kidney, ureter, and bladder should be ordered; a pelvic ultrasound may be ordered to confirm/exclude pelvic pathology such as fibroids or ovarian cysts. Occasionally a computed tomography scan or magnetic resonance imaging may be necessary.
Overview of urodynamics
Urodynamic testing involves an objective assessment of the storage, contractile, and voiding function of the bladder (Figure 57.3). In some centres a flexible cystoscopy is also performed. Only the procedure is described here, as a discussion of findings on urodynamics and the pros and cons of this procedure is outside the scope of this chapter.
Uroflowmetry is the first part of urodynamic assessment, and in most centres is done within the privacy of the toilet because the environment within the urodynamics laboratory is not always conducive, and ‘stage fright’ may affect results.
This test requires the patient with her bladder comfortably full to void into a calibrated flowmeter. The recorded parameters during the test include:• flow rate, which is the volume of urine voided via the urethra per second
• voided volume, which is the total volume expelled via the urethra
• maximum flow rate, which is the maximum measured value of the flow rate
• flow time, which is the time over which measurable flow occurs
• average flow rate, which is the volume voided divided by voiding time.
Based on the patterns elicited, this test is a useful adjunct to diagnosing voiding disorders (13).
Cystometry produces a cystometrogram that demonstrates the pressure-volume relationship of the bladder. This test comprises filling, voiding, and urethral phases, and is designed to reproduce patients’ symptoms (i.e. their bladder function in a laboratory environment). Not uncommonly this test may reveal asymptomatic bladder dysfunction; it is also a useful tool to objectively assess postoperative success/failure. The patient’s sensation of bladder filling, first desire to void, strong desire to void, urgency/pain are recorded while the cystometrogram plots the corresponding pressures. The test involves the insertion of a urethral catheter (filling catheter typically with an integrated pressure sensitive tip) to measure vesical pressures and a vaginal/rectal catheter to measure the abdominal pressures. The difference, that is, vesical pressure minus abdominal pressure, gives the detrusor pressure. The detrusor pressure is sometimes measured during voiding; however, its value in detecting obstructive pathology in females is limited. Cystometry is useful for distinguishing SUI from UUI caused by bladder overactivity. It is particularly useful in patients with MUI, where the management, medical or surgical, may be determined on the predominant finding. The final assessment is the measurement of the urethral pressure profile (measured in mmHg) or the Valsalva leak point pressure in cm of H2O.
UPP may be useful in diagnosing a deficiency in urethral function which is proposed as the primary mechanism for SUI. Its role in determining the need for or the type of surgery remains controversial. Patients with low Valsalva leak point pressure/maximum urethral closure pressure are said to have intrinsic sphincter deficiency, as opposed to the majority of patients with SUI who have urethral hypermobility as the primary cause of their leakage (13).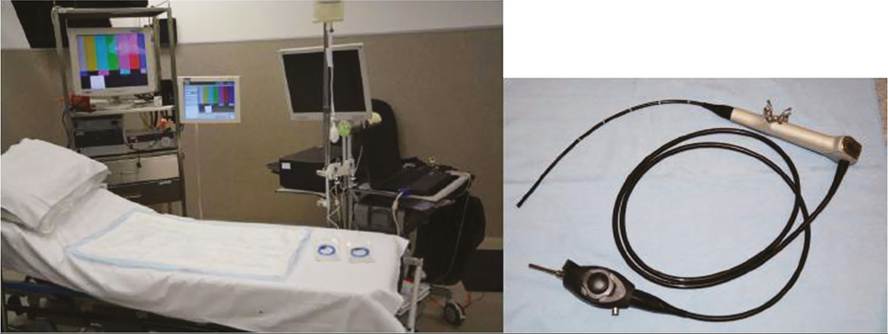
Figure 57.3 Urodynamics and flexible cystoscopy set-up.
Cystoscopy
Usually an optional evaluation, cystoscopy is routinely offered in some units as a part of urodynamic testing. The procedure is definitely indicated when a patient has microscopic or overt haematuria, has a painful bladder, previous bladder injury, radiation, and previous surgery with mesh or tape. It is also useful if a urethral stricture, urinary fistula, or diverticulum is suspected.